The main goals of a lower eyelid blepharoplasty for lower eyelid rejuvenation are orbital contouring of the fat pad compartments, achieving a smooth transition at the lower eyelid-cheek junction, and reducing the amount of skin laxity while maintaining proper eyelid function. Unless severe festooning and dermatochalasis are present (see Chapter 10 ), there is minimal, if any, skin removal performed. In order to reach the orbital fat compartments, two distinct techniques may be used. The incision may be placed either at the cutaneous border of the lash line (transcutaneous or subciliary approach) or on the conjunctival side (transconjunctival approach), which can be either preseptal or postseptal ( Fig. 5.1 ). If the transcutaneous approach is chosen, Dr. Levit and Dr. Rabinovich prefer to extend the subciliary incision past the lateral commissure which allows easier lateral undermining of the skin or skin/muscle flaps with better visualization of the anatomy. This technique partially hides the scars under the lashes as well as tightens redundant skin and resuspends the orbicularis oculi muscle using periosteal sutures. At the end of this chapter, we will also discuss a different approach commonly practiced by author EL.
Until the early 2000s, transcutaneous blepharoplasty using a subciliary incision was considered the optimal approach. This approach, however, is associated with complications related to lid malpositioning, excessive removal of fat causing a hollowed appearance, scarring, and loss of eyelashes at the tarsal plate. , Originally described by Bourguef in 1924, the transconjunctival route with conservative fat pad removal is preferred by most surgeons. Some authors also prefer to reposition the fat pads over the orbital rim rather than excise the fat pads. , This is especially true when less skin laxity is present. This approach has increased in popularity as it reduces complications associated with lid malpositioning and scarring, due to the absence of skin incisions.However, this approach comes with other risks, including possible injury to the inferior oblique muscle. Furthermore, the inability to excise skin along with fat removal can sometimes worsen skin redundancy and lower eyelid rhytids. This skin redundancy can be improved by performing simultaneous laser resurfacing.
A combination approach with fractional ablative laser skin resurfacing can lead to a reduction in superficial fine lines and wrinkles in addition to modest correction of lid laxity. The most common challenge associated with this combination approach is the addition of postoperative erythema. It is important to inform patients that this is not an adverse effect and truly is an expected outcome. Depending on the skin type, energy, and depth of the laser resurfacing, a patient with an appropriately resurfaced lower eyelid is expected to be extremely red for 10 to 14 days and pink for an additional 2 to 3 months after the procedure. Although redness may be improved with a pulsed-dye laser, this poses an additional risk of damage to the pigmented epithelium of the retina. Author HK advises patients to use makeup 14 days after the procedure. Male patients who do not typically wear makeup are advised to wear a tinted sunscreen to camouflage the redness. HK also has found that 4 weeks of pre-treatment and 6 weeks of post-treatment with Alastin® regenerating skin nectar (Alastin® Skincare Carlsbad CA) can help reduce the redness further.
In contrast to the upper eyelid, which only has medial and central fat pads, the lower eyelid has three fat pads: medial, central, and lateral. Whereas fat removal is optional in upper eyelid blepharoplasty, fat removal or repositioning is essential in the lower eyelid counterpart. The inferior oblique muscle is the structure of utmost importance to recognize and identify in lower eyelid blepharoplasties. This muscle is positioned between the medial and central fat pads. Injury to this muscle can lead to the inability to look upwards and inwards, causing diplopia ( Fig. 5.2 ).

Operative goals of lower eyelid blepharoplasty
- 1.
Resection or repositioning of the retroseptal fat pads and release of the retaining ligaments.
- 2.
Maintaining a smooth transition between eyelid and cheek junction, either by micro fat grafting or repositioning of the fat pads.
- 3.
Removal of redundant skin and/or hypertrophic orbicularis oculi muscle if needed. Resurfacing the redundant skin as an alternative to skin excision.
- 4.
Maintaining full function of the lower eyelid and prevention of lower eyelid malpositioning and scar tissue.
Preoperative skin marking
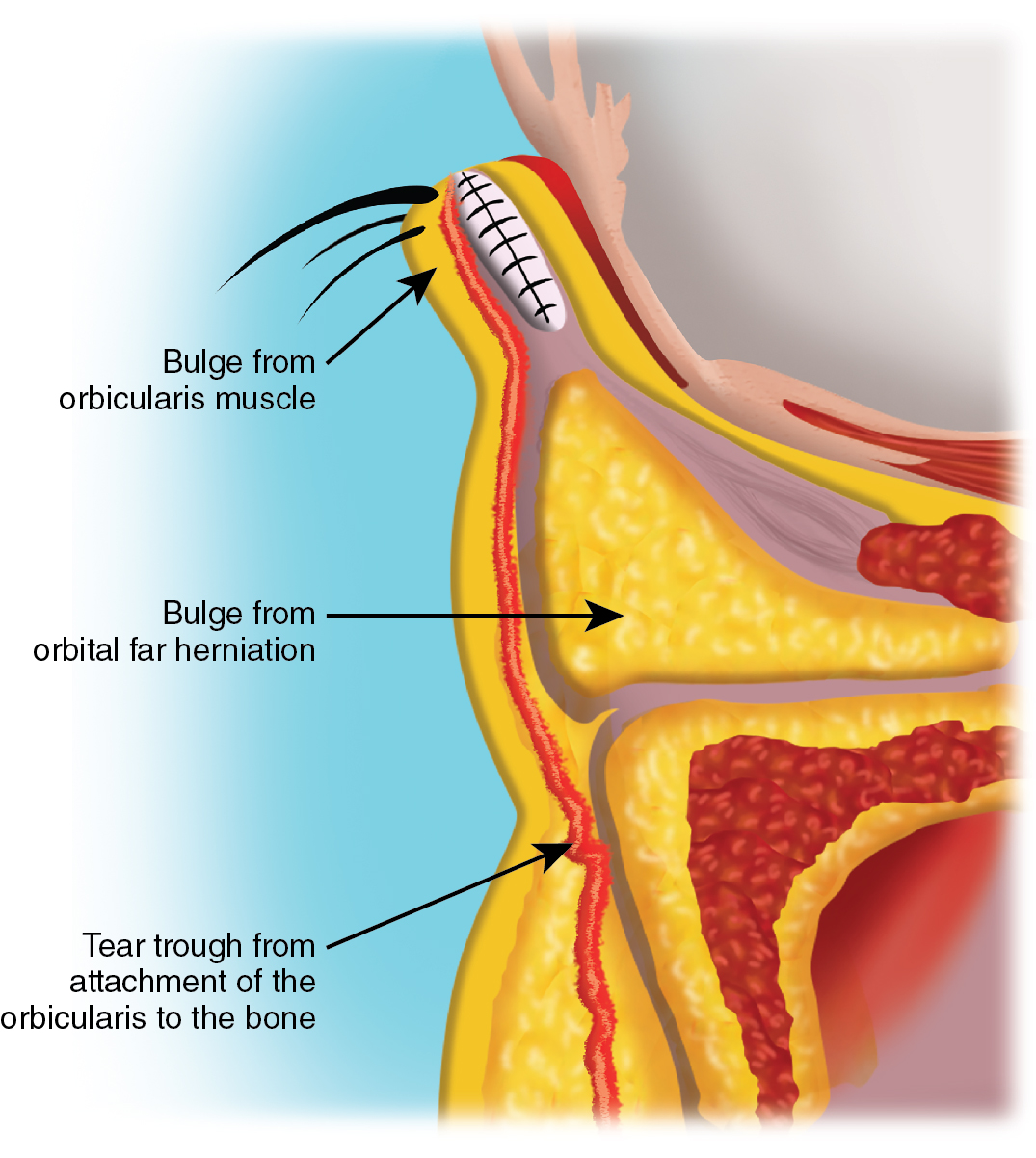
Skin marking of the prolapsed fat pads should be performed with the patient sitting in an upright position with an upward gaze ( Fig. 5.3 ). Lower lid snap-back test should be performed to estimate the amount of lower lid laxity present (please refer to Chapter 2 for more details). The presence or absence of lower eyelid rhytids, orbicularis muscle hypertrophy, and festooning should also be noted at this time. If choosing the transconjunctival approach, it is imperative that patients are adequately counseled regarding the inability of this technique to completely correct festoons or pretarsal orbicularis muscle hypertrophy ( Fig. 5.4 ).

Local anesthesia
To begin the anesthetic process, the conjunctiva should be anesthetized with topical anesthetic drops; the authors prefer to use proparacaine 0.5% or tetracaine 0.5%. A local injection of 2% lidocaine with 1:100,000 epinephrine mixed with 0.5% bupivacaine in a 1:1 proportion is injected subcutaneously below the margin along the length of the eyelid. This is done if the skin will also be removed. This mixture is then injected transconjunctivally below the tarsus in a similar fashion. Additional anesthetic agent is injected into the nasal, central, and temporal fat pads transcutaneously. A total anesthetic dose of approximately 3 mL is injected into each eyelid. About 15 minutes should be allowed for the vasoconstrictive properties of epinephrine to take effect prior to the first incision. , For improved patient comfort, IV sedation by an anesthesiologist, in addition to the above local anesthetic measures, can be considered. A sterile aseptic technique should be maintained throughout the surgery.
Surgical tray with instruments
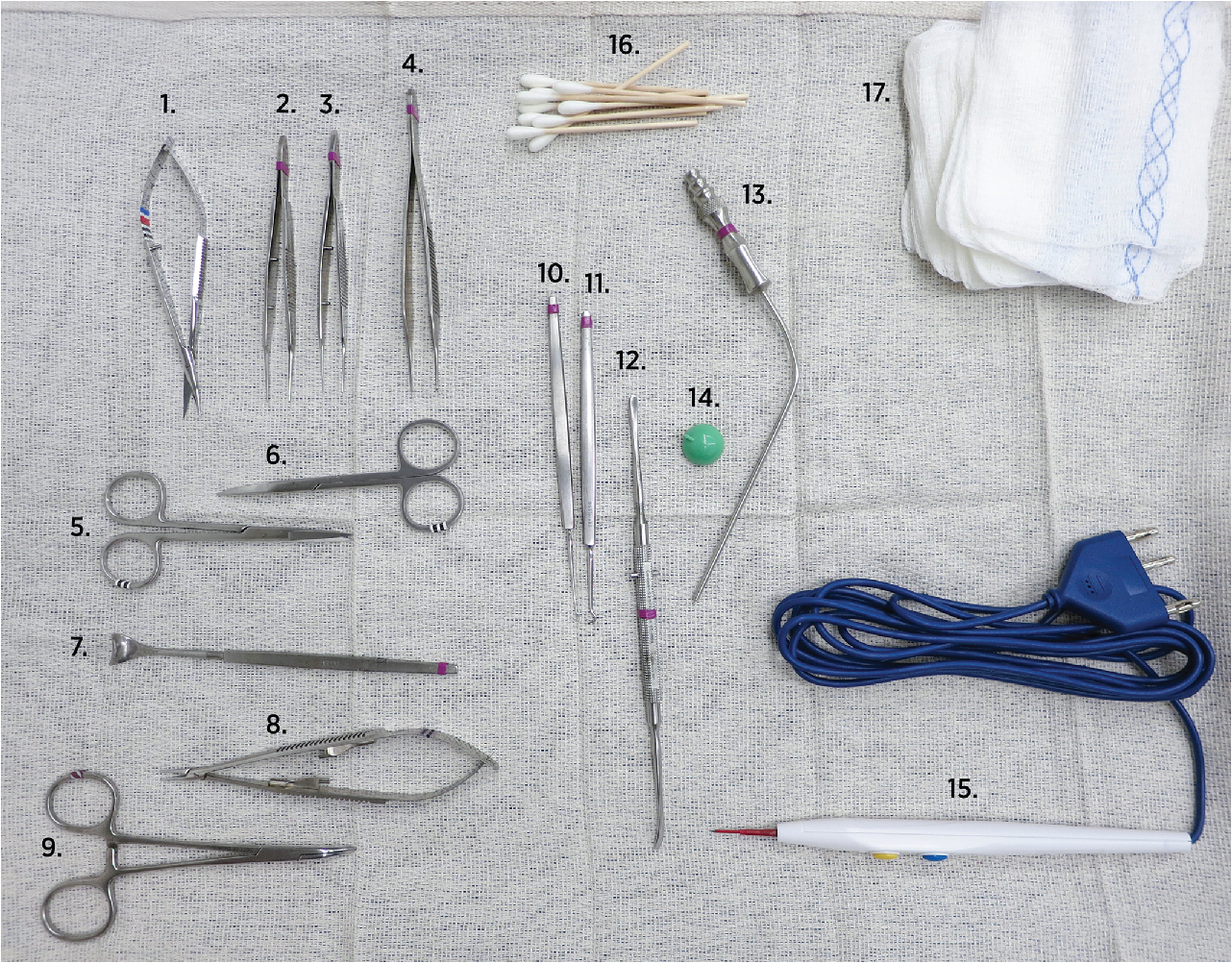
The instruments needed for lower blepharoplasty are laid out on the surgical tray in Fig. 5.5 below.
- 1.
Westcott scissors.
- 2.
Bishop-Harmon forceps with teeth (size 0.12).
- 3.
Bishop-Harmon forceps with teeth (size 0.3).
- 4.
Bishop-Harmon forceps with teeth (size 0.5).
- 5.
Straight Iris scissors.
- 6.
Curved stevens scissors.
- 7.
Desmarres retractor.
- 8.
Castroviejo needle holder.
- 9.
Curved hemostat created.
- 10.
Skin hook sharp.
- 11.
Muscle hook.
- 12.
Freer periosteal elevator 7.5″.
- 13.
Frazier suction tip.
- 14.
Plastic eye shield with eye hook for removal using the eye shield skin hook.
- 15.
Monopolar cautery pen/Bovie with cut coag and blend options. #15 Bard-Parker blade can be used to make skin incisions. Monopolar cautery is used to make transconjunctival incisions. Use appropriate grounding pad as close to the neck as possible.
- 16.
Q tips.
- 17.
4×4″ gauze.
- 18.
Not shown in the image above are the sutures we use; they include:
- a.
5-0 Prolene double armed (for canthopexy) × 2.
- b.
5-0 Vicryl suture (for orbicularis suspension).
- c.
6-0 Prolene/Ethilon (for skin closure).
- d.
5-0 Silk suture (used for retracting the upper and lower eyelids).
- a.
Transconjunctival lower eyelid blepharoplasty (see  )
)
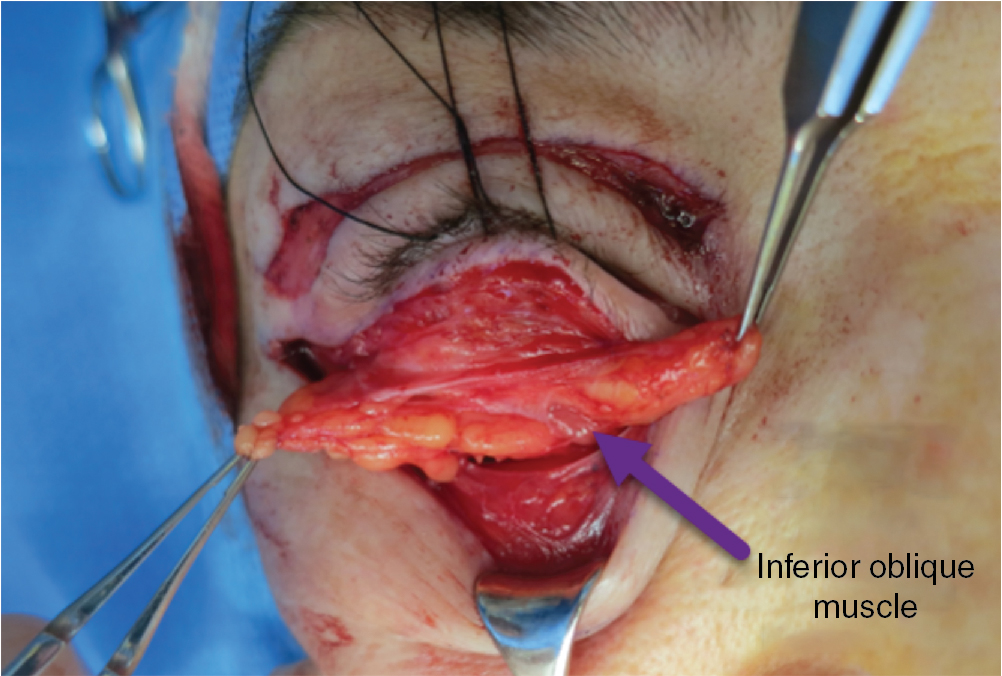
The globe is protected using either stainless steel, plastic eye shields, or more commonly a coated Jaeger plate with an assistant everting the eyelid over Desmarres lid retractor prior to use of the 0.2 mm focused hand piece of the ablative carbon dioxide (CO 2 ) laser in the continuous wave mode at a power of 4 to 8 watts. Alternatively, the Colorado needle attached to a monopolar cautery unit may be used in 14 cut and 10 coag mode; the latter technique is preferred by AR. The conjunctiva and lower eyelid retractors, including the capsulopalpebral fascia, are incised at a level below the vascular arcades approximately 8mm below the tarsal plate (see Fig. 5.1 ). The procedure is performed anterior to the orbital rim, with special care taken to avoid injury to the inferior oblique muscle, located between the medial and central fat pads.
Inferior oblique muscle tracks between the medial and central fat pads. This important muscle is most susceptible to injury during the transconjunctival approach.
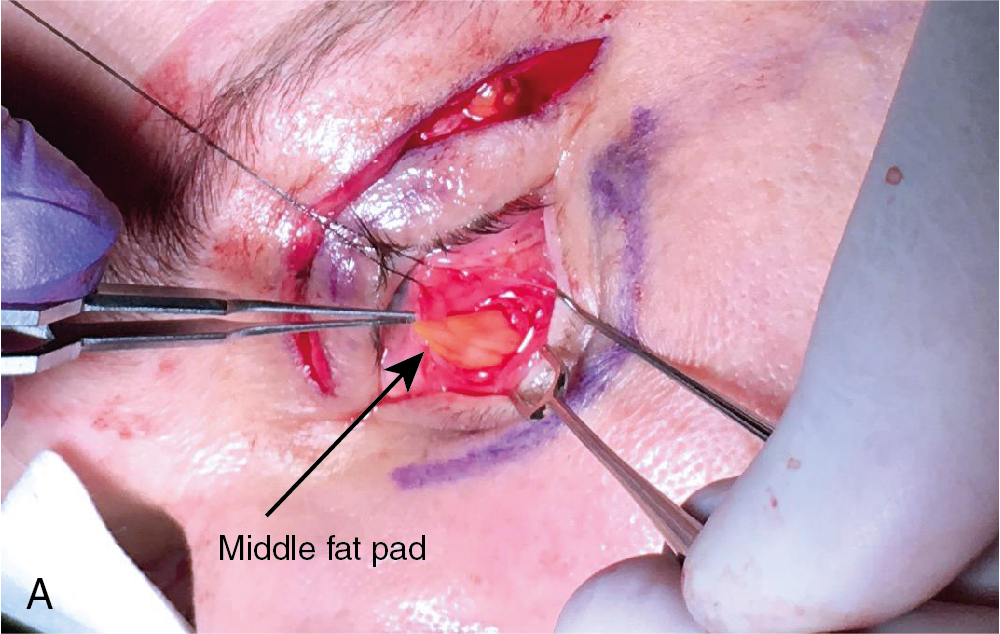
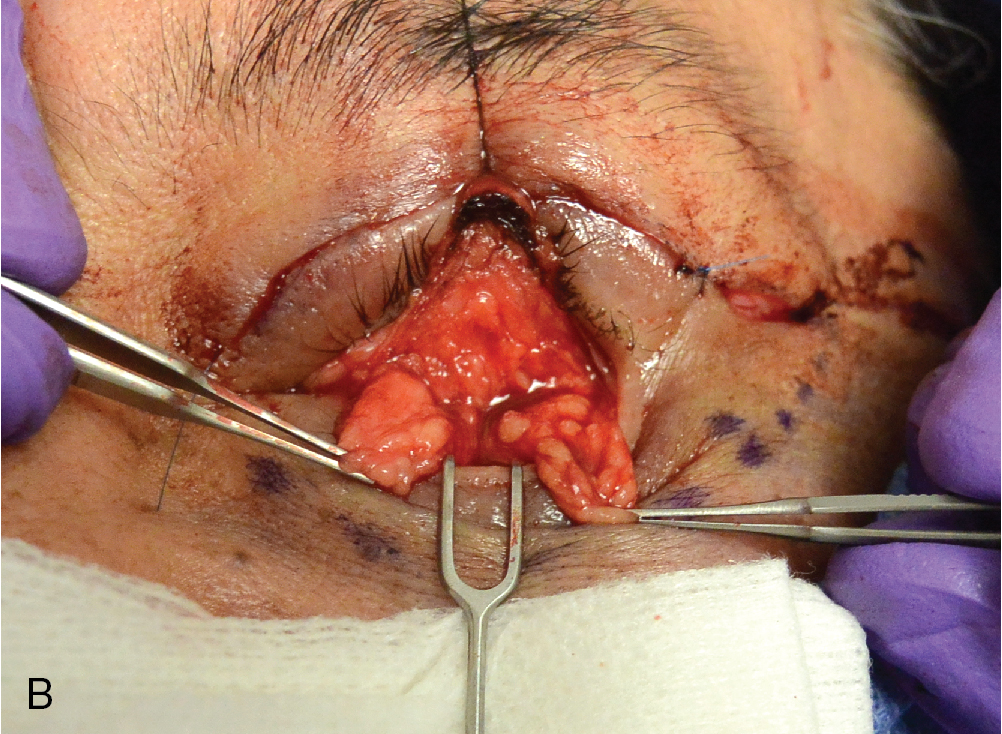
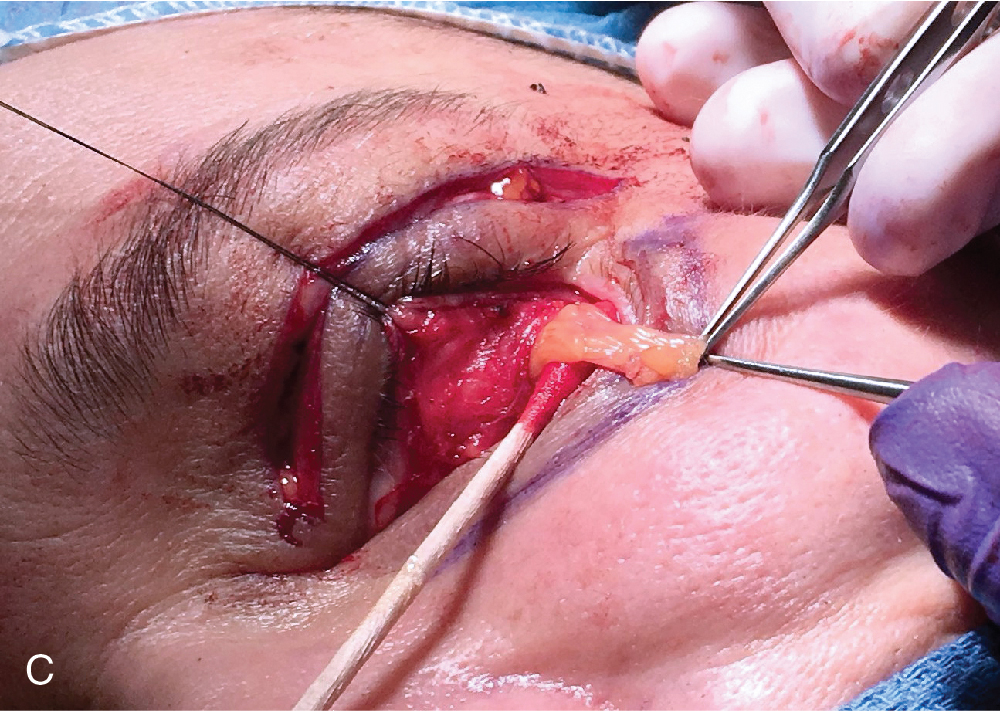
The assistant should retract the lower eyelid utilizing a Desmarres lid retractor into the incision site with one hand while occasionally providing gentle, downward pressure on the eye shield allowing retropulsion of the globe to prolapse the fat. Care must be taken not to overresect the fat pads in order to avoid leaving a hollow appearance. Using cotton tip applicators, each individual fat pad is bluntly dissected out, and the inferior oblique muscle is identified in order to prevent iatrogenic injury ( Figs. 5.6 and 5.7 A–C).
The fat prolapsing to the level of the orbital rim should be removed, with extra care taken to avoid severing larger blood vessels. Inadequate hemostasis can result in prolonged postoperative bruising or possibly even a retrobulbar hematoma. Gentle fat removal may be performed by either clamping the fat, excising it, and then cauterizing the base, or by simply coagulating it with either a monopolar Colorado needle at coag 10 HPF or melting it with CO 2 laser in continuous wave defocused mode. Bleeding can be minimized with the CO 2 laser’s thermo-coagulative properties while dissecting tissue, allowing the surgeon better intraoperative visualization of the retroseptal fat pockets.
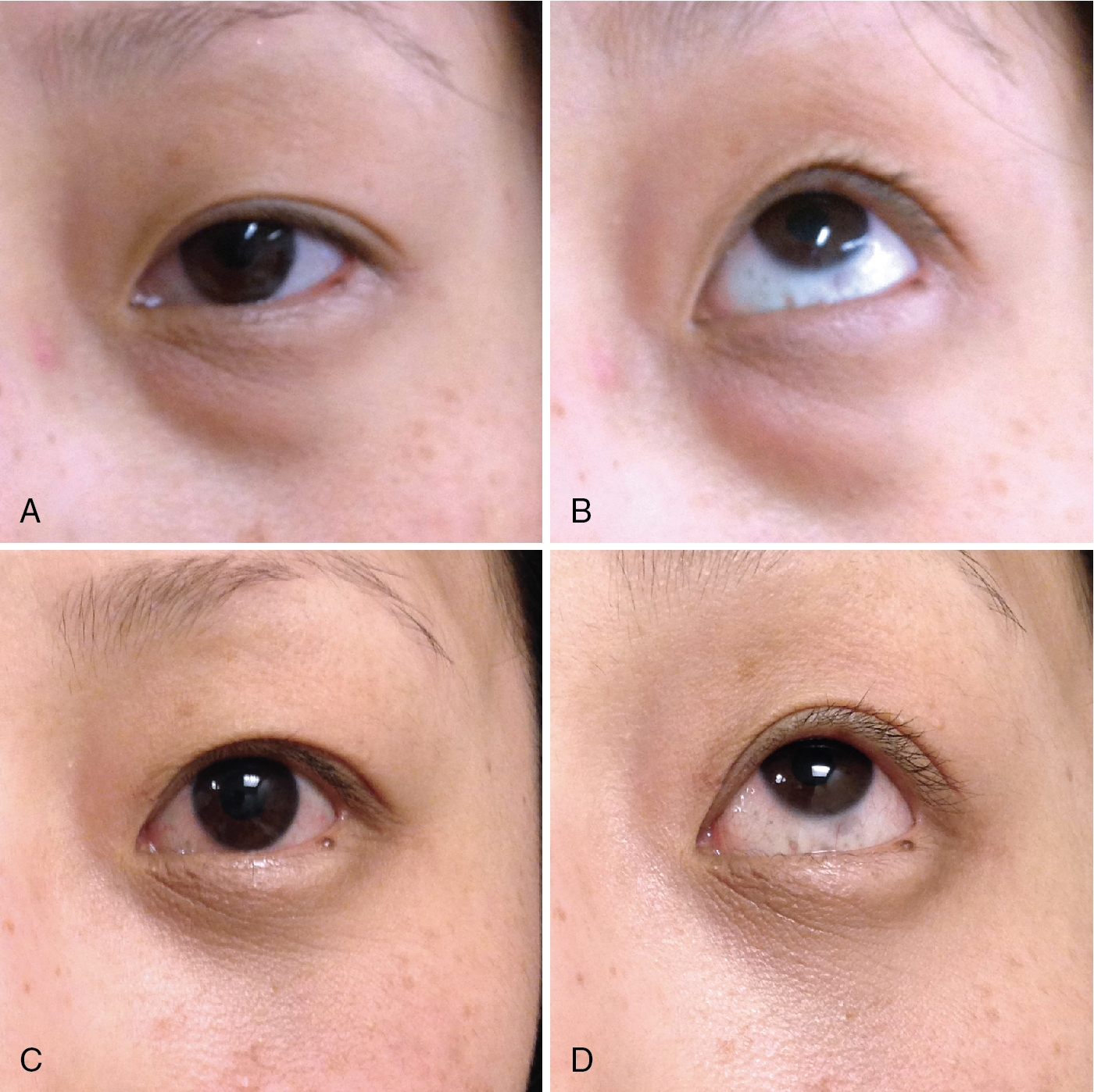
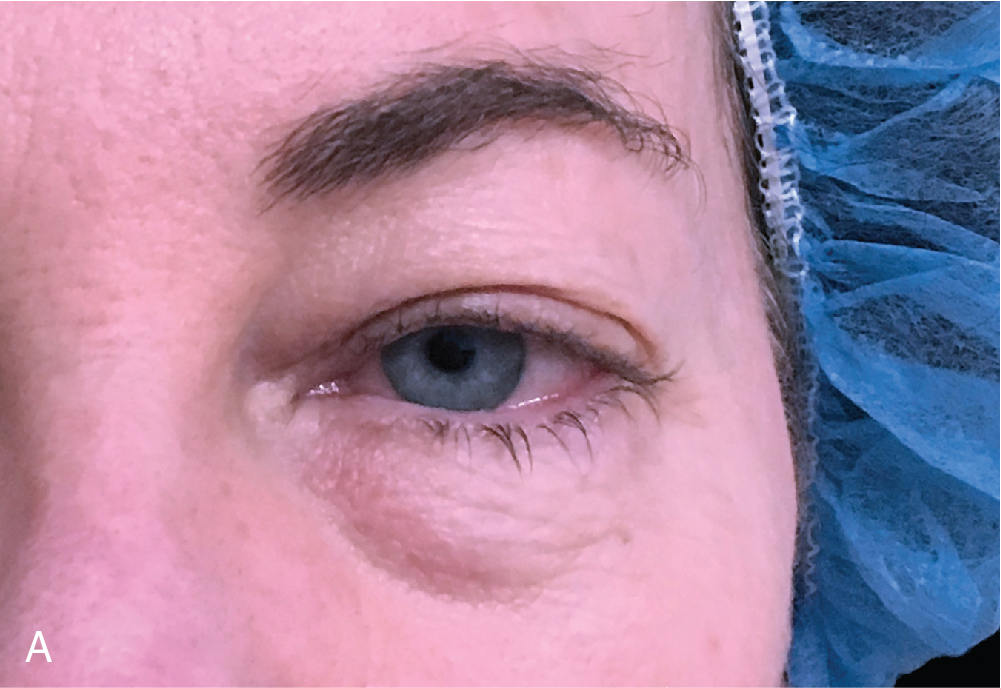
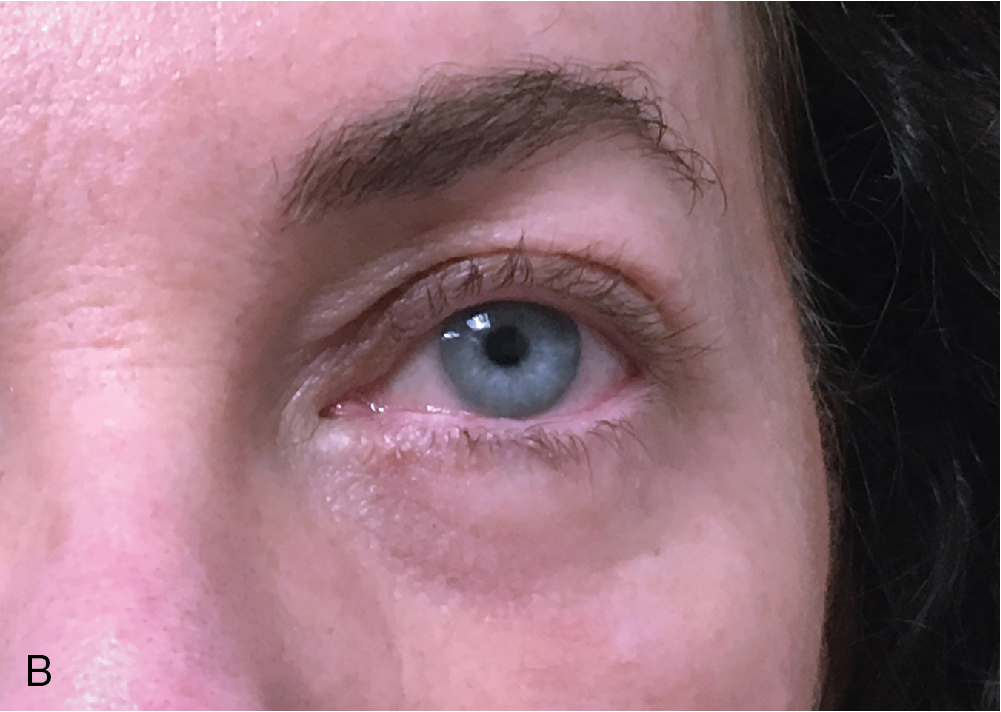
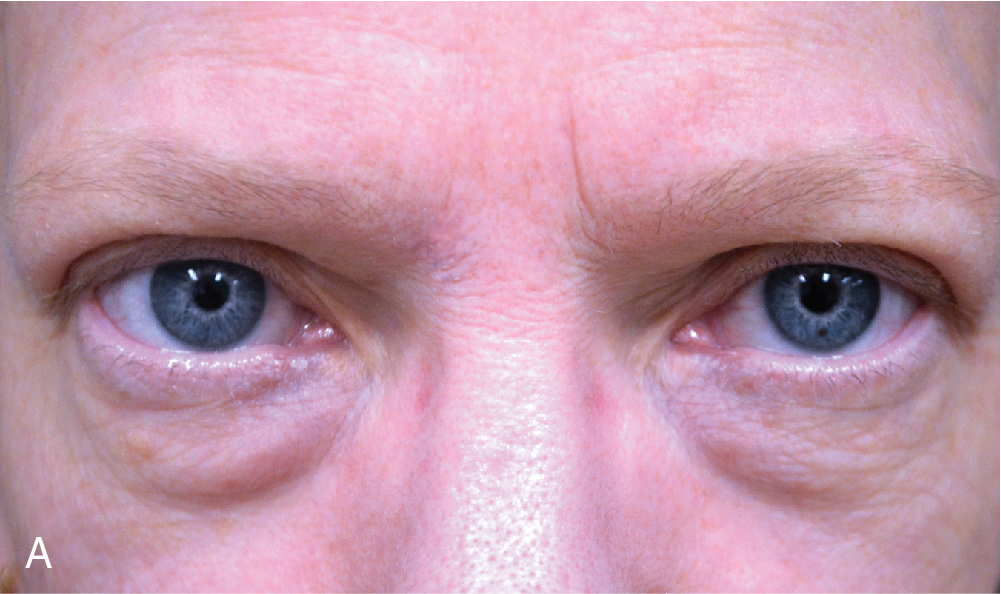
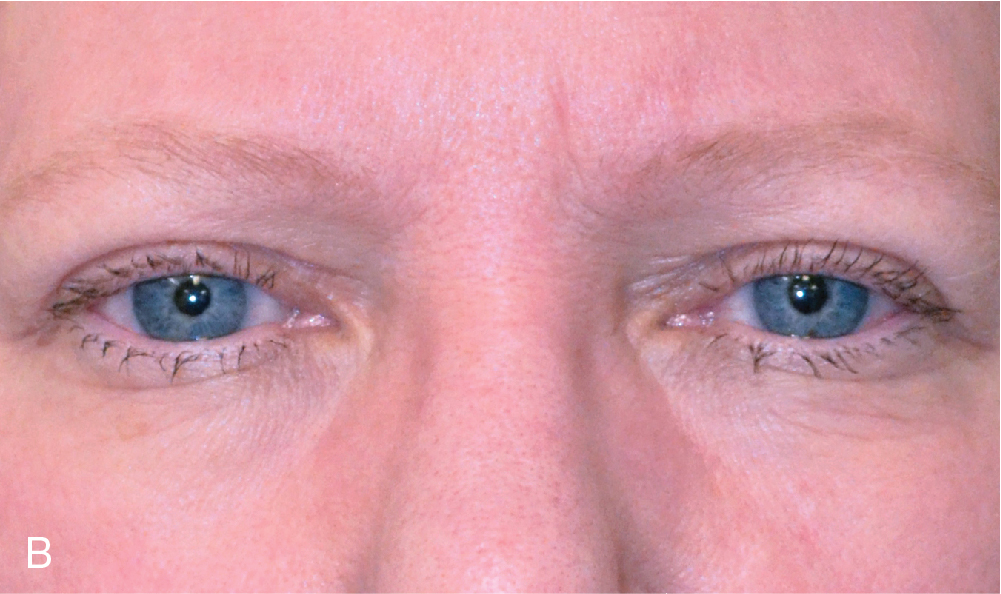
Although some authors opt to suture the trans-conjunctival incision, authors HK and EL do not find this to be necessary as the incision line usually heals beautifully without sutures within 3 to 4 days. Some surgeons, especially oculoplastic specialists, AR included, use two to three buried interrupted 6-0 plain gut fast absorbing sutures to approximate the incision without any complications noted to date. Suturing may lead to conjunctival irritation and subsequent foreign body granuloma formation with delayed wound healing. If fat pad transposition is not performed (more details below), one can alternatively combine this procedure with fat grafting to smoothen the transition from the cheek to eyelid junction. Figs. 5.8–5.10 demonstrate preoperative and postoperative images of trans-conjunctival lower lid blepharoplasty.
Once marking is completed and you begin the procedure, in HK’s and EL’s experience, the majority of the time is spent looking for and removing the lateral fat pad. HK feels it takes approximately 30 minutes to 1 hour to perform a lower eyelid blepharoplasty, and half of that time is spent finding and removing the lateral fat pad. Some suggest that if one cannot find the lateral fat pad, it is possible to transition into a transcutaneous approach laterally in order to find and remove it more easily (see section Lower Blepharoplasty Minimal Incision Technique later). In AR’s experience, if one retracts with a Desmarres retractor laterally at the level of lateral orbital rim, lateral fat pad should be easier to identify.
Additional fat grafting technique to accompany fat removal in lower eyelid blepharoplasty (  )
)
The harvest site (typically the lower abdomen) is infiltrated with 200mL of a 0.1% lidocaine tumescent anesthesia solution. From a 250mL bag of normal saline, remove 16mL, then add 12.5mL of 2% lidocaine, 3.1mL of sodium bicarbonate, and ¼ ampule of epinephrine 1:1000. The fat is harvested utilizing a micro-harvesting cannula with 10mL syringes (HK uses Tulip Gold Standard Small Volume Fat Injection set). The fat is centrifuged at 1500 rpm for 3 minutes. In order to isolate micrograft which can be easily injected via a 19 gauge cannula, the fat must first be filtered. This is achieved by attaching Tulip’s single use 2.4mm fat transfer filter to two 10mL syringes and passing the fat back and forth between the syringes 30 times. The filtered microfat is then transferred to 1mL syringes and a 19-gauge cannula is attached to each syringe. An 18-gauge needle is used to puncture the skin at the superior aspect of the nasolabial fold to allow entry of the cannula. A multi-lamellar fanning approach is used to fill the cheek eyelid junction with an average of 2 to 4mL of fat per side, as needed. It is important to over correct at the time of injection since there is anticipated 50% loss over the following 6 months. Alternatively, in patients who do not wish to be overcorrected due to unnatural fullness for 6 months, one can schedule a second fat transfer session 6 months after the initial injections. Author HK prefers the microfat injection method over the fat repositioning method as the latter seems to produce lumpiness and inconsistent results in some patients. The lumpiness can often be appreciated when the patient smiles, but not at rest. Particular care should be taken with respect to trauma of the infraorbital vessels and nerves in this region.
Fat pad repositioning
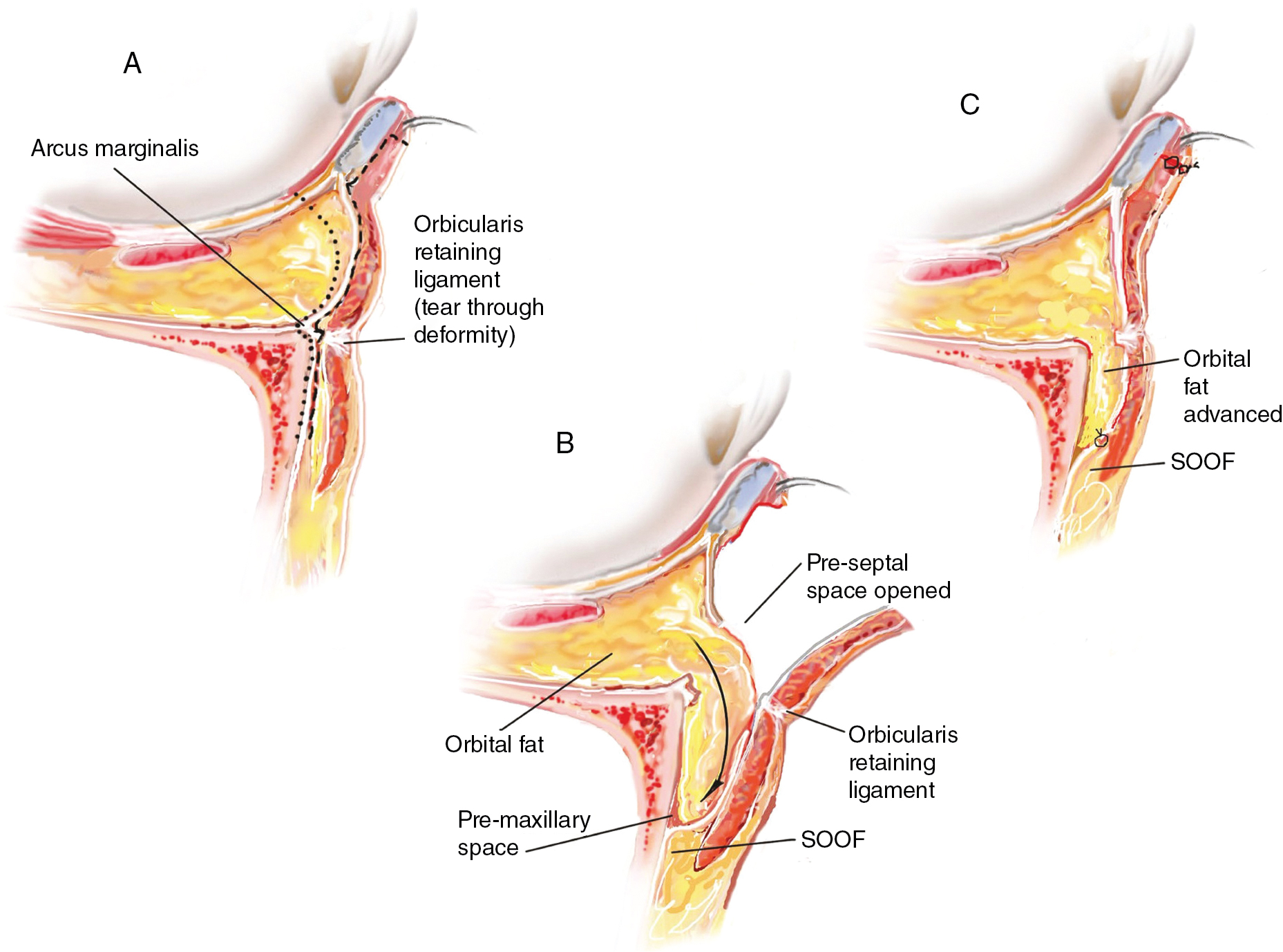
Repositioning of the medial and central fat pads is only possible if their lengths are easily redraped over the most inferior point of the volume depletion along the naso-jugal groove without manual stretching ( Fig. 5.11 A). Typically, a pedicle length of over 1-1.5cm is preferred. Lower eyelid fat pad repositioning can be performed in the sub- or supra-periosteal plane (see  ). After the fat pads have been exposed, blunt dissection of the orbital rim with exposure of the arcus marginalis is performed. The periosteum is incised using monopolar cautery or using a blunt curved scissor. Dissection in the subperiosteal plane is performed with the aid of a Cottle or Freer elevator (see Fig. 5.11 B). Electrocautery with a fine tip can be used at low energy settings to control bleeding vessels that arise from dissecting the periosteum to reach the relatively avascular subperiosteal plane. It is in this plane that the dissection is carried out medially and laterally based on the skin markings placed during preoperative preparation. Care should be taken to avoid trauma to the infraorbital nerve and vessels (typically located 2.7 cm from the midline and 0.9 cm inferior to the orbital rim). Again, care must be taken to avoid trauma to the inferior oblique muscle, which is situated between the medial and central fat pads. Once the pedicles are completely delineated and dissected, a double-armed 5-0 chromic gut suture (or a 4-0 Vicryl suture, preferred by EL) is woven at the tip of each pedicle, like a rod through a window curtain. The needles are then passed through the subperiosteal plane and are either sutured to the periosteum (
). After the fat pads have been exposed, blunt dissection of the orbital rim with exposure of the arcus marginalis is performed. The periosteum is incised using monopolar cautery or using a blunt curved scissor. Dissection in the subperiosteal plane is performed with the aid of a Cottle or Freer elevator (see Fig. 5.11 B). Electrocautery with a fine tip can be used at low energy settings to control bleeding vessels that arise from dissecting the periosteum to reach the relatively avascular subperiosteal plane. It is in this plane that the dissection is carried out medially and laterally based on the skin markings placed during preoperative preparation. Care should be taken to avoid trauma to the infraorbital nerve and vessels (typically located 2.7 cm from the midline and 0.9 cm inferior to the orbital rim). Again, care must be taken to avoid trauma to the inferior oblique muscle, which is situated between the medial and central fat pads. Once the pedicles are completely delineated and dissected, a double-armed 5-0 chromic gut suture (or a 4-0 Vicryl suture, preferred by EL) is woven at the tip of each pedicle, like a rod through a window curtain. The needles are then passed through the subperiosteal plane and are either sutured to the periosteum (  and ) or externalized (see ) for temporary anterior fixation (see Fig. 5.11 C and D). If externalized, the sutures can be tied over a bolster dressing to prevent the suture from eroding through the skin. These sutures can be removed in 5 days.
and ) or externalized (see ) for temporary anterior fixation (see Fig. 5.11 C and D). If externalized, the sutures can be tied over a bolster dressing to prevent the suture from eroding through the skin. These sutures can be removed in 5 days.

Related posts:
 Preoperative assessment of the face, neck, and eyes
Preoperative assessment of the face, neck, and eyes
 Upper eyelid blepharoplasty
Upper eyelid blepharoplasty
 Thread lifting
Thread lifting
 The modern neck lift without a facelift
The modern neck lift without a facelift
 Non-surgical skin tightening and resurfacing: Lasers, chemical peels and other devices
Non-surgical skin tightening and resurfacing: Lasers, chemical peels and other devices
 Facelift: Superficial and deep plane with and without resuspension of the retaining ligaments—a practical step-by-step guide
Facelift: Superficial and deep plane with and without resuspension of the retaining ligaments—a practical step-by-step guide
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


