Excessive scarring represents a frequently observed medical problem around the world.
In addition to their bothersome appearance, hypertrophic scars and keloids are commonly associated with significant pain, pruritus, and functional impairment.
Despite a variety of currently available therapeutic approaches, treatment remains challenging.
Injection of 5-Fluorouracil for therapy-refractory keloids and the introduction of fractional laser therapy for the improvement of hypertrophic scars have significantly contributed to recent advances in this area.
levels of TGF-β1 and TGF-β2 promote an accumulation of ECM, whereas their degradation through decreased levels of TGF-β3 and matrix metalloproteinases (MMPs) is impaired. Both the severity of inflammation and the type of immune response predispose to excess scar formation.9 An increased TH2 response stimulates fibrogenesis, whereas a TH1 preponderance reduces tissue fibrosis.10,11
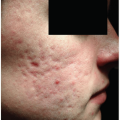
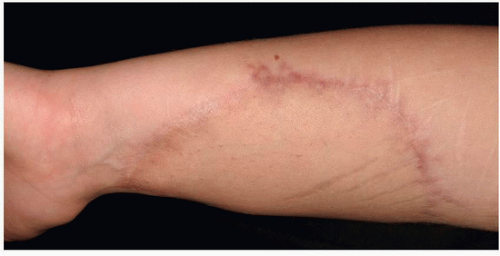 FIGURE 10-1 Immature scar with raised edges and erythema. |
 FIGURE 10-2 Physiological scar healing after surgery. (From Reinholz M, Poetschke J, Schwaiger H, et al. The dermatology life quality index as a means to assess life quality in patients with different scar types. J Eur Acad Dermatol Venereol. 2015;29(11):2112-2119.) |
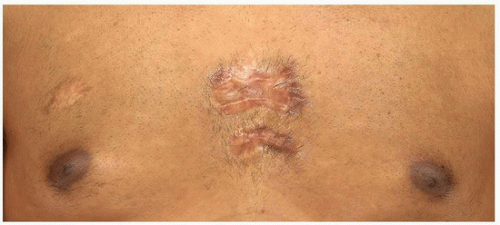 FIGURE 10-3 Spontaneous presternal keloid. |
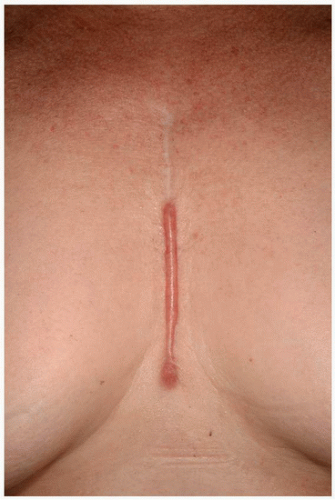 FIGURE 10-4 Hypertrophic scar after open heart surgery; the scar remains within the confines of the original injury. (From Reinholz M, Poetschke J, Schwaiger H, et al. The dermatology life quality index as a means to assess life quality in patients with different scar types. J Eur Acad Dermatol Venereol. 2015;29(11):2112-2119.) |
Table 10-1 Main Risk Factors for Hypertrophic Scars and Keloids | ||||||
|---|---|---|---|---|---|---|
|
Many of the therapeutic approaches available to date are being used for both prevention and treatment of excessive scarring.
Only a limited number of these strategies have been supported by controlled and well-designed prospective studies.
Differentiating between keloids and hypertrophic scars is crucial prior to any therapeutic manipulation because of augmented recurrence rates with keloids (Table 10-3).
Lasers continue to play an increasingly important role and are being marketed accordingly.
By utilizing basic options such as silicone sheeting/gel, intralesional triamcinolone acetonide (TAC), cryotherapy, or pressure, improvement can frequently be observed without any extensive cost for the respective patients.
Common prophylactic approaches in order to reduce the possibility of postoperative pathological scarring:
Delayed epithelialization beyond 10 to 14 days is well known to increase the incidence of hypertrophic scarring12; fostering rapid epithelialization is crucial to avoid excessive scar growth.
Wounds subjected to high tension due to motion, body location, or tissue loss are at increased risk of excessive scarring and spreading of scars (see Chapter 7). Patients undergoing surgery in these body areas should be aware of this significant risk prior to any surgery.13
The modern understanding of wound healing is based on the knowledge of restoring skin anatomy and function, and a thoughtful selection of suture materials and closure techniques. Surgical approaches should precisely coapt the tissue layers and margins. This is necessary to minimize new tissue formation within the wound. Suitable surgical closing techniques will also eliminate a potential cavity by approximating the subcutaneous tissue. If misalignment and dead space is minimized adjacent to the opposed wound edges, new tissue has limited room to grow. Atraumatic handling of tissue in combination with avoiding tight closures result in better aesthetic outcomes. Additionally, reduced tension on the wound margins facilitated by cautious undermining and loosening of the surrounding tissue contributes to better results. As an example, a combination of polydioxanone (PDS II, Ethicon Inc.) monofilament synthetic absorbable subcutaneous sutures (which provide extended wound support for up to 6 months) with absorbable sutures or Steri-Strip (3M) for optimal epidermal wound closure might be used. It has been shown that subcutaneous fascial tensile reduction sutures in a predisposed patient population, where the tension is placed on the layer of deep fascia and superficial fascia, revealed good clinical results. Here 2-0 or 3-0 PDS II sutures were preferred for subcutaneous/fascial sutures, and 4-0 or 5-0 PDS II sutures for dermal sutures.14
If hypertrophic scarring occurs, determining the optimal timing for procedural intervention (including surgical excision/revision) is key. Hypertrophic scars have the potential to mature over a year or more after injury and significantly flatten and soften without any medical intervention, potentially obviating the need for surgical excision.15 Nevertheless postexcisional relapse rates of the original hypertrophic scar are commonly negligible.16,17 On the other hand, if scar (joint) contractures occur, then invasive approaches that release contractures should be performed earlier (see Chapter 12).14
The development of hypertrophy is facilitated when there is an increased tension on wound margins. Consequently, employing surgical techniques such as Z- or W-plasty, grafts, or local skin flaps to interrupt the vicious circle between scar tension and scar thickening due to permanently stimulated ECM production may help mitigate pathological scar formation.18
Delayed would healing (e.g., after deep dermal burn or wound infection) may increase the risk of hypertrophic scars and keloids. Transforming selected lesions by surgery (excision with suture or graft) into a wound with appropriate healing time may reduce the risk of new excessive scar formation.18
If excessive scar tissue is surgically removed, a situation similar to a fresh wound is created. In this new setting disproportionate scarring might be reduced by adjuvant conservative therapy straight from the beginning.18 Nonetheless, the excision of keloids without any further conservative therapy (e.g., corticosteroid or 5-Fluorouracil [5-FU] injections, intrainterventional cryotherapy, pressure, or radiation) should be rigorously avoided because of a strongly elevated risk of recurrence (45% to 100%). The postexcision scar may even grow larger than the initial one in this new area of trauma.19,20 Remarkably good cosmetic results were obtained after a surgical repair approach (core excision with low-tension wound closure or shave excision) of earlobe keloids with postinterventional
corticosteroid or 5-FU injections, postoperative pressure (e.g., pressure earrings), application of imiquimod 5% cream or intraoperative cryotherapy on the incision site.21
Table 10-2 Hypertrophic Scars and Keloids: Current Therapeutic Strategies | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 10-3 Hypertrophic Scars and Keloids: Epidemiological, Clinical, and Histological Differences | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
100%, and recurrence rates vary from 9% to 50%.20 Side effects of corticosteroid injection include dermal atrophy, telangiectasia, and pain at the injection site. To improve the pain, topical anesthesia and/or regional injections of local anesthetics around the scars may be employed.5
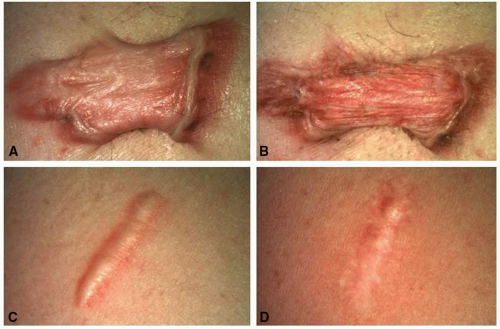 FIGURE 10-5 Keloids and hypertrophic scars after cryotherapy and triamcinolone acetonide (TAC) injections. A,C: Before treatment. B,D: After four sessions of cryotherapy and intralesional TAC injections (40 mg per mL). |
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


