Introduction: The Skin as an Immune Organ
Not only the skin is the largest organ of the body, the barrier against noxious influences from the environment, a sensory organ, and a metabolic organ, but it is also an immune organ: all the necessary constituents to produce an immune response are present in the skin. Epidermal dendritic cells (Langerhans cells) lie immediately under the stratum corneum and represent the outermost “sentinel” of our immune system. Furthermore, the skin contains different types of lymphocytes and dendritic cells in the dermis. In addition, the dermis homes mast cells and bystander cells, acting as effector cells. Keratinocytes have been shown to produce all kinds of cytokines and chemokines that play an important role in the immune response. Furthermore, there is ample capacity of innate immune responses like antimicrobial peptides (e.g., defensins) or dendritic cells with various pathogen reaction pattern receptors (e.g., toll-like receptors [TLRs]) to attract inflammatory cells such as neutrophilic leukocytes among others.
Under normal, healthy circumstances, this immune system is not sleeping; it is constantly regulated to stay in balance. Dendritic cells of the epidermis as well as regulatory T cells play an important role in this regulation and balance.
There are several ways in which this homeostatic balance can be disturbed—either by disruption of natural tolerance against self-antigens (autoimmunity) or by pathogenic immune reactions against foreign substances, be it small chemicals (haptens) or proteins leading to allergic skin diseases.
Allergic Skin Diseases
Allergy is defined as an immunologically mediated hypersensitivity reaction leading to disease and can be classified into several pathogenic types of immune reactions (modified according to Coombs and Gell):
Type I Immediate hypersensitivity, Immunoglobulin E (IgE)-mediated (urticaria, angioedema, anaphylaxis, allergic rhinoconjunctivitis, extrinsic bronchial asthma, atopic eczema (AE))
Type II Cytotoxic immune reactions (thrombocytopenic purpura, other hematologic allergies)
Type III Immune complex reactions (serum sickness, leukocytoclastic vasculitis, immune complex anaphylaxis, urticaria)
Type IV Cellular hypersensitivity
Type IVa T-helper-cells type1 (Th1)-mediated allergic contact dermatitis, delayed-type hypersensitivity
Type IVb T-helper-cells type2 (Th2)-mediated, atopic eczema (see also type I)
Type IVc CD8-mediated exanthematous and bullous drug eruptions
Type IVd Th17-mediated pustular drug eruptions (acute generalized exanthematous pustulosis [AGEP])
Type V Granulomatous skin reactions (e.g., to bovine collagen, tattoo reactions)
Type VI Stimulating-neutralizing reaction (autoantibodies against IgE or Fcε receptor in chronic urticaria)
No other organ shows a similar wide spectrum of different pathophysiologic mechanisms as well as clinical manifestations of allergic reactions like the skin (
Table 9-1).
In the following text, the most important allergic skin diseases will be briefly described. It has to be mentioned that all of the allergic diseases—whether they are in the skin or in the respiratory tract—can also be induced by nonimmune reactions (pseudoallergic reactions or “intrinsic” types), whereby these terms are negatively defined by the absence of detectable specific immune reactions.
Urticaria, Angioedema, Anaphylaxis
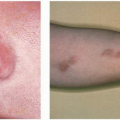
Urticaria (
Fig. 9-1) is defined as the occurrence of wheals, which generally stay for one to several hours, in rare cases up to 2 or 3 days (urticaria vasculitis). The classical example of urticaria is the histamine-induced wheal, which develops after 10 to 15 minutes of injection of histamine into the skin via prick or intradermal test and leads to a wheal and flare reaction associated with itch. The basis is an increased capillary permeability (edema), vasodilatation (redness), and an axon reflex leading to further vasodilatation (flare) (Lewis’ triad or triple response of Lewis).
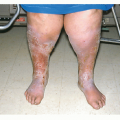
Angioedema (
Fig. 9-2) is often regarded as the subcutaneous form of urticaria with large and deep swellings, particularly in soft tissues (eyelids, lips, genital area). Urticaria and angioedema can occur in any part of the body (also on palms and soles, where patients feel pain instead of itch). Urticarial skin lesions, although itchy, are never scratched so that blood appears, but rather rubbed superficially. There are obviously different qualities of the itch sensation, which can be felt but not clearly described in our language.
Urticaria can be classified into acute (wheals occurring over a period of less than 6 weeks) and chronic (wheals appearing over a period longer than 6 weeks), which can be either intermittent or chronically relapsing with wheals appearing almost every day.
Acute urticaria is most often associated with acute infection and/or an allergic stimulus (e.g., food, drug). Chronic urticaria is also often called idiopathic when trigger factors cannot be detected. These trigger factors can be either allergens or infectious diseases of internal organs. Additives in foods can give rise to pseudoallergic type I reactions in a subgroup of chronic urticaria patients.
Autoantibodies against IgE or the high-affinity IgE receptor have been found that lead to mast cell degranulation; this phenomenon can be shown in the autologous serum test when a wheal develops after injection of a 1/10 dilution of autologous serum (Greaves’ test) (see also type VI). Another subgroup of chronic urticaria when the wheals persist over several days shows leukocytoclastic vasculitis in the dermatohistopathology and is called urticarial vasculitis. This disease is sometimes associated with autoimmune diseases (lupus erythematosus).
Management
Antihistamines are the drugs of choice; sedating antihistamines can be given overnight, sometimes also having a beneficial effect on underlying stress reactions with
psychosomatic involvement. During the day, the modern nonsedating histamine H1 antagonists are helpful. When urticaria recurs, an allergy workup or workup for an underlying infection may be beneficial. Psychosomatic counseling often is helpful in chronic urticaria. A subgroup of physical urticaria, where wheals are induced by mechanical stimuli (urticaria factitia, dermographism, pressure), temperature (cold or warm), or radiation (solar urticaria), is difficult to treat. Dapsone (avlosulfone) has been proven helpful in some cases.
Urticaria and angioedema may always be the first signs of anaphylaxis. Therefore, they have to be taken seriously. Patients with acute, severe urticaria should be observed at least 1 hour after the onset of therapy (best intravenous or intramuscular) of antihistamines and/or steroids to make sure that no further symptoms of anaphylaxis develop.
Thrombocytopenic Purpura
This is a classical type II reaction in the skin, where antibodies against substances (mostly drugs) on the surface of platelets lead to thrombocytopenia and noninflammatory purpura. This rather rare condition can be elicited by analgesics or hypnotics. The idiopathic form can be treated with intravenous immunoglobulin (IVIG).
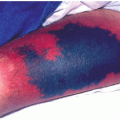
Allergic Leukocytoclastic Vasculitis
This is the prototype of a type III allergic reaction in the skin, where immune complexes lead to attraction of neutrophils with activation of proteases and mast cells, leading to destruction of vessels and vessel walls. Most often, infectious (hepatitis) or neoplastic diseases are elicitors; however, food allergens and drugs can also induce allergic leukocytoclastic vasculitis (
Fig. 9-3). In the course of serum sickness (the allergic condition inspiring Clemens von Pirquet to create the term “allergy” over 100 years ago), urticaria goes along with fever and lymph node swelling in an acute type III reaction.
Allergic Contact Dermatitis
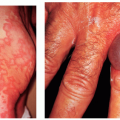
Allergic contact dermatitis (ACD) (
Fig. 9-4) is the most common occupational disease in many countries of the Western world. The dermatopathology of ACD shows acanthosis, parakeratosis, spongiosis (intercellular edema in the epidermis with intact desmosomes looking like a sponge), and lymphocytic infiltrations in the upper dermis. The terms “dermatitis” and “eczema” are used interchangeably in the dermatologic literature and are defined as:
“Non-contagious epidermo-dermitis with characteristic clinical (synchronous or metachronous polymorphology) and dermato-pathological characteristics (acanthosis, parakeratosis, spongiosis) occurring mostly on the basis of hypersensitivity.”
There are several types of eczema/dermatitis diseases (
Table 9-2).
Seborrheic dermatitis may represent a hyperergic reaction to skin microflora (Malassezia species) and show a little spongiosis.
ACD develops against small chemicals (haptens) taken up by epidermal dendritic cells (Langerhans cells) and then presented to lymphocytes that polarize into Th1 cells, leading to the inflammation in the skin. Dendritic cells attract these cells when carrying the cutaneous lymphocyte antigen (CLA). Major cytokines produced by these lymphocytes are interleukin-2, tumor necrosis factor alpha (TNF-α), and interferon gamma (IFN-γ), giving rise to keratinocyte apoptosis and spongiosis.
The most common contact allergens are tested in standard series, constantly updated by international or regional contact dermatitis research groups (ICDRG, American CDRG, European CDRG, etc.). A current standard is shown in
Table 9-3.