Introduction
The management of the contralateral breast following breast conservation therapy (BCT) or oncoplastic surgery is an important yet frequently overlooked component of reconstructive breast surgery. It is now well appreciated that reconstructive breast surgery has improved the quality of life for many women following partial or total removal; however, unless breast symmetry is achieved, patient satisfaction may not be optimized. Although oncoplastic surgery can be successfully performed without a contralateral procedure, it is useful in many women. This is especially true following oncoplastic surgery in which greater amounts of normal breast parenchyma are excised, which will exacerbate any resultant volume or contour asymmetry. Although the exact incidence of these contralateral procedures has not been reported following oncoplastic surgery, it has been reported to range from 15% to 89% following total mastectomy and immediate breast reconstruction.
The purpose of this chapter is to review the techniques, concepts, and principles for contralateral breast operations in the setting of oncoplastic breast surgery. The most common techniques include reduction mammaplasty, mastopexy, and augmentation. Many of these essential concepts have been reviewed in the previous chapters; however, this chapter will focus primarily on the contralateral breast and secondarily on the ipsilateral breast because the two are co-dependent.
Indications and contraindications
Contralateral breast procedures will improve breast symmetry in many women following oncoplastic surgery. There are essentially three different contralateral operations that can be performed: a reduction mammaplasty, mastopexy, and augmentation ( Box 13.1 ). In the case of volume discrepancy, a reduction mammaplasty may be indicated; in the case of contour discrepancy, a mastopexy may be indicated; and in the reverse case in which the contralateral breast is smaller, an augmentation using a prosthetic device may be indicated. The factors guiding these decisions include patient and breast characteristics, timing of surgery, cancer stage, margin status, and postoperative radiation treatments. The contraindications for contralateral breast operations will be related to patient desire, oncologic risks of developing a contralateral breast cancer, and breast characteristics. These factors will be further reviewed.
Preoperative history and considerations
A number of factors should be considered when counseling patients regarding surgery of the contralateral breast. First, the surgeon should confirm that the patient has been thoroughly evaluated for the presence of cancer in that breast. Next, the surgeon must determine the patients’ goals regarding size and shape of the breasts, as well as the position and size of the nipple–areolar complex (NAC). Patients with large breasts should be questioned about associated problems such as back and neck pain, grooving from bra straps, and infections. Risk factors for poor outcomes, such as obesity and tobacco use, should be addressed and appropriately managed. Finally, patients should be educated about the increased risk of breast cancer in the contralateral breast and counseled regarding the importance of continued surveillance by both routine physical exam and breast imaging.
Patient selection
Women who may benefit from a contralateral procedure can be considered in two ways: those who need recontouring and those who need volume adjustments. All of these women have one common denominator: they have all undergone a unilateral oncologic operation and decided to preserve the NAC. The importance of a natural appearance and symmetry should not be underestimated. These women may range in age from young (<30 years of age) to elderly (>65 years of age); however, the majority of women are middle aged, have had children, and have breasts that have become increasingly pendulous, voluminous, and/or ptotic. In some of these women, resection of the primary breast cancer may not result in a perceptible change in contour or volume and obviate the need for a contralateral procedure. However, in other women, a lumpectomy or partial mastectomy can result in a perceptible change and asymmetry between the two breasts. For these women, contralateral operations may be useful.
All women considering oncoplastic surgery are required to undergo imaging studies of both breasts via mammography or magnetic resonance imaging (MRI). The presence of an abnormality in the contralateral breast would be a contraindication for a purely aesthetic operation and would necessitate oncologic evaluation. Women are informed that the cancerous breast following oncoplastic management will be irradiated and should be informed that the breast contour may be altered following the radiation treatments. This fact may influence the decision regarding whether or not to have the contralateral procedure performed immediately or on a delayed basis.
Timing of surgery
The decision to have an immediate or delayed contralateral procedure is dependent upon a variety of factors, which include patient desire, the ability to completely resect the primary tumor, recognition of postoperative and post-radiation changes, and the feasibility of coordinating an operation between the oncologic and reconstructive surgeon. The long-term outcomes are essentially the same, other than the fact that the patient will be asymmetric in the short run. Many women prefer to undergo one procedure, the principal reason being that both breasts can be operated upon at the same time. Prominent volume or contour asymmetries can be a source of dissatisfaction for some women.
An important consideration that influences the timing of the contralateral operation is the ability to completely resect the primary tumor. If the tumor is small and localized and the oncologic surgeon is confident that the tumor has been excised with an acceptable margin of resection, then the acquired deformity can be reconstructed and a contralateral procedure for symmetry performed at the same time. If there are any concerns based on the fact that the tumor is larger than expected, is multifocal, or that an adequate margin of resection is uncertain, then reconstruction of the ipsilateral and contralateral breast should be delayed. Some women may decide to observe the outcome of the initial operation and then decide whether or not to have a contralateral procedure. The advantage of this approach is that margin status can be pathologically confirmed and specific asymmetries noted.
The final consideration is the ability to coordinate schedules between the oncologic and reconstructive surgeons. Obviously, with a delayed contralateral procedure, this will not be a factor; however, in immediate cases, it may. In women with moderate to severe mammary hypertrophy or breast ptosis, a reduction mammaplasty or mastopexy may be needed. Many surgeons support addressing the opposite breast at the time of the cancer surgery because the contralateral breast serves as a model by which the reconstructed breast is patterned. Immediate reduction of the contralateral breast also allows for histological examination of the resected tissues with the potential to find and treat occult disease. On the other hand, some surgeons will endorse a delayed approach, allowing ample time for postsurgical and radiation changes to evolve. Although a secondary procedure may become necessary, proponents will argue that the results are more predictable.
It is an accepted belief that the oncologic portions of the operation are performed by a surgeon specializing in ablative procedures and that the reconstructive portions are performed by a reconstructive specialist. In some settings, the ablative surgeons are comfortable with the reconstructive portions of the operation as well. In these cases coordinating schedules will not be a factor. However, in other situations where the reconstructive portion of the ipsilateral and contralateral breast will be more complicated, a surgeon specializing in breast reconstruction should be involved.
Oncologic considerations
As part of the breast cancer management team, it is important for plastic surgeons to be familiar with the cancer risks women face following treatment of breast cancer. A personal history of breast cancer is the number one risk of developing breast cancer in the contralateral breast. It has been reported that women who have had cancer have a 2–5 times higher risk of getting a cancer in the contralateral breast compared to other women. Other studies have suggested that the risk of developing a new cancer is about 0.5–1% per year. Up to 5–10% of patients with a primary breast cancer will get a contralateral breast cancer sometime in their lifetime.
After breast cancer treatment, women are advised to continue with breast cancer surveillance via physical examination and breast imaging. Women who have had surgery on the contralateral breast for symmetry are advised to obtain a new baseline mammogram 6 months following the operation. Mammographic and clinical findings should be considered more suspicious than in patients without breast cancer. Reduction mammaplasty will alter the parenchymal architecture of the breast and result in microcalcifications. However, these findings are no different from changes associated with other breast procedures such as biopsies and lumpectomies. These changes are easily distinguished from suspicious lesions by experienced breast imagers. It has been demonstrated that reduction of the breasts does not interfere with cancer surveillance.
The surgeon should be prepared to answer questions patients have about the risk of operating on the contralateral breast with regard to a new cancer and the detection of breast cancer. Certain symmetry procedures have been reported to facilitate a woman’s ability to detect cancer and may be beneficial as a risk reduction maneuver. It has been reported that breast reduction can result in a 28% decrease in the risk of breast cancer. Furthermore, reducing the contralateral breast allows for evaluation of the pathologic status of the breast. In one series occult tumors were identified in 4.5% of contralateral breast reduction specimens in patients undergoing a symmetry procedure for breast reconstruction.
There is a smaller subset of patients that are candidates for breast augmentation following BCT or oncoplastic surgery. In general, these are women with relative micromastia who would have considered breast augmentation in the absence of a diagnosis of breast cancer. Patients who consider or have augmentation with prosthetic devices should be counseled about the need for specialized breast screening. When using the standard craniocaudal and medial–lateral–oblique views of screening mammography for women with implants, up to 40% of the breast parenchyma is potentially obscured. For this reason, specialized implant displacement views have been developed. With these views, an implant in the subglandular position obscures 35% of the breast, and the submuscular position obscures 15%. Thus, women should be made aware that the presence of an implant may hinder breast cancer detection.
Operative technique
Surgical anatomy
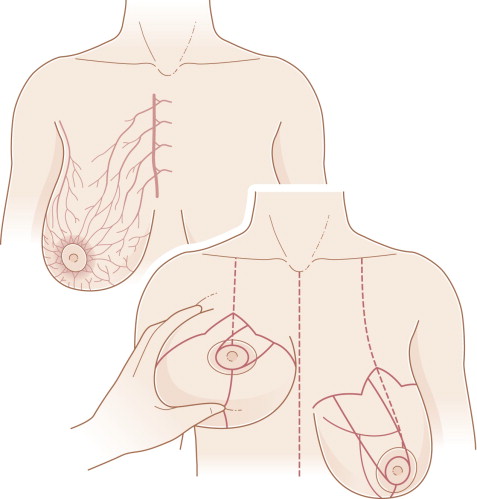
The blood supply to the breast comes from perforating branches of the internal mammary, lateral thoracic, thoracodorsal, thoracoacromial, and intercostal arteries and veins ( Fig. 13.1 ). The sensory innervation of the breast is dermatomal and derived from the anterolateral and anteromedial branches of the thoracic intercostal nerves T2–T6. Sensation to the NAC is principally derived from the fourth thoracic intercostal nerve. When designing and executing any aesthetic operation on the breast, the vascularity and innervation must be considered. Poorly designed operations can result in nipple–areolar necrosis, loss of nipple areolar sensation, delayed healing, fat necrosis, and persistent asymmetry. There are several methods by which a given breast can be reduced in volume or altered in shape.
The ensuing sections will review the authors’ preferred methods of reduction mammaplasty, mastopexy, and augmentation. The operative techniques that will be reviewed can be performed immediately (at the time of oncoplastic resection) or on a delayed basis. In general, reduction mammaplasty procedures are performed immediately or on a delayed basis, whereas mastopexy and augmentation are always performed on a delayed basis. The specific reduction technique can be a vertical or short scar approach or the traditional ‘inverted T’ using the Wise pattern. The specific approach is dependent upon the plastic surgeon’s preference and level of comfort. In general, the short scar techniques are used for resections less than 300 g and the Wise pattern is used for resections greater than 300 g. Mastopexy is performed with various patterns that include a circumareolar approach, a circumvertical approach, and an inverted T or Wise pattern approach. Breast augmentation is rarely used but may be considered in select cases. The various techniques will be briefly described.
Immediate contralateral reduction mammaplasty using a Wise pattern
Preoperative markings
In patients who will have immediate bilateral reduction mammaplasty following unilateral oncoplastic surgery, several considerations are important. The first is that the specific reduction technique may be different for the two breasts. This is because the specific location of the resected tumor may alter the orientation of the pedicle. The reconstructive surgeon should have a general idea or concept of how the breast will appear following the procedure. The contralateral breast will serve as a template for the oncoplastic breast. Another consideration is that the cancer breast will be radiated and the contralateral breast will not. This may cause the oncoplastic breast to shrink; therefore, that breast should be reconstructed to be slightly larger than the non-cancerous breast.
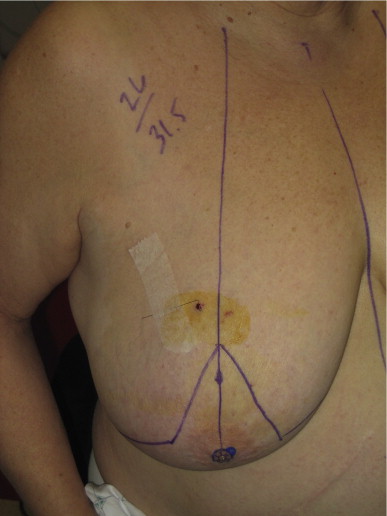
There are several important landmarks that are delineated prior to the reduction. These include the sternal midline, the inframammary fold, and the breast meridian ( Fig. 13.2 ). The breast meridian is determined by marking the mid clavicle and then delineating the midline of the breast. Usually this will bisect the NAC; however, when the NAC is medially or laterally displaced, the meridian will be to the right or left of the NAC ( Fig. 13.3 ). The location of the NAC is usually based at the level of the inframammary fold (IMF) at the point where the breast meridian is bisected. A Wise pattern is delineated on both breasts ( Fig. 13.3 ).


The orientation of the pedicle that will ultimately perfuse the NAC is an important consideration. For upper pole tumors, an inferior pedicle is preferred. For lower pole tumors, a superior, superomedial, or medial pedicle is preferred. For medially or laterally based tumors, the pedicle is oriented such that the resulting deformity can be adequately filled. This is usually achieved using a pedicle that is oriented 180 degrees away from the defect.
Technique
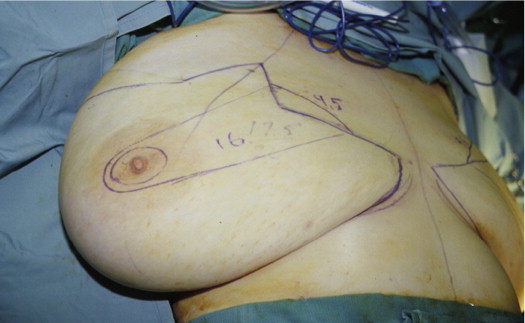
The ablative surgeon is advised to proceed with the resection of the tumor. If the tumor is within the delineated Wise pattern then the incision can be placed either on or within the pattern ( Fig. 13.4 ). If the tumor is outside the Wise pattern, the incisions may have to be extended in order to facilitate the excision ( Fig. 13.5 ). This may alter the appearance of the incisions when comparing the two breasts; however, it is acceptable following maturation of the scars. Following excision of the tumor and surrounding parenchyma, the specimen is weighed and the volume is assessed.

Attention is directed toward the contralateral breast. In general, a medial pedicle is preferred, especially when the anticipated resection volume will exceed 600 g and the NAC requires >6 cm of elevation. A superomedial pedicle is usually preferred when the NAC is elevated more than 6 cm. This is because the longer pedicles will rotate on an arc more easily than the shorter pedicles. Short pedicles often require a back-cut along the dermis of the proximal pedicle to facilitate rotation without kinking. An inferior pedicle is used when the length of the nipple to IMF is less than the length of the delineated medial pedicle or when the majority of breast volume is superiorly located.
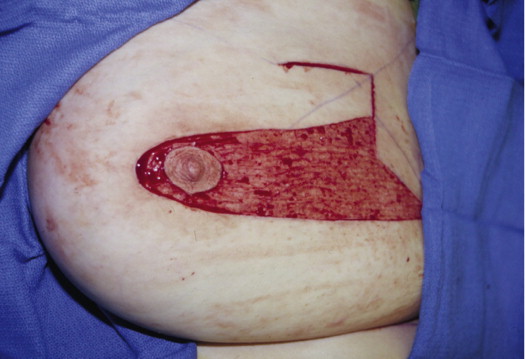
The first step is to inscribe the NAC with a 38–45 mm cookie cutter ( Fig. 13.6 ). The perimeter of the inscription is incised and the pedicle is de-epithelialized ( Fig. 13.7 ). The Wise pattern markings are then incised. Dermoglandular wedge excisions are then performed. For a medial or superomedial pedicle, the dermoglandular excision is primarily inferior and lateral ( Fig. 13.8 ). For an inferior pedicle, the dermoglandular excision is predominantly superior and lateral. The handling of the vascularized pedicle is important. In general, the pectoral attachments of the pedicle are preserved in order to optimize blood supply. The vascularity of the pedicle and NAC is derived from the subdermal plexus and the intercostal/pectoral perforating vessels ( Fig. 13.9 ). Perfusion to the NAC is assessed by adequate arterial bleeding from the dermal edges. Following the dermoglandular excision, the pedicle is rotated toward the apex of the vertical limbs of the Wise pattern ( Fig. 13.10 ) and the reduction pattern is closed ( Fig. 13.11 ).



Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Oncoplastic Breast Surgery and the Effects of Radiation Therapy
Oncoplastic Breast Surgery and the Effects of Radiation Therapy
 Breast Augmentation Technique (Biplanar) for Oncoplasty
Breast Augmentation Technique (Biplanar) for Oncoplasty
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


