Introduction
Traditional breast conservation therapy (BCT), consisting of lumpectomy, sentinel lymph node biopsy, possible axillary dissection, and radiation therapy, is medically equivalent to mastectomy with regard to overall long-term survival rates and has been the recommended treatment of choice for women with early-stage breast cancer. BCT has always focused on optimizing cosmetic goals and minimizing the psychological morbidity of a mastectomy, while maintaining low rates of local recurrence. Historically, BCT was only performed when adequate tumor-free margins could be obtained with cosmetically acceptable results. Although large tumor size alone is not considered a contraindication for BCT in terms of local tumor control, it is an important variable in obtaining good cosmetic results. Specifically, the breast volume excised in relation to total breast volume directly correlates with cosmesis and patient satisfaction after BCT. The site of the breast tumor also plays a role in anticipating poor aesthetic outcomes, such that medial tumors lead to more unfavorable cosmesis. Oncoplastic techniques have extended the indications of breast conservation therapy in the modern day management of patients with breast cancer. Combining wide resection of breast parenchyma with simultaneous reconstruction of the defect, oncoplastic breast surgery avoids significant risk of local deformity, thereby preserving aesthetics while increasing the accuracy of local disease control.
The critical factor in achieving an oncologically sound resection is tumor margin clearance. Achieving oncologic clearance with increasing tumor size requires extensive breast volume resection, resulting in large partial mastectomy defects requiring reconstruction using volume displacement or volume replacement techniques. Volume displacement, described in a previous chapter, uses local glandular or dermoglandular rearrangement to fill the resection defect. Depending on the amount of breast volume resected, a simultaneous contralateral reduction may be required to achieve symmetry. Surgical resection ultimately reaches a maximum volume limit when volume displacement techniques will not be adequate to achieve an aesthetically pleasing result, even if the contralateral breast is reduced for symmetry. In these cases, volume replacement techniques are necessary to restore breast shape and contour. These techniques use autologous tissue to replace the volume of excised breast parenchyma. As the volume is restored, contralateral surgery is rarely required to achieve symmetry. Volume replacement reconstruction techniques are being employed more frequently as the indications for breast conservation therapy are extended to include larger T2 and T3 breast tumors, including those treated with adjuvant chemotherapy or radiation. Unfortunately, some patients present requesting reconstruction for an unforeseen cosmetic defect after completion of BCT and radiation. These patients also benefit from autologous tissue transfer for volume replacement. This chapter focuses on the latissimus dorsi (LD) flap, the most commonly used autologous tissue in volume replacement reconstruction of the partial mastectomy defect following breast conserving surgery.
The LD flap was first described by Tansini in 1897. Evolving over the past century, this flap has been used reliably to cover soft tissue defects as a free or pedicle-based myocutaneous or myofascial flap. The harvesting technique, which involves a large dorsal skin incision for flap elevation, has remained essentially the same since its initial introduction for soft tissue coverage of anterior chest wall defects. The conventional technique, although clearly efficacious, results in a large oblique back scar that can be troubling to a woman concerned with cosmesis. In an era of oncoplastic breast resection and in a quest to combat unwanted scarring, the LD flap may also be harvested through an endoscopic approach.
The use of endoscopes to assist in partial mastectomy defect reconstruction has been effectively used at our institution since 1994. The endoscopic assisted reconstruction with latissimus dorsi (EARLi) flap technique, originally performed by the senior author after BCT, uses a much smaller incision ( Fig. 8.1 ) than the open technique and is performed with the use of modified instruments used in endoscopic cholecystectomy surgery ( Fig. 8.2 ). Less traumatic tissue dissection in conjunction with smaller surgical incisions have enabled many patients to benefit from reduced postoperative pain, expedited recovery, and improved cosmesis. By comparison with other surgical disciplines, plastic surgery has been slower to adopt minimally invasive techniques, in part due to the limited surgical apertures, confined optical cavities, and difficult anatomical exposures required in many of the reconstructive procedures. Improvement in general endoscopy in recent years and the addition of tumescent fluid has resulted in striking new advances in the technique of endoscopic latissimus harvest.


BCT and reconstruction with the LD flap is an oncologically safe treatment for patients with early-stage breast cancer and those with larger T2 and T3 breast cancers. At our institution, if a skin paddle is not necessary then we prefer the EARLi flap technique to achieve a favorable cosmetic outcome with little scarring. Because of the small incision and limited soft tissue dissection, postoperative pain is reduced and recovery time is diminished. Whether harvested through an open or endoscopic approach, the principal goals of the LD flap for reconstruction of partial mastectomy defects are to replace excised tissue volume and prevent breast deformity. In addition, breast size and contour are maintained, and scar tissue contracture is minimized.
Indications and contraindications
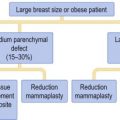
Significant volume loss after BCT surgery can result in a partial mastectomy defect requiring reconstruction with volume displacement or volume replacement oncoplastic techniques. Certain patients can be anticipated to have poor aesthetic outcomes after BCT. Recognizing patient and treatment-related risk factors at the time of consultation can optimize surgical planning and reconstructive options. Patient risk factors include large tumor size, patients with small breast to tumor ratios and tumor position, specifically superior medial tumors, and inferior lateral tumors. Although there is a trend toward managing larger breast tumors with BCT, one of the major limitations is the ability to perform a large enough resection without compromising the cosmetic result. If anticipated breast volume excised is greater than 10–20%, then reconstruction should be planned. Excising this amount of tissue in a small to medium-breasted woman without ptosis precludes the use of volume displacement techniques, whereas an LD flap reconstruction will provide optimal contour and shape. Treatment-related risk factors may include patients presenting with breast deformity following multiple re-excisions for positive margins or following the radiation phase of BCT. Delayed reconstruction after radiation treatment is best managed with volume replacement using autologous tissue. In this situation, the LD flap will not only provide non-irradiated supple skin but also additional blood supply for adequate wound healing in an irradiated operative field.
Partial mastectomy defects reconstructed with volume displacement techniques will usually require a contralateral breast symmetry procedure. Patients who are not amenable to surgery on the contralateral breast are good candidates for breast volume replacement techniques. This indication for an LD flap achieves a good breast contour and shape while maintaining volume to match the symmetry of the opposite breast.
The LD flap is optimal for defects in the upper outer quadrant, the site of occurrence for approximately 75% of breast cancers. This type of reconstruction is least suited for breast defects in the lower inner quadrant, where less than 6% of breast cancers reside. A large cavity in the lower inner quadrant cannot be adequately filled with a pedicled LD flap.
Due to the reliable and robust blood supply of the flap, patients with comorbidities that would preclude transfer of other autologous tissues are considered safe candidates for pedicled latissimus dorsi reconstruction. We have used this flap safely in patients with diabetes, smokers and in obese patients. General contraindications to oncoplastic reconstruction with volume replacement techniques include patients with T4 tumors, multicentric disease, extensive malignant mammographic microcalcifications, inflammatory carcinoma and when clear margins cannot be assured without performing a mastectomy. The specific contraindications for an EARLi flap are essentially the same as those for a traditional LD flap. The exception occurs more in the event of delayed reconstruction. Patients presenting with radiation-induced deformities or other etiologies requiring need of a skin paddle for reconstruction are not candidates for the EARLi flap. Lack of latissimus musculature to adequately fill the oncologic resection defect would compromise breast shape and fail to achieve aesthetically pleasing cosmesis. This may be overcome with use of an implant or a contralateral breast-reducing procedure if the patient is amenable. Pedicle compromise is also a contraindication to the LD flap. A previous thoracotomy or axillary incision should raise the concern of an injured or ligated pedicle. The LD can survive on flow through the serratus branches if the thoracodorsal is the only vessel injured, but this would have to be carefully evaluated at the time of surgery. Other options for reconstruction would have to be discussed at the time of initial consultation in anticipation of previous injury to both arterial supplies.
Because the LD muscle is transferred, muscle function may be compromised, but functional deficits are only seen with specific activities. This flap would have relative contraindications in women active in sports requiring extreme upper body strength, such as mountain climbers, rowers and competitive swimmers, because muscle weakness can be seen in these patients.
Preoperative history and considerations
Oncoplastic surgery is a new paradigm shift created in the evolution of multidisciplinary contributions to advancing breast cancer treatments. Conventionally, the breast surgeon ensured oncologic resection of the tumor and the patient was referred to a plastic surgeon for aesthetic breast reconstruction. Due to the new sub-specialty of oncoplastic surgery, oncologic principles and aesthetics are merging. There remains ambiguity as to the boundaries of breast surgeons and plastic surgeons when reconstructing a breast defect. Regardless, as the reconstructive surgeon, there are several underlying principles to understand and apply when initially evaluating a patient who is to receive BCT. To effectively care for these patients, the surgeon must be able to visualize the anticipated defect, all of its reconstructive options and be able to treat all potential postoperative complications.
Preoperative knowledge of the tumor location and size in comparison to the native breast volume is of high importance since volume displacement procedures are only suitable for patients with enough remaining healthy breast tissue to allow reconstruction of the breast. Discussing with patients their desires of having a symmetry procedure to the contralateral breast is necessary in the decision regarding reconstructive options. Volume replacement techniques such as the LD flap will be more suited to women who do not desire surgery to the opposite breast and who have large tumor to breast volume ratios. The location of the tumor plays a role in reconstructive options as medial lower quadrant defects in a patient with insufficient volume for breast displacement procedures will not be a good candidate for LD flap reconstruction and would be better served with autologous tissue from the abdomen.
Once volume replacement reconstruction is decided, patient history and desire will dictate whether LD reconstruction is chosen. Careful examination and past medical history will reveal any previous surgeries which may have compromised the vascular supply to the flap. Thoracotomy or axillary scars may preclude use of the thoracodorsal pedicle. Patients should be warned of the large donor site scar and given the option of an endoscopic approach. In the event of recurrence and need for a mastectomy, the option of an ipsilateral pedicled LD flap breast reconstruction will no longer be possible. In patients who desire autologous reconstruction, evaluation of the abdominal tissues is necessary, so that in the event of recurrence and completion mastectomy they may be easily reconstructed with TRAM flaps.
A patient may present for consultation after completion of breast conservation therapy with a significant breast deformity. This type of secondary reconstruction for radiated partial mastectomy deformities can be more difficult to correct. The breast resection not only creates loss of volume, but the radiation results in soft tissue scarring and contracture which may distort the nipple–areola complex. These patients will often need a skin paddle in addition to soft tissues for volume replacement and therefore will not qualify for an endoscopic approach. It is not advisable to offer these patients delayed breast displacement techniques as the complication rate averages 50% due to decreased healing properties of the irradiated local tissues.
Timing of the partial mastectomy defect reconstruction using the LD flap is a critical component to success with this technique. The reconstruction is performed only after wide local excision and confirmation of final pathology reports. It should not be used simultaneously at the time of initial tumor resection before final margins are confirmed. With immediate reconstruction it is difficult to locate the position of a positive tumor margin. If the final pathology is back, the procedure can be performed early in the postoperative period, as early as 3 days after oncologic resection. However, it may also be performed as a delayed–immediate reconstruction as long as 3 weeks after tumor resection to accommodate patient preference for timing of surgery. This approach will not sacrifice an important reconstructive modality if the breast and flap need to be removed to obtain adequate tumor margins. While a short interval between lumpectomy and LD flap reconstruction is important, it is advantageous to carry out the flap prior to the formation of scar contracture in order to obviate the need for a skin paddle to release contracted skin.
Reconstruction with an LD flap does not affect postoperative cancer surveillance, which is important since some studies have found 2-to 3-year local recurrence rates to be as high as 13–15% when using an LD flap for volume replacement. This number seems high when compared to the reported 8–22% 18-year recurrence rates following traditional lumpectomy techniques. Our institution-based local recurrence rates correlate more with the 6% rates seen in the literature following displacement oncoplastic techniques. We believe that local recurrence rates are institution based due to different resection techniques and patient selection variations. Many of the patients receiving LD flap volume replacement have larger tumors and may be better served with a mastectomy and reconstruction. If an LD reconstruction is chosen, then higher chances of local recurrence will need to be discussed with the patients. To reduce the rate, breast tumor resection is best treated with oncoplastic techniques rather than by simple lumpectomy. If larger volumes are removed, such as in the case of a partial mastectomy or quadrantectomy, then wider margins will naturally be obtained, resulting in lower rates of local recurrence. Invariably, local recurrences will continue to occur throughout the follow-up period, so close surveillance is warranted. Recurrence may present as a palpable nodule that can be easily biopsied for pathologic review. For non-palpable recurrences, women treated with LD flap reconstruction after BCT have mammographic findings that are predictable. The most common radiographic appearances are relative radiolucency in the central portion of the flap due to fibrofatty degeneration, with or without density from muscle fibers at the periphery of the transferred LD.
Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Timing and Key Considerations in Reconstruction for Breast-Conserving Therapy
Timing and Key Considerations in Reconstruction for Breast-Conserving Therapy
 Breast Augmentation Technique (Biplanar) for Oncoplasty
Breast Augmentation Technique (Biplanar) for Oncoplasty
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
 Complications of Oncoplastic Breast Surgery
Complications of Oncoplastic Breast Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


