and Frank Hölzle2
(1)
Department of Oral and Maxillofacial Surgery, Klinikum rechts der Isar, Technische Universität Munich, Munich, Germany
(2)
Department of Oral and Maxillofacial Surgery, University Hospital of RWTH Aachen University, Aachen, Germany
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-53670-5_10) contains supplementary material, which is available to authorized users.
10.1 Development and Indications
The possibility to transfer bone blocks of the ileum as parts of composite flaps from the groin donor site was described in anatomical studies by Taylor and Watson in 1978 [540]. These authors used this flap pedicled on the superficial circumflex iliac artery (SCIA) for reconstruction of compound defects of the lower leg. Whereas the blood supply of the SCIA was excellent to the skin, the bone blocks of the iliac crest were only perfused marginally by these vessels. Other vascular pedicles around the hip, such as the ascending branch of the circumflex femoral artery or the superior gluteal artery, were also used for microvascular transfer of composite flaps containing bone from the iliac crest [29, 235]. Although the vascular anatomy of the groin region, which was the first donor site for free flaps [15], was already investigated by Taylor and Daniel in 1973 [538], it took until 1979, when Taylor et al. [540] and Sanders and Mayou [463] described the first transfer of the iliac crest bone, using the deep circumflex iliac artery (DCIA) as the vascular pedicle. Both groups independently identified the DCIA to be the main nutrient vessel of the whole ileum. Since these first reports, the iliac crest proved to be a useful and reliable donor site, which, due to its anatomical shape, is ideally suited for the harvest of bone flaps to reconstruct defects of up to half a mandible [4, 41, 42, 113, 132, 147, 260, 261, 436, 533, 534, 562, 563]. Because of the high amount of bone available, endosseous dental implants can be inserted without problems, making the iliac crest the donor site of the first choice for functional masticatory reconstruction of the mandible and maxilla [377, 436]. Sanders and Mayou also have shown that the DCIA provides blood supply to the overlying skin of the iliac crest by myocutaneous vessels [463]; thus, a skin paddle from the groin region can additionally be included and used for extraoral or intraoral reconstruction [260, 436, 562, 563]. Other flaps, such as the anterolateral thigh flap has been additionally transferred together with the iliac crest [299] to extend the skin territory for soft tissue reconstruction, performing additional anastomoses at the descending branch of the circumflex femoral artery. Because of the bulk and the limited maneuverability of the iliac crest skin paddle. Urken and coworkers introduced the inclusion of the internal oblique muscle into the iliac osteomyocutaneous flap [559, 562, 563]. He proposed to use this flat and flexible muscle for intraoral lining instead of the voluminous skin paddle. Although it was shown by Ramasastry et al. already in 1984 [426], that the internal oblique muscle is safely perfused by the ascending branch of the DCIA, thus offering the possibility to build a vascularised myo-osseous iliac flap pedicled on the DCIA, the internal oblique muscle was only used as an isolated muscle flap until Urken’s description. Apart from the decreased bulk, covering the iliac crest with the internal oblique muscle is advantageous for prosthetic rehabilitation following the insertion of endosseous dental implants. Due to the secondary atrophy of the muscle, a tight and flat residual tissue, similar to that of the attached gingiva will develop, allowing for good hygiene and loadability around the implants. The iliac crest internal oblique flap also has proven to be useful in covering skull base defects and to reconstruct the hard palate.
10.2 Anatomy
The anatomy of the DCIA was first described by Taylor et al. in detail [540]. The artery arises directly cranial (57%) to the inguinal ligament from the external iliac artery or directly caudal to it from the femoral artery (42%), mostly opposite to the inferior epigastric artery [236]. The diameter of the artery varies between 1.5 and 3 mm [40, 410, 540]. Two comitant veins are usually found, which merge 1–2 cm before entering the external iliac vein; here, the vein has a calibre of 3–5 mm. Between the transversalis and iliacus fascia, the vascular pedicle courses towards the anterior superior iliac spine (ASIS), about 2 cm cranial to the connecting line between the tuberculum pubicum and the ASIS, representing the inguinal ligament. After having reached the anterior margin of the iliac crest approximately 2 cm inferior to the ASIS, the DCIA courses along the inner aspect of the ileum dorsally, being located into the groove formed by the iliacus and transversus muscles. In the region of the iliosacral joint, the DCIA anastomoses with the thoracolumbar artery, which has an outer diameter of 2 mm and could also serve as the vascular pedicle if the DCIA has been transected following previous surgery [84]. During its course, the DCIA is giving off several branches to the iliacus muscle, as well as periosteal and medullary perforators to the iliac crest. Moreover, the DCIA is giving off the ascending branch, which is running at the undersurface of the internal oblique muscle. During its course along the inner aspect of the ileum, a number of myocutaneous perforators arise from the DCIA, piercing all of the three muscle layers of the abdominal wall. These 3–9, fine perforators are entering the skin within an approximately 2.5 cm broad cuff of externus oblique muscle, beginning at the SIAS and reaching about 10 cm distally. This muscle cuff always has to be incorporated when elevating a skin paddle. If the bulk of the muscle cuff should be reduced, a perforator-based skin paddle can be harvested if the exact localisation of the perforating vessel to the skin has been confirmed by ultrasound preoperatively [276]. Apart from the above-mentioned periosteal and medullary branches, the bone is additionally supplied by the well-perfused cuff of the iliacus and oblique muscles, which has to be left attached to the bone during flap harvesting. According to the results of anatomical studies and clinical experience, bone flaps can include the whole iliac crest, extending from the SIAS up to the iliosacral joint [40–42, 410, 436, 463, 540, 559]. Angiographically, Taylor was able to identify a number of foramina at the iliac crest, allowing the DCIA to anastomose with branches from the inferior gluteal artery, giving the anatomical basis to include parts of the gluteus muscle into the flap [333, 406, 540]. These findings were confirmed using dye injections, which also have shown that the skin paddle supplied by the DCIA can be extended along the whole ileum, reaching close to the inferior rib arch. The most important side branch of the DCIA is the ascending branch, which mostly arises from the vascular pedicle (80%) before it reaches the ASIS [559]. In the remaining cases, multiple smaller branches can be found, which reach the undersurface of the internal oblique distolaterally to the ASIS. Another branching pattern was described by Taylor, who found the ascending branch to spring off in each one third of the cases from the proximal, intermediate and distal segment of the vascular pedicle between the iliac artery and the ASIS [540]. This branch, measuring 1–2 mm in diameter, provides the dominant blood supply to the internal oblique muscle, but it does not contribute to skin perfusion. This branch allows for integration of nearly the whole internal oblique muscle, which can be used for intraoral lining [132, 559, 562, 563]. Another side branch regularly can be found just proximal to the ASIS to reach the iliacus muscle. The lateral femoral cutaneous nerve, which mostly crosses the DCIA superficially, provides sensation to the lateral and proximal aspect of the thigh. Although this cutaneous nerve can be identified medial to the ASIS and preserved by meticulous dissection, it normally is sacrificed during dissection of the pedicle because numbness at the thigh is not negatively registered by the patients. The vascular pedicle was never found to be absent [559], and besides the above-mentioned variations concerning the ascending branch, only the veins join in a variable distance from the external iliac vein, sometimes making two separate anastomoses necessary. Moreover, in rare cases, the DCIA can be doublicated [477, 559] so that the decision of which of the both arteries provide reliable blood supply to the flap has to be made by temporary clamping. Because of its variable exit and strong calibre, the ascending branch can be mistaken for the DCIA, especially in those seldom cases when the DCIA passes through the transversus muscle medially to the ASIS so that it travels more superficially along the iliac crest [540].
10.3 Advantages and Disadvantages
Because of its extensive amount of bone and the various possibilities to design the bone flap, the iliac crest is supposed to be the ideal donor site for mandible reconstruction; moreover, the flap has the potential to be used for other osseous defects at the maxilla, skull base, tibia, metacarpus and many other parts of the skeleton [132, 376, 406, 436, 477, 533, 534, 559]. Computer-assisted planning of the flap configuration can help to increase the accuracy of the bony reconstruction in the facial skeleton [27, 375, 376]. To restore masticatory function, augmentations to the severely atrophied mandible have been performed using this flap, which allows for insertion of dental implants without difficulties [436]. The anatomy of the vascular pedicle is without significant variations, and the donor site morbidity normally is low, even if extensive bone flaps have been removed including the ASIS. To prevent complications at the donor site, closure has to be performed by an experienced surgeon. After accurate hemostasis, the iliacus muscle is attached to the transversus muscle using multiple and deep sutures, which additionally can be placed through drill holes along the cut margin of the pelvic bone. Next, the internus and externus oblique muscles are approximated to the tensor and gluteus muscles. Finally, the subcutaneous fatty tissue and the skin are closed in layers. The patient is immobilised for 3–4 days, and ambulation is begun under physiotherapeutic assistance. Nevertheless, a number of complications at the donor site are known, such as herniation (9.7%), long-lasting pain (8.4%), neuropathy (4.8%), and impotence (1.2%) [152]. Moreover, injury to the iliohypogastric and ilioinguinal nerves is possible, which penetrate the muscles of the abdominal wall [333].
The length of the vascular pedicle is limited to about 7 cm, sometimes making anastomosis difficult, especially after radical neck dissection. In these cases, vein interponates have to be used to lengthen the pedicle [261, 406]. Due to the voluminous skin paddle, osteomyocutaneous iliac crest flaps often are too bulky for intraoral reconstruction [406, 559]. Moreover, reliability of the skin paddle can easily be reduced by kinking, stretching or compression of the fine myocutaneous perforators. Thus, the skin island has to be handled without any tensile or compressive forces, and it must always be designed large enough to capture a high number of myocutaneous vessels, making skin perfusion reliable. Despite this, venous drainage of the skin can be insufficient in up to 20%, if only the deep vascular system is used [260, 261, 406]. Because of this, these and other authors emphasise to additionally perform a second venous anastomosis to the superficial venous system (SCIV), which is always included in a large skin paddle [260, 406, 463].
10.4 Patient Positioning
The patient is placed in supine position with the buttocks on the donor site elevated by a beanbag. The operating field is prepped between the midline, posterior axillary line, lower rib arch and upper thigh. For mandible reconstruction, the ipsilateral hip is selected if the defect involves the ramus and angle and extends to the anterior arch and if the recipient vessels arise in the region of the angle. If a skin paddle is needed for intraoral lining, the opposite hip is selected; if the skin paddle is to be placed extraorally, the flap is raised from the ipsilateral side. Because of the constant anatomy, no preoperative measures are necessary to reveal the course of the flap vessels.
10.5 Flap Design
Bone segments of up to 6–8 × 16–18 cm can be harvested from the whole iliac crest, keeping a safe distance to the acetabulum and iliosacral joint. For mandibular reconstruction, the ASIS is used to build the angle, extending the bone flap along the iliac crest to form the body and anterior arch. The anterior border of the pelvis between the ASIS and the inferior spine is used to form the ramus of the new hemimandible. Even if the angle is not involved, inclusion of the ASIS will facilitate flap raising and does not negatively affect the appearance or morbidity of the donor site. Elliptic skin islands are outlined along the curvature of the iliac crest with the axis running in a distance of 2.5 cm parallel and medial to the iliac crest. Skin islands must always be large enough to include all perforators in a zone between the ASIS and approximately 10 cm posterior to the ASIS.
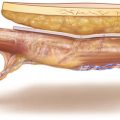
For raising of a myo-osseous flap without a skin paddle, the incision is outlined 2 cm superior to the connection of the pubic tubercule and the ASIS, starting just lateral to the pulse of the femoral artery. For further exposure of the pelvic bone, the incision is drawn directly above the curvature of the iliac crest far enough distally to allow for easy detachment of the soft tissues (◘ Figs. 10.1 and 10.2).
Skin Incision, Exposure of Inguinal Ligament
First, skin and subcutaneous fatty tissue are incised between the femoral artery and the ASIS, and the inguinal ligament is identified. The superficial epigastric vessels may run across the incision line and are ligated and divided (◘ Fig. 10.3).
Identification of Internal Oblique Muscle
The inguinal ligament which forms the aponeurosis of the external iliac muscle is incised parallel to the orientation of the ligament fibres, and the internal oblique muscle readily becomes visible. The orientation of this muscle is perpendicular to the fibres of the inguinal ligament. For the next step, skin and ligament are retracted in a cranial direction (◘ Fig. 10.4).
Exposure of Vascular Pedicle
The internal oblique muscle is transected with a scissor 2 cm superior to the connection of the ASIS and the pubic tubercule, and loose fatty tissue becomes visible, covering the thin transversalis fascia. The pulse of the DCIA is easily palpated in the groove formed by the transversus and iliacus muscle, and the vascular pedicle is exposed by careful and mostly blunt separation of the fatty tissue. It is not necessary to expose the external iliac artery for identification of the DCIA (◘ Figs. 10.5 and 10.6).
Dissection of DCIA Towards the Anterior Superior Iliac Spine (ASIS)
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


