Case 1
Clinical Presentation
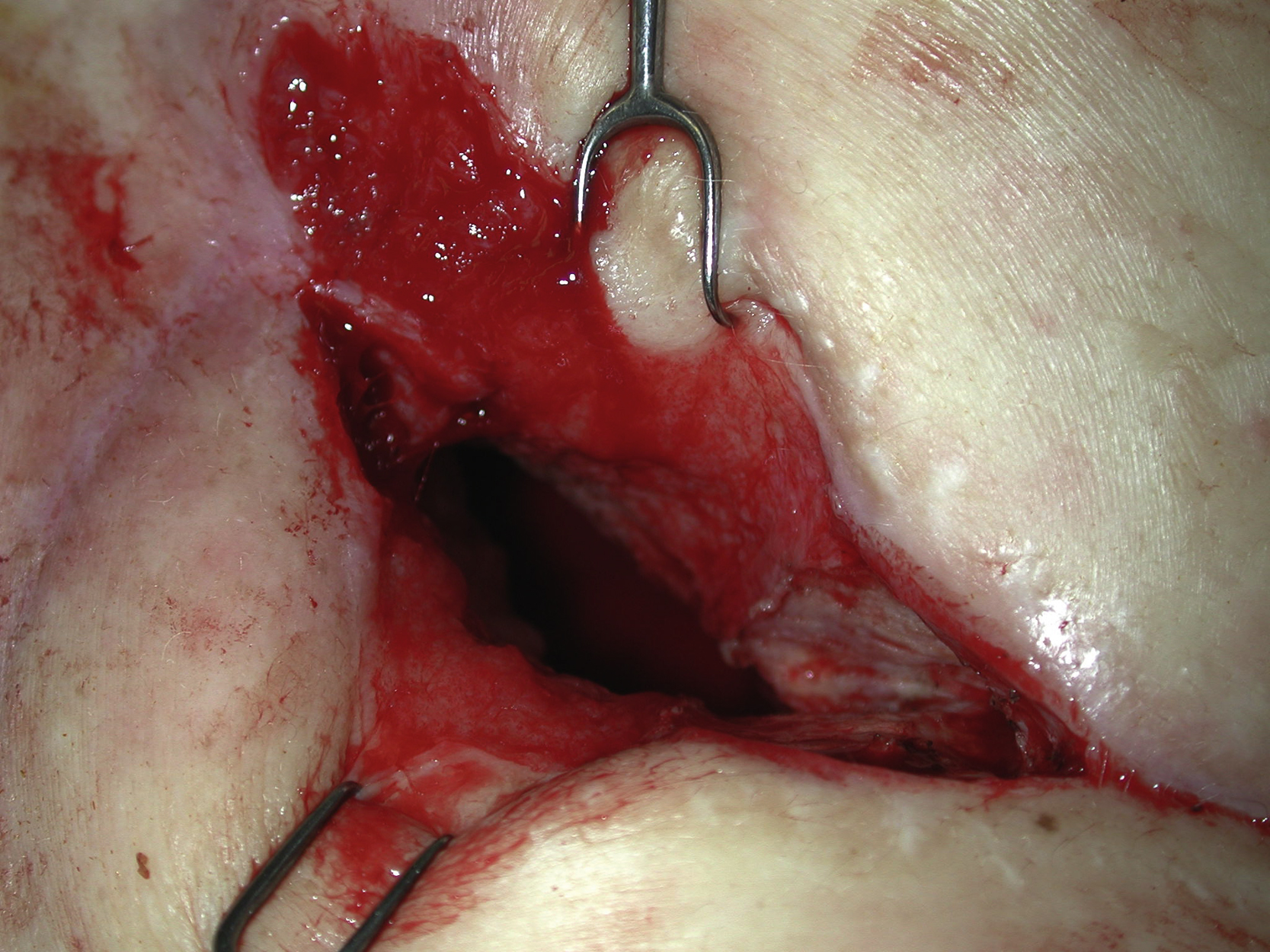
A 49-year-old White female underwent right total pneumonectomy for stage IIIA nonsmall cell lung cancer. She had preoperative radiation and chemotherapy for treatment of her advanced cancer. About 2 weeks postoperatively, she was found to have right bronchopleural fistula with air leak and vancomycin-resistant enterococcus infection as well as methicillin-resistant Staphylococcus aureus infection. A right thoracoplasty was performed initially by the thoracic surgeon to control the bronchopleural fistula. She had a very complicated hospital course including emergent cardiopulmonary bypass to control the bleeding from the right pulmonary artery stump. The plastic surgery service was asked by the thoracic surgery service to help the chest wound closure after repair of the bronchopleural fistula site ( Fig. 24.1 ). The primary service determined that the patient was stable enough to proceed to a more definitive operation to control the bronchopleural fistula and to close the right chest wound.

Operative Plan and Special Considerations
After examining the open wound over the right lateral chest, it appeared that the most part of the open chest cavity was located in the lower chest and the actual fistula site was in the middle chest. A midabdominal transverse rectus abdominis musculocutaneous (TRAM) flap could be selected based on the right superior epigastric vessels. The reason for selecting a midabdominal TRAM flap was because of her previous lower abdominal midline scar and to ensure the near-total survival of the midabdominal TRAM flap based on its large periumbilical perforators. This myocutaneous flap, after de-epithelization of it skin paddle, might provide a large amount of vascularized tissue to seal the bronchopleural fistula site and to obliterate a large part of the pleural cavity. The midabdominal TRAM flap may be more reliable than a standard lower abdominal TRAM flap. It might be possible that all four zones of flap tissue could survive and the flap could be tunneled and placed entirely into the chest.
Operative Procedures
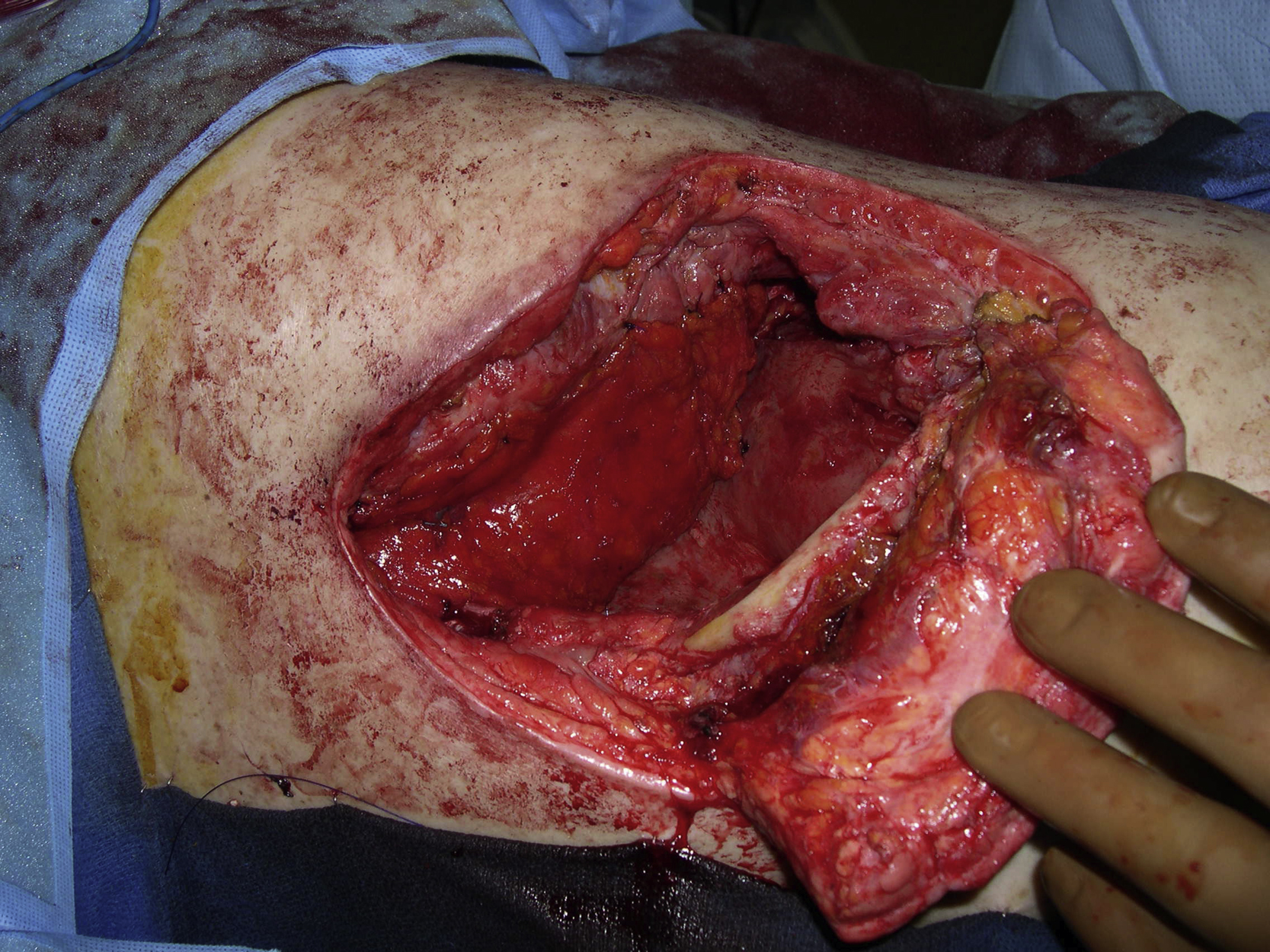
The patient was brought to the operating room by the plastic surgery service about 5 weeks after the right total pneumonectomy. Under general anesthesia with the patient in the left lateral decubitus position, careful debridement was performed to remove all necrotic, infected, or colonized tissues within the right chest. The patient was then placed in the supine position and a midabdominal TRAM flap was designed based on the right superior epigastric vessels ( Fig. 24.2 ). The skin paddle (30 × 12 cm) was elevated first. Once the incisions had been made through the anterior rectus sheath over the muscle, it was dissected free and its inferior insertion was divided. The entire flap was elevated, tunneled through the right subcostal area ( Fig. 24.3 ) and placed inside the right chest without tension after the skin paddle of the flap was de-epithelized. The flap donor site was closed in a standard fashion over two drains.


The patient was then placed in the left lateral decubitus position again. For an intrathoracic placement of the entire de-epithelized right midabdominal TRAM flap, zones 1 and 2 of the flap faced the site of the bronchopleural fistula and the stump of the pulmonary vessels and zones 3 and 4 faced outward. A chest tube was placed inside the chest. The muscle portion of the flap was wrapped around the repaired bronchopleural fistula site and sutured and the rest of the flap was then placed inside the chest with interrupted sutures ( Fig. 24.4 ). After some skin undermining and local tissue rearrangement, the right chest open wound was closed in two layers after intrathoracic placement of the midabdominal TRAM flap ( Fig. 24.5 ).

Follow-Up Results
Postoperatively the patient did well except she developed a deep venous thrombosis of the right upper extremity, which was treated accordingly. The air leak and infection appeared to be resolved. Repeated chest CT scans showed a good filling of vascularized soft tissue to the right middle and lower chest ( Fig. 24.6 ). The right chest wound repair site remained closed. She was discharged from the hospital 2 months later.

Management of Complications
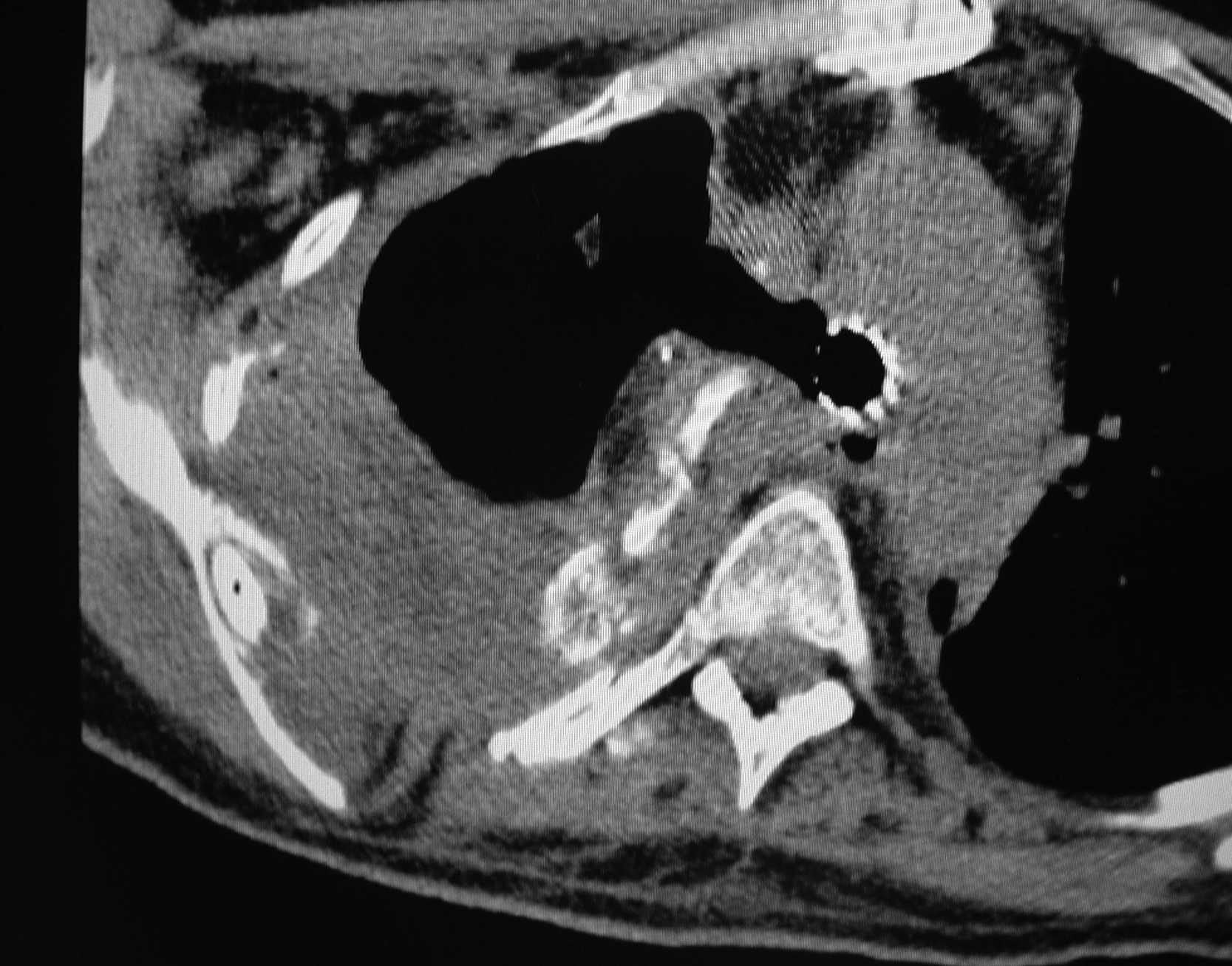
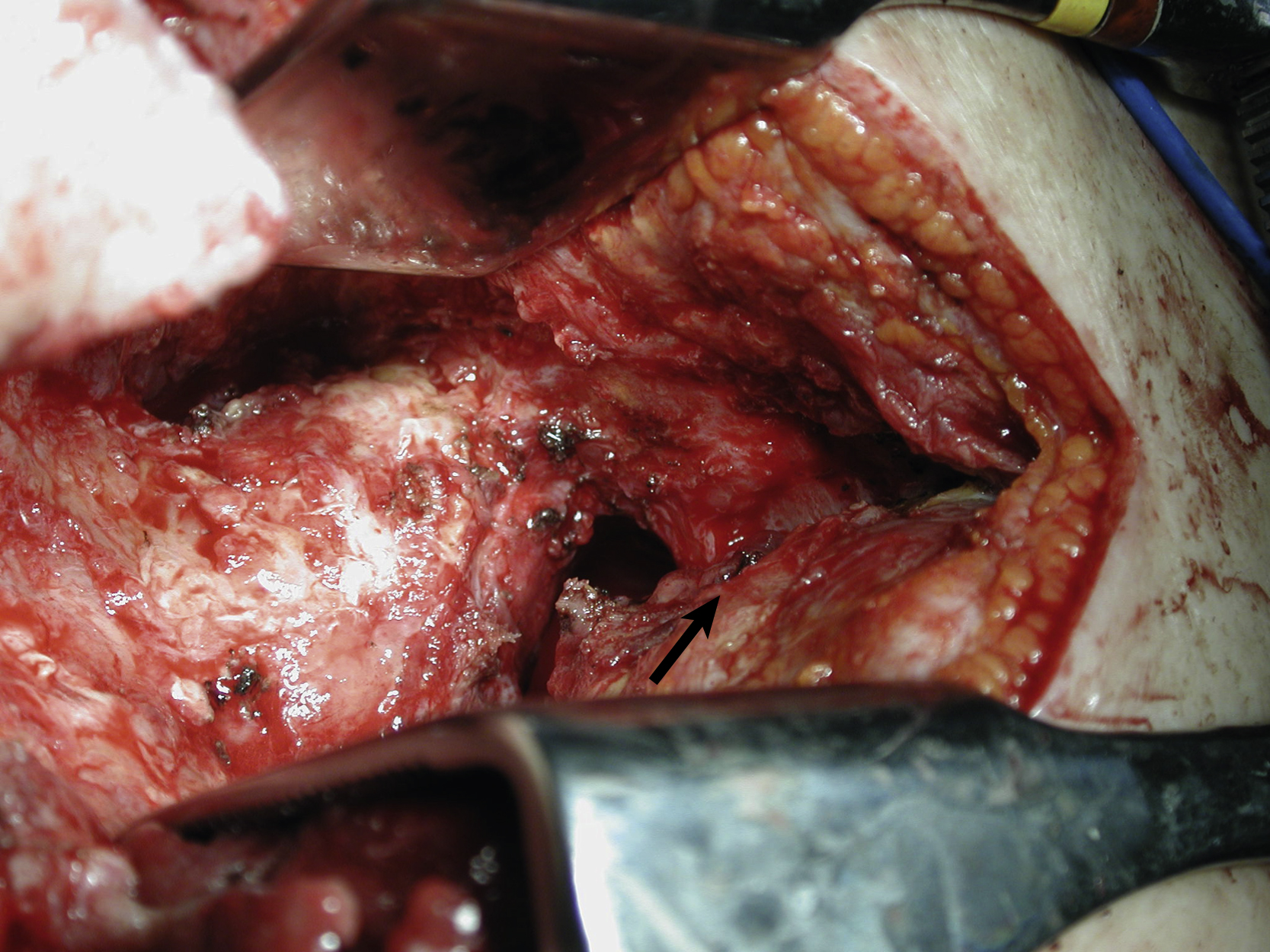
She unfortunately developed recurrent bronchopleural fistula about 4 months after the first flap surgery, with a small open wound on her right chest and a persistent air leak. She was otherwise doing well with no evidence of infection ( Fig. 24.7 ). Repeated chest CT scans showed a less optimal filling of the pleural cavity ( Fig. 24.8 ). At this point, it became clear that additional well-vascularized tissue would be required not only to seal the recurrent bronchopleural fistula but also to obliterate the remaining dead space within the thoracic cavity. She was brought to the operating room for the second intrathoracic flap transfer. During exploration, the recurrent bronchopleural fistula was identified ( Figs. 24.9 and 24.10 ) and repaired again by the thoracic surgery service with additional suture and fascial patch graft ( Fig. 24.11 ). Because of the previous right thoracotomy, the left latissimus dorsi myocutaneous flap was selected and elevated as a free flap ( Fig. 24.12 ). The right thoracodorsal vessels were explored for the recipient vessels. After successful end-to-end microvascular anastomoses for both artery and vein, the entire flap appeared to be well perfused ( Fig. 24.13 ). The de-epithelialized flap could be placed freely anywhere inside the pleural cavity. The repair site of the recurrent fistula was covered with the muscular portion of the flap and the remaining dead space was completely obliterated by the flap with the de-epithelized portion facing out ( Fig. 24.14 ). With concerns of the flap being buried inside the chest, it was observed for an hour in the operating room after both microvascular anastomoses before the chest wound was closed. It reassured the surgeon that both microvascular anastomoses were patent and there were no technical errors in the free tissue transfer. The chest wound was closed again in two layers after local tissue rearrangement ( Fig. 24.15 ). The patient tolerated the entire procedure well and was extubated the next day. She was found to have no further air leak after the second flap surgery and was discharged from the hospital 2 weeks postoperatively