Multimodal Scar Management
Rei Ogawa
KEY POINTS
Keloids and hypertrophic scars (HSs), which result from abnormal healing of injured or irritated skin, are red, elevated scars that have an unappealing appearance and are associated with intermittent pain, persistent itching, and a sensation of contraction.
It is possible that HSs and keloids are manifestations of the same fibroproliferative skin disorders, which are graded according to the intensity and period of inflammation and influenced by genetic, systemic, and local factors.
Steroid injections have long been a first-line therapy; however, over the past decade, many studies have examined different approaches to the treatment and management of keloids/HSs. A multimodal approach is often required for optimal results, both in combination on the same treatment day and on alternating visits.
Keloids and HSs are now regarded as treatable diseases. However, the therapeutic approaches still require improvement if they are to be truly successful from both a physiologic and an aesthetic perspective. This chapter will provide one expert’s perspective on multimodal pathologic scar management.
Keloids and hypertrophic scars (HSs) are caused by abnormal healing of injured or irritated skin.1 These red, elevated scars have an unappealing appearance and are associated with intermittent pain, persistent itching, and a sensation of contraction. Inflammation is continuous and local. Moreover, some keloids can discharge pus because of the presence of infected inclusion cysts. Many classical textbooks consider keloids and HSs to be completely different scar types. Clinicians define HSs as scars that do not grow beyond the boundaries of the original wound, whereas keloids spread into the surrounding normal skin. By contrast, pathologists make a histologic distinction between keloids and HSs based on the presence of thick eosinophilic (hyalinizing) collagen bundles, called “keloidal collagen,” which are present in the former but absent from the latter (see Chapter 5). However, there are many cases in which a scar bears the growth and histologic features of both HSs and keloids. Indeed, it is possible that HSs and keloids are manifestations of the same fibroproliferative skin disorders,2 which are graded according to the intensity and period of inflammation, which in turn are influenced by genetic, systemic, and local risk factors.3
Pathogenesis of Keloids and HSs
Various genetic, systemic, and local factors influence the quality and quantity of keloids and HSs. Genetic links to pathologic scar development may involve single-nucleotide polymorphisms (SNPs). A genome-wide association study4 and our own research5 show that four SNP loci in three chromosomal regions are significantly associated with keloid development in the Japanese population. There are probably many other genetic factors that are still not known.
In terms of systemic factors, adolescence and pregnancy appear to be associated with a higher risk of developing pathologic scars. It may be that sex hormones such as estrogens and androgens have vasodilatory effects that intensify inflammation and make keloids and HSs worse. According to our unpublished data, the rate of occurrence of keloids not caused by trauma suddenly increases around 10 years of age; thus, we consider that increases in the levels of sex steroids at the start of adolescence are responsible for the higher risk of pathologic scar development in adolescents, rather than increases in the likelihood of trauma. Moreover, our recent study revealed that hypertension is associated with the development of severe keloids.6 Hypertension may damage the blood vessels, thereby increasing inflammation in scar tissue.
However, we believe that mechanical forces play a particularly important role in the pathophysiology of keloids and HSs (see Chapter 7).7,8 Keloids show a marked preference for particular locations on the body and commonly adopt distinct site-specific shapes. The typical butterfly, crab’s claw, or dumbbell shapes of keloids appear to be largely determined by the direction of the tension applied to the skin around the wound site.7,8,9 Moreover, keloids usually
occur at sites that are constantly or frequently subjected to tension (such as the anterior chest and scapular regions), but seldom in areas where stretching/contraction of the skin is rare (such as the parietal region or anterior lower leg), even in patients who have multiple/large keloids. In the case of the earlobe, the contribution of mechanical factors may be minor, although friction against the pillow and the weight of the keloid itself can induce keloids. Furthermore, repeated attaching and detaching of piercings may lead to repeated injury and infection, which are triggers of persistent inflammation.
occur at sites that are constantly or frequently subjected to tension (such as the anterior chest and scapular regions), but seldom in areas where stretching/contraction of the skin is rare (such as the parietal region or anterior lower leg), even in patients who have multiple/large keloids. In the case of the earlobe, the contribution of mechanical factors may be minor, although friction against the pillow and the weight of the keloid itself can induce keloids. Furthermore, repeated attaching and detaching of piercings may lead to repeated injury and infection, which are triggers of persistent inflammation.
Although physicians cannot (or at least find it very difficult to) control genetic and systemic factors, they can reduce the mechanical forces around keloids and HSs; this can be achieved using various surgical techniques (including Z-plasties). Moreover, anti-inflammatory treatments such as corticosteroids or anti-angiogenesis agents (which reduce the number of blood vessels) are viable clinical strategies.
Prevention of Keloids and HSs
A burn wound that heals in less than 10 days has a 4% risk of developing into a HS, whereas a burn wound that takes 21 days or more to heal has a 70% (or greater) risk of developing into a HS.10 This means that a deep skin injury that extends to the reticular layer of dermis needs time to heal; however, if inflammation continues for a long period, then the risk of developing a pathologic scar increases. Histopathologic examination of pathologic scars reveals that the epidermis and the papillary layer of the dermis are almost normal, except for minor inflammation, but the reticular layer shows strong inflammation with an increase in the number of blood vessels and nerve and collagen fibers.1,3
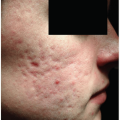
Thus, speedy wound healing is essential to prevent the formation of pathologic scars. Keloids can arise from very small injuries or from irritated skin (e.g., acne, herpes zoster, insect bites, and skin injections). This means that special care should be taken when treating patients with a history of keloids.
Stretching of a wound risks evoking inflammation of the dermis; thus, wounds should be stabilized as soon as the exudate from the wound surface has stopped. Silicone tape is better than paper tape as its use prevents epidermal injury caused by repeated taping. Moreover, silicone tape keeps the scar surface moist. These tapes can be kept in place until they detach naturally. The patient does not need to change the tape after taking a bath/shower. In the experience of the author, patients can keep a tape in place for about 1 to 2 weeks, except in summer when perspiration can reduce tape adherence.
If the patient has a clear history of pathologic scars, then the stabilization tape should be exchanged for steroid plaster/tape at about 1 month after epithelialization. Flurandrenolide tape (Cordran tape), fludroxycortide tape (Drenison tape), and deprodone propionate tape (Eclar plaster) are available worldwide. These steroid tapes/plasters should be changed every 24 to 48 hours, and should be cut so that they just cover the wound, with minimal attachment (if any) to healthy skin (unpublished data).
Treatment of Keloids and HSs
Over the past 10 years, our understanding of the pathogenesis of keloids and HSs has increased markedly.11 Thus, keloids and HSs are now regarded as treatable diseases. However, the available therapeutic approaches, which include surgery, radiation, corticosteroids, laser therapy, and makeup therapies, still require improvement, and combinations of these modalities may be required for optimal results.
Surgery
Surgical treatment can result in recurrence of keloids and HSs, which are then often much bigger than the original lesions. Thus, careful consideration is necessary for anything other than minor HSs. Radiation therapy after surgery markedly reduces the risk of recurrence; however, the recurrence rate can also be reduced by using particular surgical techniques; namely, subcutaneous/fascial tensile-reduction sutures, Z-plasties, and local flap transfer.
The use of subcutaneous/fascial tensile-reduction sutures relates to the fact that keloids and HSs arise from the dermis.8 Therefore, dermal sutures do not effectively reduce tension on the dermis. To achieve this, we need to access the much deeper structures (namely, the superficial and deep fascia) and suture them (Fig. 16-1). This type of suturing will elevate the wound edges smoothly, with minimal tension on the dermis. In other words, the wound edges will naturally attach to each other. Only then should dermal and superficial sutures be used. Dermal sutures should not be used as “tension-reduction sutures.” This is an important concept to prevent the formation of pathologic scars after surgery (Fig. 16-2). However, wedge excision should be the standard procedure for the earlobe12 (Fig. 16-3), and core excision13 should also be used for the cartilaginous part of the auricle.
Zigzag sutures, including Z-plasties, are good for releasing linear scar contractures and tension (see Chapter 12). A major benefit of Z-plasties is that segmented scars mature faster than long linear scars.14 In particular, if a scar crosses a joint, zigzag incision and suturing is important to reduce the risk of developing pathologic scars.
In addition, various local flaps are useful for releasing scar contractures. They are also important for preventing contractures because, unlike skin grafts, local flaps expand naturally after surgery. Because skin grafting tends to generate secondary contractures that result in circular pathologic scars around the grafted skin, flap surgery is generally better for keloids. In the past, keloid reconstruction with flaps was discouraged because it was thought that the donor site could itself develop keloids. However, the development of keloids at the donor site can be prevented by multimodal therapy, which includes tension-reduction sutures and radiation therapy. Thus, flap surgery may be considered a first-line treatment when dealing with keloids.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


