Mandibular condyle fractures can result in short-term and long-term morbidity. As a weak area of the mandible, the condyle is vulnerable to injury by a direct impact or an indirect force. Current treatment recommendations aim to better match the severity of the fracture with the choice of closed or open approach. Long-term follow-up of patients provides the best opportunity to monitor the degree of functional restoration after treatment. There is a growing consensus regarding the use of standardized fracture classification methods and outcomes measures that will allow better assessment of treatment results and strengthen the quality of outcomes research.
Key points
- •
The condyle is a frequently fractured subsite of the mandible and the most frequently injured in children
- •
Standard outcomes measures should be recorded for all patients including opening, protrusion, lateral excursion, occlusion, chin deviation with opening, facial symmetry, pain, and TMJ derangement
- •
Patients with fractures with significant displacement, dislocation, or override with ramus shortening have the poorest prognosis for functional restoration when treated closed. These patients may best be served with open treatment
- •
Children younger than 12 years, even with displaced or dislocated fractures, have good functional outcomes with closed treatment
Introduction
The mandibular condyle is estimated to be involved in 25% to 45% of adult mandibular fractures. Up to 52% of mandibular fractures involve the condyle in the pediatric population. Most individuals sustaining condylar fractures are men and young, with average ages between 20 and 40 years, and an estimated 40% to 50% have a second fracture elsewhere in the mandible, often a contralateral parasymphyseal or body fracture. Bilateral condylar fractures may occur. , Fractures of the condyle may result from a direct blow to the condylar region or to another region of the mandible with the force transmitted to this weak area. Common causes of mandibular fractures include assault, motor vehicle accidents or falls, especially onto the chin as can occur during skateboarding and bicycle riding.
Anatomy and fracture classification
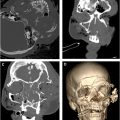
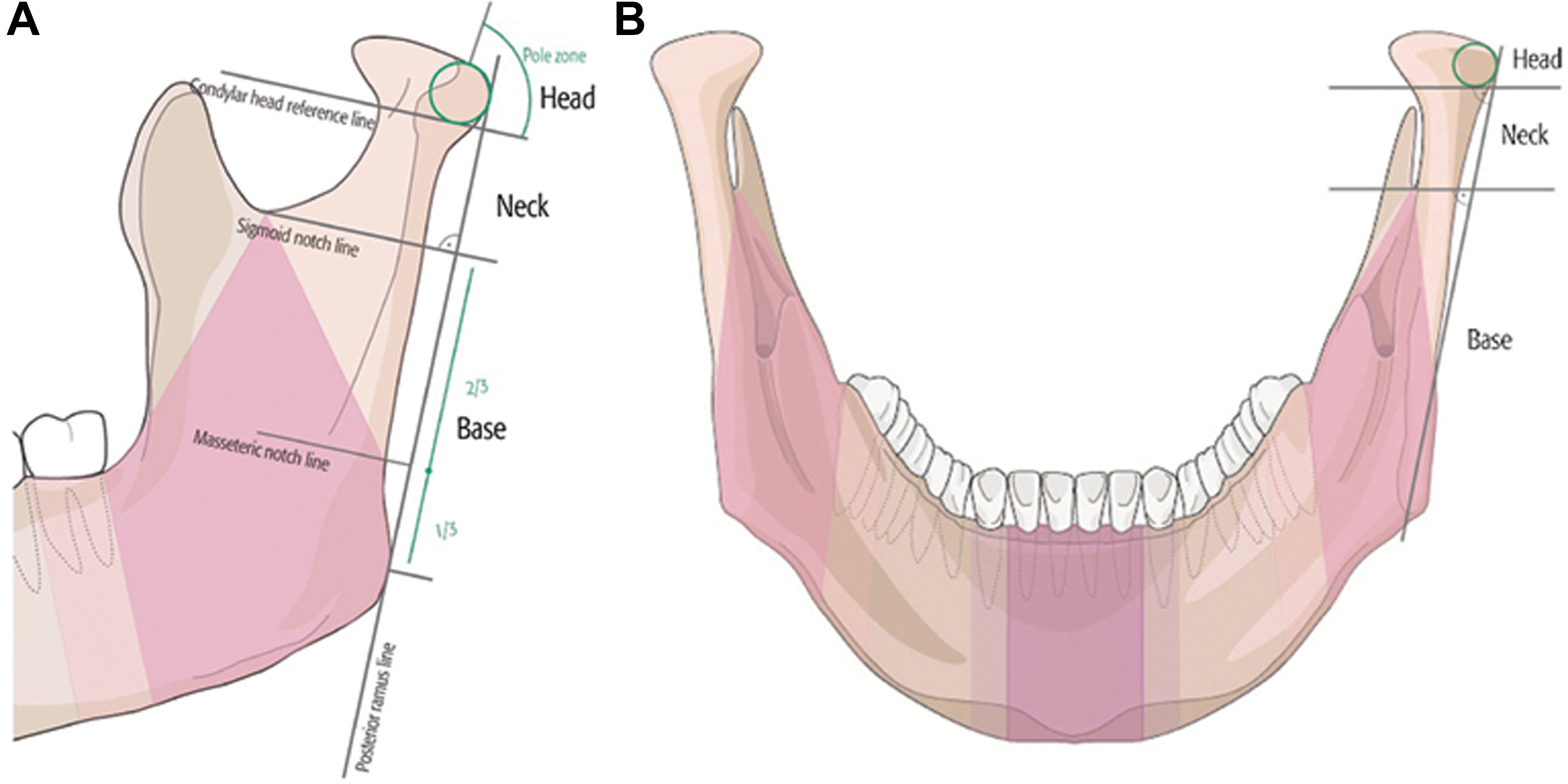
The condyle has 3 subsites: the condylar head, the condylar neck, and the subcondylar area. , ( Fig. 1 ) The condylar head is broad and rounded articulating in the glenoid fossa and completely surrounded by the temporomandibular joint (TMJ) capsule ( Fig. 2 ). At the inferior portion of the TMJ capsule, the condyle tapers to the region of the condylar neck and then widens at its attachment to the mandible forming the condylar base or subcondylar region.
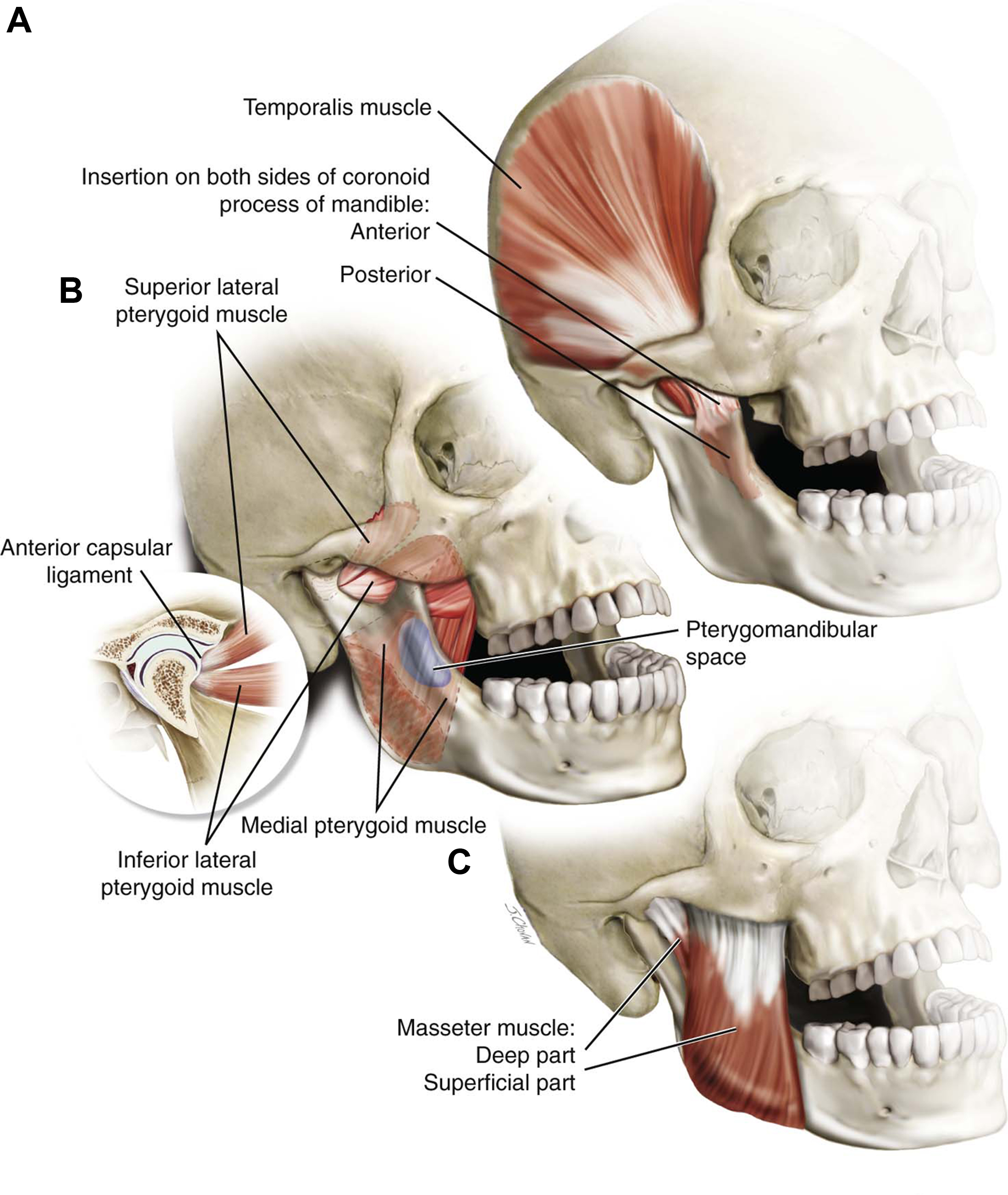
The TMJ functions as both a hinge and sliding joint, also known as ginglymoarthrodial, and is capable of opening, closing, left and right excursion, jaw protrusion, and retrotrusion. Left and right lateral excursion occur, by the pterygoid muscles pulling the mandible toward the contralateral side (ie, contraction of the right medial and lateral pterygoid muscles causes lateral excursion to the left; see Fig. 2 ). ,
Classification of condylar fractures should allow for clear communication among specialists and consist of an adequate number of domains to describe the fracture in several dimensions. ,
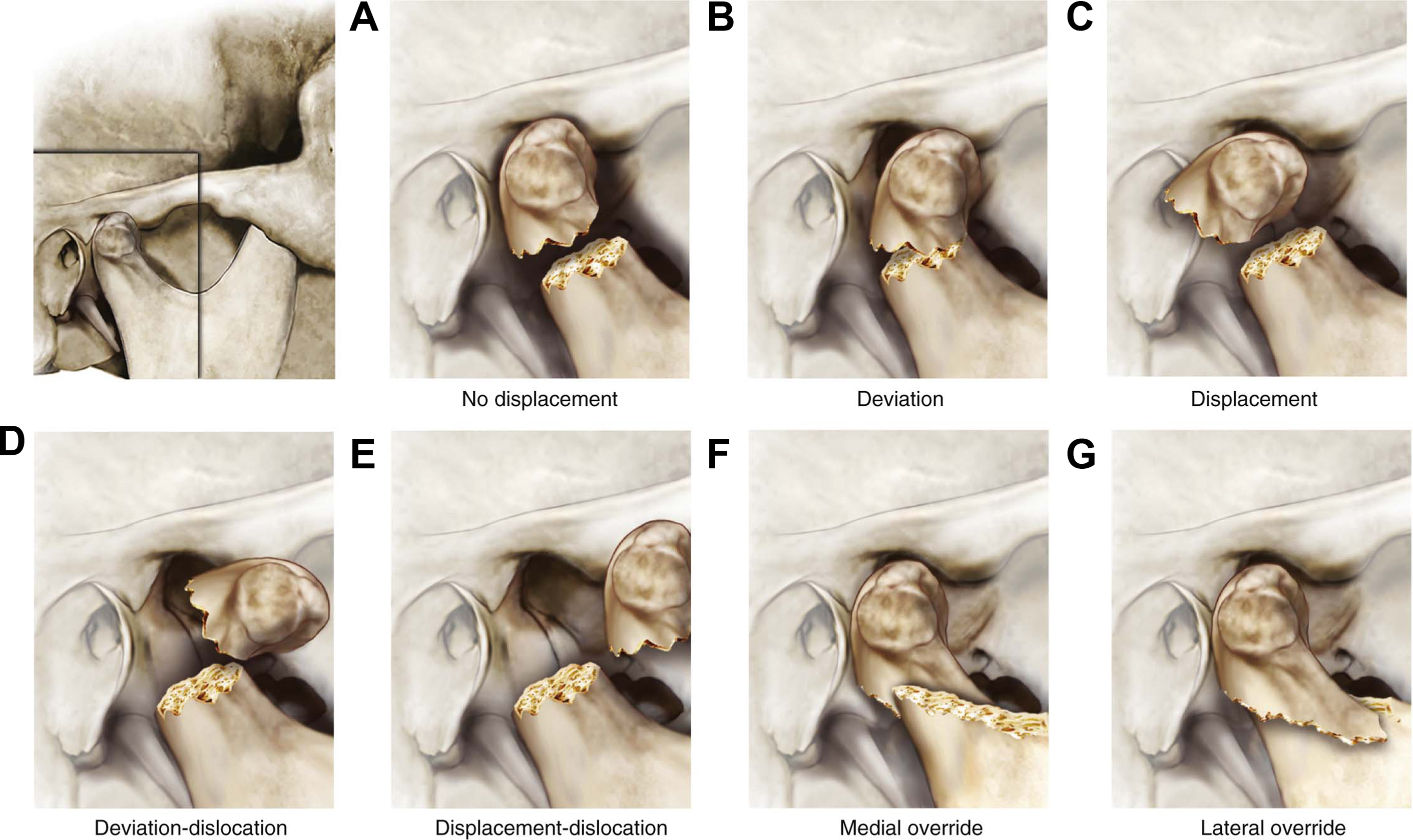
The terminology used in these systems warrants review. The terms “displacement” and “dislocation” have different meanings in European medical journals compared to those from Great Britain and North America. , , The definition that will be used in this article for fracture “displacement” is the relationship of the caudal end of the condyle relative to the mandibular ramus. There may be no displacement, minimal tilting, or medial or lateral displacement resulting in overlap of the segments. , Displacement can be quantified as the degrees of angulation of the bones at the fracture site and millimeters of overlap between the condylar segment and the ramus. , The term “dislocation” refers to the location of the condylar head relative to the glenoid fossa. The term “intracapsular” has been used in reports to refer to fractures of the condylar head which is surrounded by the TMJ capsule but recently the term “diacapitular” was proposed to describe this fracture that may extend beyond the capsule. , ,
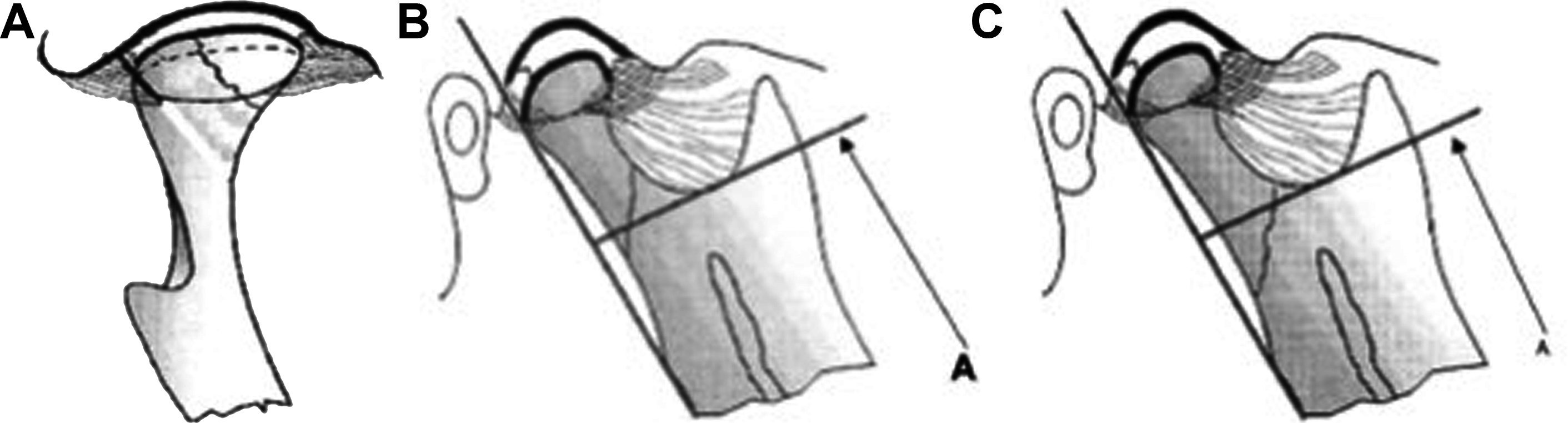
Lindahl’s ( 1977 ) system of condylar fractures includes 3 domains: fracture level, displacement, and condylar dislocation , , ( Fig. 3 ). Loukota and colleagues ( 2005 ) introduced a system that was adopted by the Strasbourg Osteosynthesis Research Group (SORG) that distinguished condylar subsites defining the demarcation between the condylar neck and the subcondylar region using “Line A” a horizontal line drawn tangent to the deepest part of the sigmoid notch and perpendicular to a vertical line parallel to the posterior border of the mandibular ramus ( Fig. 4 ). Condylar neck fractures result from a fracture line wherein more than 50% of the length is above line A, whereas subcondylar fractures are generated by fracture lines 50% or more of whose length is below line A (see Fig. 4 ).
In 2014, the AOCMF published a classification system that includes reproducible landmarks that demarcate fracture levels similar to Loukota’s system (see Fig. 1 ). Angulation/displacement and dislocation of the condylar segment is similar conceptually to Lindahl’s system. This system allows for coding of the specific fractures and we refer the reader to this article for a review of all the domains.
The need for consensus on the use of classification systems was the focus of a study by McLeod et al who reviewed 88 articles published between 2016 and 2019 and identified which condylar fracture classification systems were used. Forty papers used a previously published classification system ( the top three cited were Loukota 2005 = 12; Lindahl 1977 = 10; Neff 2014 = 9 ). , , Thirty-one published studies did not use a fracture classification system and 17 studies included a system not previously published. McLeod concluded with a call for consistency in terminology and classification of condylar fractures and for peer reviewers and journal editors considering studies for publication to encourage more rigor in this area.
Clinical presentation
The initial assessment of all craniofacial trauma begins with the primary trauma survey and emergency management of any potentially life-threatening injuries. Mandibular fractures can result in airway compromise secondary to floor of mouth swelling, hematoma or secondary to posterior displacement of the tongue. Displaced fractures of the mandibular condyle may result in a limited mouth opening, making specialized airway management devices such as the video laryngoscope or flexible fiber-optic bronchoscope necessary for endotracheal intubation. Identification of cervical spine injuries during the initial trauma survey is critical, and the incidence of concomitant cervical spine injuries in patients with mandibular fractures has been reported at 1% to 7%.
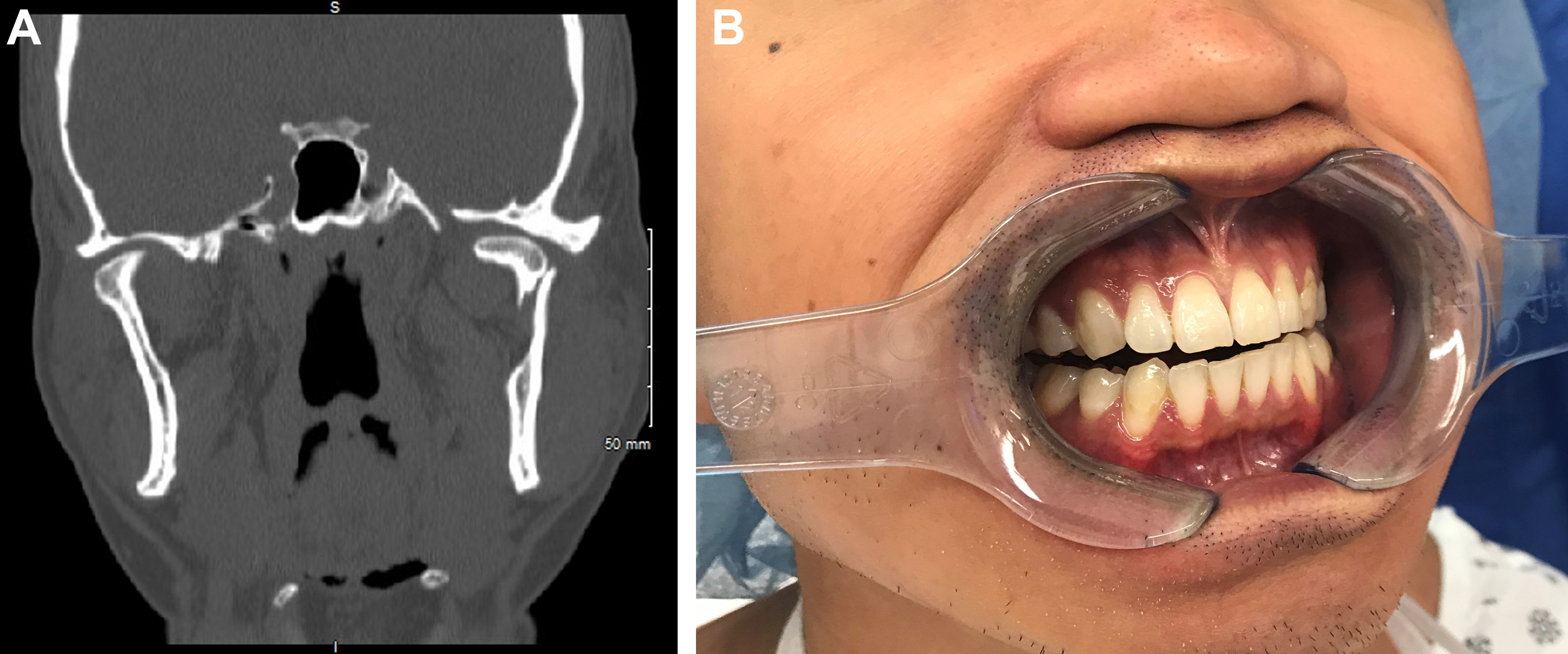
On examination, patients with condylar fractures may have tenderness and edema of the preauricular area; chin lacerations, ecchymosis, or edema; malocclusion, trismus, and deviation of the chin with opening. , Displaced unilateral condylar fractures can result in a loss of vertical ramus height, premature contact of the molar teeth on the injured side, and a posterior open bite on the contralateral side ( Fig. 5 ). The chin can deviate toward the side of injury during opening due to unopposed contralateral lateral pterygoid muscle contraction. Patients with bilateral condylar fractures have bilateral ramus height shortening and premature molar contact resulting in an anterior open bite malocclusion. Trismus, defined as a maximal incisal opening less than 40 mm, may be present due to functional interferences of the fracture segments, joint hemarthrosis, or pain. , Care must be taken in evaluating pediatric patients with a low threshold for imaging with CT scan—especially children presenting after a fall on the chin—to avoid missing a fracture.
Imaging
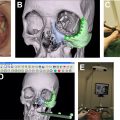
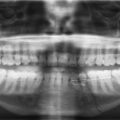
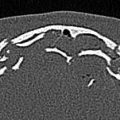
Helical computed tomography is the gold standard for radiographic diagnosis and can be reconstructed into 3-dimensional images. The mandible series is a set of plain x-rays taken from 5 different views ( Fig. 6 ). Towne’s view (patient has their head angled downward 30°), lateral oblique, and lateral views are best for visualizing the condyle. Panoramic orthopantomogram may also be obtained and provides a single composite panoramic image.

Goals of treatment/treatment decision making
Unlike other areas of the mandible, restoration of the condylar segment to its preinjury position is not required for the function to be restored. The following are the 5 outcomes that should be measured to assess attainment of treatment goals: (1) pain-free mouth opening, with an interincisal opening of 40 mm or more; (2) full movement of the jaw in all excursions with no deviation on opening; (3) restoration of preinjury occlusion; (4) avoidance of TMJ dysfunction; and (5) facial and jaw symmetry. There are 3 main treatment options offered to patients. Closed treatment includes 2 possibilities: a conservative therapy regimen of analgesics, soft diet and jaw mobility exercises or maxillomandibular fixation (MMF) to either completely immobilize the mandible or allow limited guided movement controlled by elastics attached to arch bars or MMF screws ( Fig. 7 ). It is important to recognize that closed treatment is not equivalent to closed reduction. , In nondisplaced fractures, the condylar segment may assume a normal or near-normal position. Fracture segments that are displaced or dislocated may reside in a nonanatomical position even after a period of MMF, yet the patient can achieve normal occlusion and jaw movements at the completion of treatment ( Fig. 8 ). One stated advantage of open reduction and internal fixation is alignment and stability of the condylar segment, which is thought to provide the best chance for full functional rehabilitation.

Survey studies that assess practice patterns provide a snapshot of surgeon preferences at a given period and provide an understanding of the evolution of condylar fracture management over time. In 1998, Baker and colleagues surveyed selected expert oral maxillofacial surgeons regarding the management of different presentations of condylar fractures. Among respondents, open reduction, internal fixation (ORIF) of the condylar fracture was most often chosen in the scenarios when the condylar process was dislocated out of the glenoid fossa and malocclusion was present. Twenty-six percent of respondents would perform ORIF with a unilateral condylar fracture-dislocation. For other unilateral fracture scenarios, closed treatment with MMF was overwhelmingly favored when the patient presented with malocclusion (90% when nondisplaced, 78% when displaced).
A more recent survey indicates how treatment approaches have evolved in nearly two decades. Kommers and colleagues (2015) also distributed a survey to OMFS experts who were presented with 3 unilateral fracture cases involving each condylar level. Case 1, a displaced condylar neck fracture with medial override and normal occlusion was treated by 55.6% of respondents with MMF and 19.5% with ORIF if the patient had normal occlusion. If the same patient presented with malocclusion, the recommended treatment selected changed: 49.3% opted for MMF and 46.6% opted for ORIF. For the case of a subcondylar fracture with malocclusion, respondents overwhelmingly (81.3%) chose ORIF. ,
Numerous systematic reviews and randomized controlled trials have been published over the last 25 years comparing outcomes between patients treated closed or open. Initial guidelines for absolute indications included clinical presentations that are rare (middle cranial fossa dislocation of the proximal condylar segment, foreign body within the TMJ for example). The challenge for surgeons is to stratify patients into groups based on imaging and clinical presentation that represent severe, moderate, and mild/stable injuries. Current data have helped to identify the group of patients in whom closed treatment will most likely result in good outcomes: patients with fractures lacking displacement (or minimally displaced) without ramus shortening, lacking dislocation, and/or with normal occlusion. , , Many still recommend closed treatment for condylar head fractures but even that trend is changing. ,
Indications with strong evidence supporting ORIF include the inability to establish normal occlusion during placement of MMF, bilateral condylar fractures, severe condylar displacement (fragment angulation >45°) condylar fracture in edentulous patients, ramus height shortening greater than 2 mm, and associated midfacial fractures. , , , It is the group of patients with more moderate presentations (mild to moderate displacement, minimal overlap but some malocclusion) where surgeons must review the literature, consult expert opinion, assess their own experience, and factor in patient wishes to arrive at a final treatment plan.
The mandibular condyle is a major mandibular growth center with significant potential for remodeling during childhood. The pediatric condylar process that is short with thin cortical bone transforms into the adult form that is longer with a thicker cortex.
The condylar head in children is highly vascular and covered with periosteum with high osteogenic ability leading to an increased risk of TMJ ankylosis as a fracture complication. Conservative treatment and MMF are the most frequently reported management options. The duration of MMF is shorter in younger children than in older children or adults, given concerns about TMJ ankylosis. There is near-universal consensus that in young children (aged less than 7–8 years), open reduction and internal fixation is not indicated, given the risks to mandibular growth and the excellent reported results with closed treatment. , Long-term follow-up of a pediatric patient is required to monitor for the development of malocclusion, growth disturbance of TMJ derangements.
Closed treatment
Descriptions of closed treatment methods, duration of treatment, and specific outcome measures reported vary considerably in the literature. Nondisplaced fractures of the condyle with stable occlusion are well suited for conservative management. Soft diet is typically maintained for 1 to 2 months. These patients undergo close outpatient follow-up to assess occlusion and mandibular function over the course of treatment.
Condylar fractures with mild displacement resulting in malocclusion can be managed with MMF followed by a period of soft diet and rehabilitation. , , The use of arch bars is considered the gold standard of MMF, although Ernst ligatures, and intermaxillary fixation screws are also used. Some protocols recommend a period of rigid MMF and complete jaw immobilization to minimize pain, provide a period of “rest” for the muscles, and allow union between the bone fragments. Duration of MMF varies from 5 to 49 days, with an average of 3 weeks reported in a recent systematic review after which patients may transition to elastics.
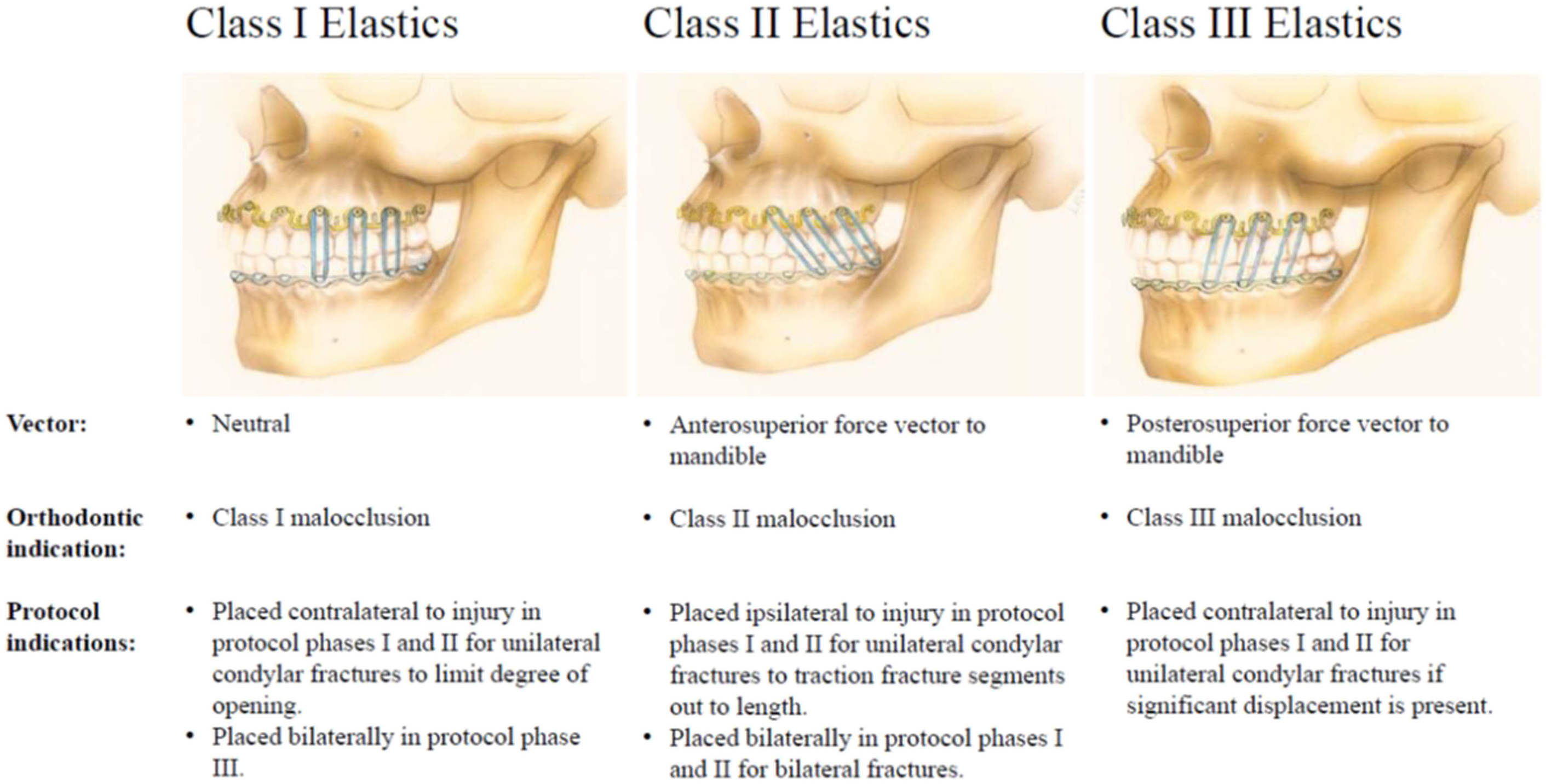
Some protocols recommend immediate placement of elastics, skipping any period of rigid MMF, and using elastics for occlusal guidance ( Fig. 9 ). , , The stated advantage of this approach is early active mobilization which can prevent joint scarring. , , , On the fractured side, elastics are placed in a class II orientation (eg, mandibular first premolar to maxillary canine) exerting an anterosuperior force on the mandible (see Fig. 7 ). , , Class I elastics may be placed on the contralateral side to close the posterior open bite. , Elastics are lightened from heavy to medium to light over 4 to 6 weeks, although they may be worn up to 3 months in some situations (see Fig. 9 ). , ,