and Frank Hölzle2
(1)
Department of Oral and Maxillofacial Surgery, Klinikum rechts der Isar, Technische Universität Munich, Munich, Germany
(2)
Department of Oral and Maxillofacial Surgery, University Hospital of RWTH Aachen University, Aachen, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-53670-5_4) contains supplementary material, which is available to authorized users.
4.1 Development and Indications
This first septocutaneous flap was originally introduced in 1982 by Song and coworkers [507] and 2 years later was described in more detail by Katsaros et al. [262]. Similar to the radial forearm flap, the lateral upper arm flap is relatively thin, but limited in width, and can be transferred together with a segment of bone, muscle, or sensory nerves. The flap, which is raised at the lateral aspect of the upper arm, is perfused by the terminal branches of the profunda brachii artery. This artery is not essential for the vascularity of the extremity. Early clinical series document a number of application possibilities, especially in the head and neck area [107, 109, 349, 483, 494, 577]. Because of its texture and the favorable color match, the flap is well suited for replacement of the facial skin [507]. At the extremities, the upper arm flap is useful for defect coverage on the foot, hand, or forearm as a free flap [310, 484, 406, 475, 577] or as a pedicled flap for coverage of defects at the shoulder region [109, 577]. For defect coverage at the temporal region, Inoue and Fujino left the flap pedicled on the cephalic vein, whereas the flap artery was microsurgically anastomosed to a neck artery [248]. Apart from these indications, the lateral upper arm flap can be used for a number of intraoral reconstructions. Matloub and coworkers reported on six reconstructions following partial or total glossectomy or defect coverage at the hard palate [349]. By connecting the posterior cutaneous nerve of the arm to the lingual nerve, they could achieve a neurocutaneous reinnervation. Including a cortical segment of the humerus, a limited amount of bone can be harvested together with the skin paddle, which was used for lower jaw reconstruction [349, 577]. Other authors confirmed the usefulness of the lateral upper arm flap for intraoral reconstructions in larger clinical series [98, 200, 431], especially the high success rate of neurocutaneous reinnervation after nerve coadaptation [98]. When extending the flap to the proximal forearm, the thin and pliable forearm skin can be combined with the thicker flap portion of the upper arm [98]. Moffett and coworkers demonstrated the possibility of dividing the flap, which can then be used for closure of through-and-through defects of the oral cavity [378].
4.2 Anatomy
The lateral upper arm flap is nourished by septocutaneous branches of the posterior radial collateral artery (PRCA), which develops from the profunda brachii artery. The cutaneous branches of the flap are running within the lateral intermuscular septum, which separates the brachialis from the triceps muscles. According to Myong, the profunda brachii artery branches off from the brachialis artery as a singular vessel in 52%, or together with the ulnar collateral artery in 30% [411]. In 8%, the vessel was found to branch off directly from the axillaris artery and different studies describe a double profunda brachii artery with an incidence of 4–12% [262, 378, 440]. In these seldom cases, temporary occlusion of each of the arteries has to be performed to test their contribution to flap perfusion [378]. The proximal diameter of the artery varies from 0.9 to 2.5 mm [107, 262, 411], measuring 1.2 [349] or 1.5 mm in average [107, 262]. In close proximity to the radial nerve, the vascular pedicle spirals around the humerus, and proximal to the lateral intermuscular septum, it divides into the small anterior and the stronger posterior radial collateral artery (PRCA). Whereas the small anterior radial collateral artery is traveling together with the radial nerve, the PRCA is the main nutrient artery of the flap, giving off the septocutaneous branches. After having traversed the septum at its base, the PRCA anastomoses with the interosseous recurrent artery, on which the flap can be perfused in a retrograde fashion. Because the proximal segment of the profunda brachii artery is running underneath the long and lateral head of the triceps muscle, dissection of the vascular pedicle to a proximal direction can be difficult. The average length of the pedicle which is not covered by the triceps muscle thus is 7–8 cm [349, 378]. By longitudinal splitting of the above-mentioned triceps heads, the profunda brachii artery and veins can be followed up to the brachial vessels, obtaining a 6–8 cm longer pedicle [378]. It must be mentioned, that this maneuver can lead to a reduced strength of the operated arm, possibly following injury of muscular branches of the radial nerve [378]. The posterior cutaneous nerve of the arm (PCNA), which accompanies the PRCA and always has to be sacrificed during flap elevation, can be used to create sensate flaps [349, 406, 507, 577]. The posterior cutaneous nerve of the forearm (PCNF) does not provide sensation to the flap and could be preserved during flap elevation, but due to technical reasons, this nerve is normally sacrificed too. Venous drainage is the most reliable by the comitant veins of the profunda brachii, because the cephalic vein mostly runs too far medially at the upper arm [406]. When outlining the skin paddle, flap axis is positioned along the intermuscular lateral septum, which is defined by the interconnecting line between the lateral epicondyle and deltoid insertion. Although the skin territory can be as large as 18 × 11 cm [349], flaps should always be located within the “zone of security,” extending 12 cm proximal to the lateral epicondyle and including one-third of the circumference of the upper arm [440, 577]. According to anatomic studies using dye injections, the distal extension of the flap is possible up to 8 cm inferior of the lateral epicondyle [307].The harvest of a cortical segment of humerus is technically possible, but only to a size of 10 × 1 cm, leaving a muscle cuff on either side of the septum to include periosteal vessels of the PRCA [107]. Direct closure of the donor site is only possible if the width of the flap does not exceed 6 cm. For aesthetic reasons, the use of a skin graft should be avoided in this area [406].
4.3 Advantages and Disadvantages
The lateral upper arm flap has a reliable and constant anatomy, and because of the good color match and similar texture, the flap is suitable for defect coverage at the face and neck. Compared to the radial forearm flap, the raising of this flap is technically more demanding due to the deeper location of the pedicle and its close relationship to the radial nerve. Using color Doppler sonography, origin, course, variations, and locations of the perforators can be studied to preoperatively assess the vascular anatomy [519], but this is rarely needed. Although in normal weighing patients the flap does carry only a thin layer of subcutaneous fat, the average thickness of the adipose layer is 1.3 cm [164], and a considerable amount of the subcutaneous fatty tissue can be found in adipose patients [406]. The possibility to create sensate flaps is considered an advantage, especially in tongue reconstructions [349]. The combination of the skin paddle with a segment of the humerus bone or triceps muscle may contribute to a wider indicational spectrum of the flap [107, 262]. The high and reliable vascularity of the fascia allows for raising of purely fascial flaps, which can be covered with split-thickness skin grafts [507]. These fascial flaps have proven to be useful in reconstructions of the ear and nose [98]. The main disadvantage of the flap is the limited length of the pedicle and the small diameter of the vessels, so that anastomoses can become difficult, especially following radical neck dissection [378, 406, 577]. Flap raising leads to sensory loss at the proximal and posterior aspect of the forearm, but this is mostly not emphasized by the patients. Although there is no functional limitation at the donor arm, strength and extension can be objectively reduced after transection of the triceps head. Another disadvantage is the limited width of the flap, so that another donor site should be considered if a broad flap is needed. As a solution to this problem, Katsaros proposed to divide a long flap and to position both skin islands adjacent to each other, so that the flap width is doubled and the donor site can still be closed directly [262]. Another possibility to overcome this problem is pretransfer skin expansion [494], but this technique cannot be performed in patients with malignant tumors needing primary reconstruction.
4.4 Patient Positioning
The upper arm is disinfected completely from the shoulder and axilla down to the distal forearm and brought in an abducted and supine position. In the elbow, the arm is moderately flexed. In this position, flap raising can be carried out simultaneously to tumor resection in the head and neck area. No specific preoperative measures are necessary for elevating the lateral arm flap, and there is no need to use a tourniquet.
4.5 Standard Flap Design
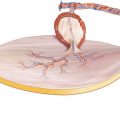
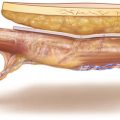
For most indications, the flap dimensions vary between 7 and 12 cm in length and 5 and 6 cm in width. The central axis of the skin island lies over the septum between the brachialis and triceps muscle (lateral intermuscular septum), which is represented by the interconnection of the lateral epicondyle and the insertion of the deltoid muscle. The skin paddle covers the biceps and brachialis muscle anterior and the lateral head of the triceps muscle posterior to the septum with a maximum width of 7 cm. The distal pole of the flap is outlined 1–2 cm proximal to the epicondyle, and the proximal pole is placed 4–6 cm below the deltoideus insertion. An incision is made for exposure of the proximal vascular pedicle (◘ Fig. 4.1).
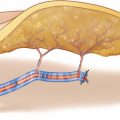
Incision Through Skin and Fatty Tissue
At the posterior circumference of the flap, the skin incision is made perpendicularly through the subcutaneous fatty tissue until the brachial fascia is reached. During the whole flap-raising procedure, the skin paddle may not be separated from the underlying fascia, which forms the intermuscular septum and thus contains the septocutaneous flap vessels (◘ Fig. 4.2).
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


