Synopsis
- ▪
Always consider the defect when planning a flap.
- ▪
Assess availability and laxity of local tissue.
- ▪
Rob Peter to pay Paul but only if Peter can afford it.
- ▪
Match the flap to the defect, not the defect to the flap.
- ▪
Keep your reconstruction as simple as possible.
- ▪
Good cosmesis is vital, but function trumps cosmesis.
- ▪
Do not burn bridges.
- ▪
If unsure of how to proceed, for whatever reason, use a temporizing approach.
Cheek reconstruction
- ▪
Local tissue should be used whenever possible.
- ▪
Local and regional flaps work well.
- ▪
Color match is important.
- ▪
For composite defects of lips and cheeks, each component defect can be reconstructed as a separate unit.
Lip reconstruction
- ▪
Accurate three-layered closure of lip defects is imperative to preserve function.
- ▪
Local tissue should be used whenever possible.
- ▪
Small defects can be closed by direct repair:
- •
Defects up to 25% of the width of the upper lip can be closed.
- •
Defects up to 30% of the width of the lower lip can be closed.
- •
- ▪
Intermediate defects are best reconstructed with local flaps.
- ▪
Total or subtotal lip defects are best reconstructed with free tissue.
Keywords
Face, Flap, Local, Adjacent, Rotation, Transposition
Synopsis
- ▪
Always consider the defect when planning a flap.
- ▪
Assess availability and laxity of local tissue.
- ▪
Rob Peter to pay Paul but only if Peter can afford it.
- ▪
Match the flap to the defect, not the defect to the flap.
- ▪
Keep your reconstruction as simple as possible.
- ▪
Good cosmesis is vital, but function trumps cosmesis.
- ▪
Do not burn bridges.
- ▪
If unsure of how to proceed, for whatever reason, use a temporizing approach.
Cheek reconstruction
- ▪
Local tissue should be used whenever possible.
- ▪
Local and regional flaps work well.
- ▪
Color match is important.
- ▪
For composite defects of lips and cheeks, each component defect can be reconstructed as a separate unit.
Lip reconstruction
- ▪
Accurate three-layered closure of lip defects is imperative to preserve function.
- ▪
Local tissue should be used whenever possible.
- ▪
Small defects can be closed by direct repair:
- ▪
Defects up to 25% of the width of the upper lip can be closed.
- ▪
Defects up to 30% of the width of the lower lip can be closed.
- ▪
- ▪
Intermediate defects are best reconstructed with local flaps.
- ▪
Total or subtotal lip defects are best reconstructed with free tissue.
Brief introduction
- ▪
Flaps on the face have many designs, and these are related to the area to be reconstructed and the size of the defect. It must not be forgotten, however, that there are only certain basic well-defined tissue manipulations; these are based on the concepts of advancement, transposition, and rotation (
 ;
;  ).
).
- ▪
When a wound is closed tightly or a flap which seems too small is used and yet the defect is closed, the biomechanical properties of creep and stress relaxation have been harnessed, and the skin elongates over time ( Table 10.1 ).
Table 10.1
Viscoelastic properties of the skin
Creep
When a sudden load is applied and kept constant, skin will stretch.
Stress relaxation
A constant load on the skin will cause lengthening. With time, the load required to maintain the lengthening decreases. This explains why white flaps will frequently become pink with time.
- ▪
For simplicity, key concepts for facial coverage will be grouped according to anatomic area.
Forehead and scalp
- ▪
The characteristics of the forehead vary considerably with age and nationality.
- ▪
All foreheads have a limited amount of spare skin, and, as a result, wide undermining and freeing are necessary to deal with many skin defects.
- ▪
The forehead is surrounded by a frame with distinct outlines, mainly of hair that should not be disturbed, where possible.
Technical pearls
- ▪
In the forehead, vertical donor sites are preferred to horizontal sites, which may cause an upward shift of the eyebrows or downward repositioning the forehead hairline ( Fig. 10.1 ) .
- •
Bilateral horizontal advancement flaps can be designed to take advantage of naturally occurring rhytids ( Fig. 10.2 ) . The flap should be designed equal to the size of the defect. Small Burrow triangles can be added to allow greater advancement and reduce dog ear formation.



Figure 10.2
(A–C) Bilateral horizontal advancement flaps can be designed to take advantage of the naturally occurring rhytids.
- •
Hatchet flap reconstruction can also be utilized and often requires two flaps, with opposing pedicles, i.e., one superiorly based and one inferiorly based ( Fig. 10.3 ) .





Figure 10.3
Nevus of left supraorbital area involving eyebrow–hatchet flap reconstruction. (A) The planned excision has been drawn out together with bilateral hatched flaps. (B) Nevus has been excised. It can be seen that the flap pedicles are superior for the lateral flap and inferious for the medial flap. (C) The flaps are elevated. (D) The flaps are transposed, and the secondary defect is closed. (E) Satisfactory end result with the eyebrow in a good position.
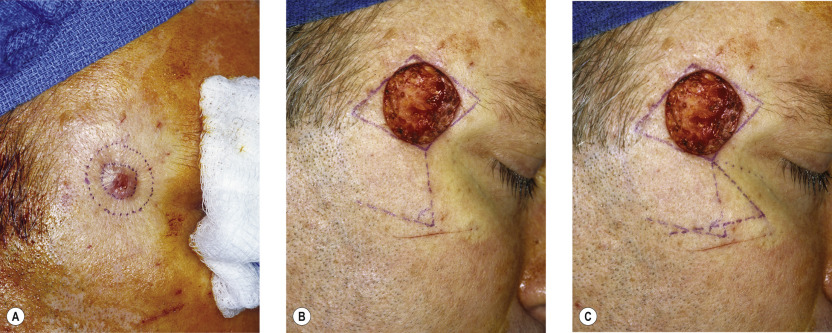
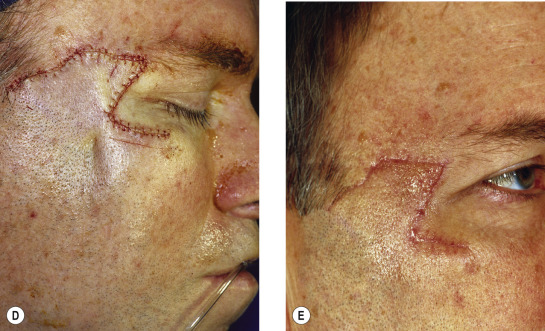
Figure 10.1
Rhomboid flap. (A) Melanoma in situ right temple. (B,C) Lesion excised. Limberg flap designed for repair of 2×2 cm defect. (D,E) Dufourmentel flap designed and transferred to defect.
- •
- ▪
In larger defects, a triple rhomboid may be used; this necessitates an excision of a hexagonal design ( Fig. 10.4 ) .
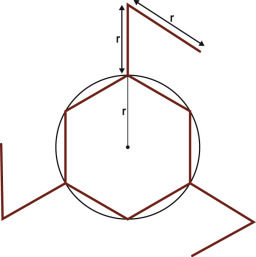
Figure 10.4
Triple rhomboid flap. Circular cutaneous defect conceptualized as hexagon. Sides of hexagon are equal to radius (r) of circle. First side of flap created by direct extension equal in length to radius at alternative corners to prevent sharing of common sides. Second side of flap designed parallel to adjacent side of hexagon.
(From Bray DA. Rhombic flaps. In: Baker SR, Swanson NA, eds. Local Flaps in Facial Reconstruction. St Louis: Mosby; 1995:155, Fig 6, with permission.)
- ▪
Careful planning and assessment of the availability of loose skin in all three areas of flap harvest is essential.
- ▪
In the temporal area, 3.5-cm flaps can be used, but this requires great care in order to prevent too great a shift of the hairline. This applies to reconstruction of any area on the non-hair-bearing scalp in proximity to the hairline edge ( Fig. 10.5 ) .
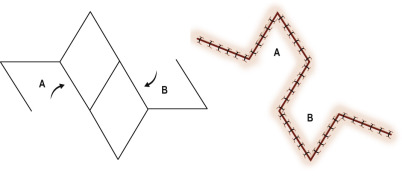
Figure 10.5
Bilateral rhombic flaps designed for repair of large defect. Defect divided into two adjacent rhombuses (A,B) to assist with designing rhombic flaps.
- ▪
Direct advancement flaps are possible but can only close smaller defects.
- ▪
Island flaps are used only occasionally; they are frequently based on subcutaneous tissue rather than on definite blood vessels. This necessitates taking great care to maintain every subcutaneous strand possible, and tension must be minimized.
- ▪
Bilobed flaps can be used, but they tend to trapdoor or pincushion and are therefore obvious in any form of indirect lighting.
- ▪
Large forehead reconstruction is treated by tissue expansion; this allows reconstruction by simple advancement or one of the expanded flaps described previously ( Fig. 10.6 ) .



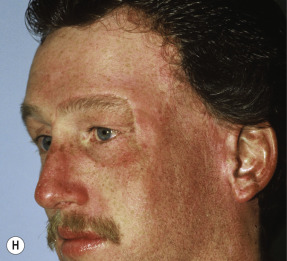
Figure 10.6
Tissue expansion to achieve defect closure. (A,B) Skin graft covering temple, anterior parietal scalp, and lateral cheek. (C) Expanded forehead skin. (D) Following tissue expansion, expanded forehead skin used to cover defect created by partial resection of skin graft. (E) Expansion provided sufficient skin to cover temple. (F) Tissue expander beneath lateral cheek skin. (G) 6 days following removal of skin graft from cheek and reconstruction with expanded cheek advancement flap. (H) 6 months postoperative.
- ▪
Post-expansion size increases will decrease when the expander is removed, and this must be taken into consideration when planning the reconstruction. Thus, a degree of over-expansion is strongly advised.
Eyebrow reconstruction
- ▪
The eyebrow is complex, and reconstruction is difficult; this is because hair grows in a fixed pattern that is not uniform and is difficult to reproduce exactly.
- •
Hatchet flaps may be a great option in this location, as the proper design can prevent elevation of the brow.
- •
Technical pearls
- ▪
A scalp island flap based on the temporal blood supply can be used, but the hair must be trimmed.
- ▪
The hair is often too dense and does not grow in the correct manner; however, the reconstructed eyebrow can be much appreciated by the patient, especially in the burned patient in whom both eyebrows are frequently involved.
- ▪
An alternative technique is micro-hair transplants with frequent trimming. These, unfortunately, rarely produce the unique anatomy and the density of the eyebrow hair.
Nasal reconstruction
- ▪
Many different flaps for nasal reconstruction have been described. In some cases, flap selection can be narrowed based on location of the defect ( Table 10.2 ).
Table 10.2
Flap selection for nasal reconstruction with local and regional flaps based on location
Proximal third of the nose
Central
Horizontal defect: dorsal nasal flap
Round defect: glabella flap
Vertical defect: V-Y flap
Lateral
Horizontal defect: glabella flap, first choice; dorsal nasal flap, second choice
Vertical defect: V-Y flap
Combined defect: gorehead flap
Middle third of the nose
Central
Horizontal and round defect: dorsal nasal flap
Vertical defect: V-Y flap
Lateral
Horizontal defect: dorsal nasal flap
Vertical defect: V-Y flap, first choice; nasolabial flap, second choice
Combined defect: forehead flap
Distal third of the nose
Alar defect: nasolabial flap, first choice; V-Y flap, second choice
Domal-alar groove defect — nasolabial flap, first choice; V-Y flap, second choice
Dome defect: bilobed flap
Central tip defect — bilobed flap
Columella defect: composite graft, skin graft, ascending helical free flap
Nasal sill defect: nasolabial flap
Combined defect forehead flap, first choice; nasolabial or extended V-Y flap, second choice
Technical pearls
- ▪
In the bridgeline region, the glabella is the preferred donor site, and the variety of flaps can be the direct advancement type ( Fig. 10.7 ) , transposition ( Fig. 10.8 ) , bilobed ( Fig. 10.9 ) , rhomboid (see Fig. 10.1 ), or island ( Fig. 10.10 ) .

Figure 10.7
Reconstruction of nasal defect with lateral advancement flaps. (A) 0.5×0.5 cm skin defect of nasal tip. (B) Primary wound closure planned. Anticipated standing cutaneous deformities (marked by horizontal lines). (C) Deformities excised and wound closed. (D) 1.5 years postoperatively.


Figure 10.8
Reconstruction of lateral nasal defect with forehead flap. (A,B) 1.5×1.5 cm skin defect of nasal tip. (C) Interpolated paramedian forehead flap used to repair defect. (D) 9 months postoperative. Depressed scar surrounds lateral aspect of flap, and mild trapdoor deformity is present. (E) Nose marked for planned contouring procedure. Three Z-plasties positioned along depressed scar. (F) Flap thinned and Z-plasties performed. (G,H) 4 months following Z-plasties and full-face carbon dioxide laser peel.


Figure 10.9
Closure of nasal defect with bilobed flap. (A) 1×1 cm skin defect of tip. (B) Bilobed flap designed for repair. Anticipated standing cutaneous deformity marked for excision in alar groove. Linear axis of each lobe designed 45° from each other with primary lobe axis positioned 45° from axis of defect. (C) Transfer of flap requires complete undermining of entire nasal skin. (D) Flap in place. (E) 1 year postoperative. No revision surgery performed.
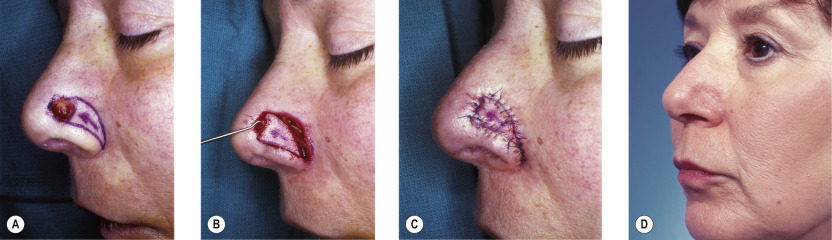
Figure 10.10
(A) 0.8×0.7 cm skin defect of alar groove. V-Y island subcutaneous tissue pedicle advancement flap designed for repair. (B) Flap incised and advanced on nasalis muscle. (C) Flap in place. (D) 4 months postoperative.
- ▪
On the lateral aspect of the nose, bilobed (see Fig. 10.9 ), rotation ( Fig. 10.11 ) , or transposition flaps ( Fig. 10.12 ) – all can provide excellent results. Fortunately, there is often more skin available in this area than expected.
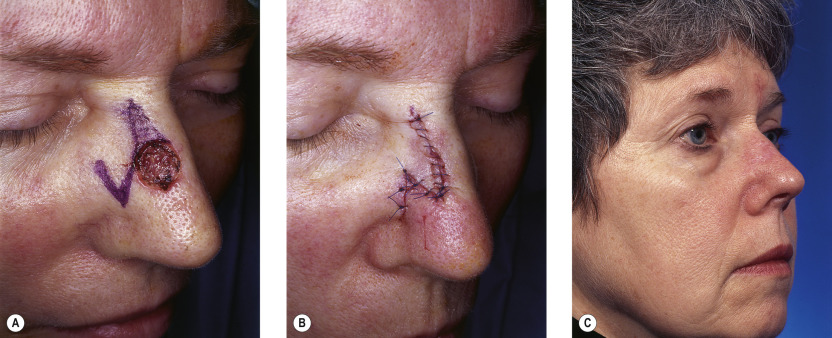
Figure 10.11
(A) 1×0.8 cm skin defect of the dorsum. Transoperative flap designed for repair. Anticipated standing cutaneous deformity marked by horizontal lines. (B) Flap transposed. (C) 6 months postoperative. No revision surgery performed.
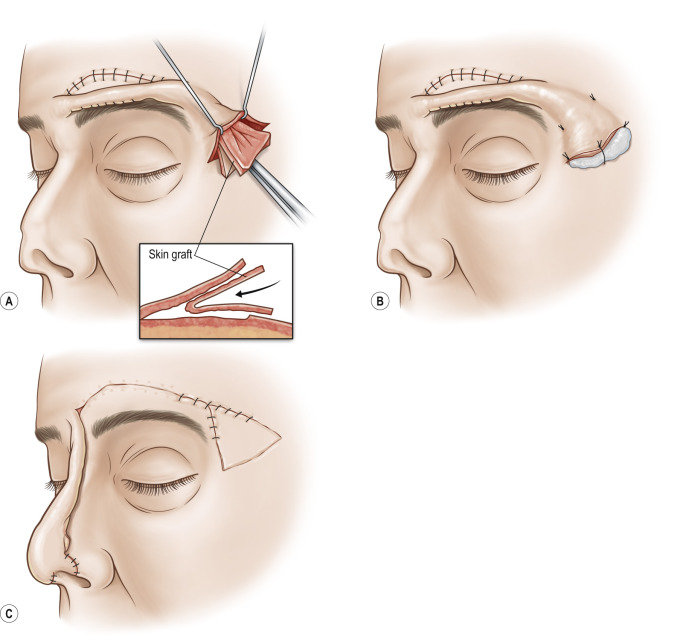
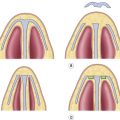
Figure 10.12
Transverse forehead flap for composite nasal tip defect. (A) At initial elevation of the flap, a septal mucosa graft is prelaminated within the distal flap to provide eventual nasal lining. (B) A bolster dressing is applied to the septal mucosa graft. (C) At a second stage, the flap is rotated and inset.
- ▪
To provide an acceptable nasal tip reconstruction, the bilobed flap is ideal, though, as already mentioned, it does have a tendency to trapdoor.
- ▪
The long advancement flap of Rintala, which looks unreliable, usually works well but can cause some apprehension on the part of the surgeon and the patient due to skin color changes (see Fig. 10.12 ).
- ▪
Laterally, a nostril is made by dissecting a skin pocket and lining it with a skin graft and cartilage, which will provide the required support if necessary.
- ▪
Approximately 2–3 weeks after the initial reconstruction, this composite is brought down to reconstruct the rim and the alar region (see Fig. 10.12 ).
- ▪
A composite graft from the ear is an excellent choice when the nostril is to be reconstructed.
- ▪
The maximal dimensions of a composite graft are approximately 1 cm 2 ; for defects greater than this, a composite flap of helical root is an excellent solution.
- ▪
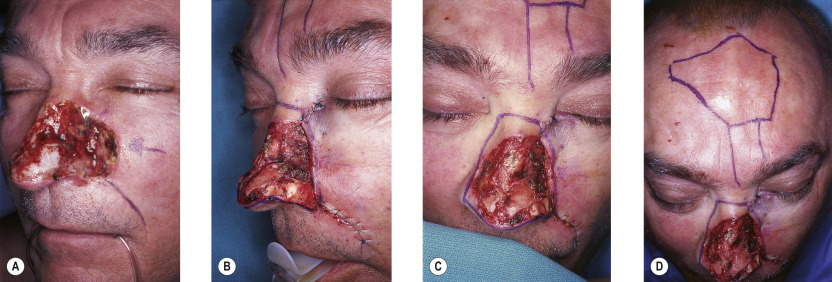
When a more complex reconstruction is required (e.g., bilateral alar rims and columella), the total central forehead should be used.
- ▪
The key to complete survival of the flap is the position of its base; this should be at the medial canthal level or below. In this way, the vascular anastomosis on the side of the nose between the cheek and forehead vessels is used to give length to the flap.
- ▪
The reason for poor results and failures is usually due to elevating the flap pedicle based on the brow area.
- ▪
The forehead is closed directly, but if there is tension in the area just anterior to the hairline, it should be left to close secondarily. The scar resulting from this rarely, if ever, requires any reconstruction.
- ▪
The pedicle is divided at 2–3 weeks, depending on the inset, and the nasal tip is fashioned. Apart from thinning, it is unusual to require further adjustments ( Fig. 10.13 ) .