Abstract
Systemic disease can bring about many changes in patients’ hair. Such changes include hair loss by various mechanisms, changes in hair texture, and excess hair growth. This chapter outlines common hair changes and their association with systemic disease.
Keywords
Alopecia, Hair, Hirsutism, Hypertrichosis, Telogen effluvium
- •
Hair loss in the setting of systemic disease may occur through one of five mechanisms: telogen effluvium, anagen arrest, hair miniaturization, scarring alopecia, and hair shaft disorders.
- •
The most common cause of hair loss is telogen effluvium, which can be divided into five subtypes depending on which portion of the hair cycle is pathologically lengthened or shortened.
- •
Anagen arrest occurs when there is a sudden halt in mitotic activity of the hair matrix cells.
- •
Hair miniaturization is caused by a complex interplay of genetic and hormonal influences.
- •
Scarring alopecia results in permanent injury to hair follicles and may be primary or secondary in origin.
- •
Trichorrhexis nodosa is the most common hair shaft abnormality.
- •
Systemic disease may cause excess hair in the form of hirsutism or hypertrichosis.
Hair disorders are commonly associated with systemic disease although they may be overlooked by clinicians and dismissed as unimportant, particularly in comparison with the patient’s underlying systemic illness. This is an unfortunate reality since hair can be perceived as a critical indicator of health, prosperity, and even social status. One retrospective review on the psychologic impact of alopecia on patients (regardless of cause) indicated that such patients are more likely to suffer from psychiatric illness, low self-esteem, and poor quality of life. Likewise, Americans have been estimated to spend over $2 billion annually on the removal of unwanted hair. In diagnosing and treating diseases that are associated with hair disorders, it is imperative that clinicians are mindful of the unique needs and sensitivities inherent to this group of patients.
Follicular Biology
In order to understand the behavior of the hair follicle in the setting of systemic disease, it is first important to appreciate normal follicular biology. At the time of birth, there are approximately 150,000 hair follicles on the scalp. Each undergoes a continuous cyclic pattern of changes (the follicular lifecycle) during the person’s lifetime. The first two cycles of hair growth occur synchronously in utero and then shortly after birth. After that, each follicle seems to have a growth cycle independent of those around it.
The duration of hair growth cycles is dependent on varying factors, including location of the hair, the individual’s age, nutritional habits, hormonal factors, and health status.
In healthy individuals, scalp hair grows approximately 0.35 mm/day (1 cm per month). It should be noted, however, that data suggest that African textured hair grows more slowly, at approximately 0.77 cm per month. Growth rates are also influenced by the type and anatomic location of hairs. Vellus hairs are widely distributed throughout the body, rooted in the upper dermis. They are nonpigmented, lacking melanin and a medulla, and are finely textured, measuring 0.03 mm or less in diameter and less than 1 cm in length. Growth rates for vellus hairs range from 0.03 to 0.13 mm/day. Hormonal influences at puberty induce vellus hairs to be replaced by terminal hairs in hormone-sensitive areas such as the axillae and pubis. Terminal hairs are medullated and contain melanin and thus are pigmented. They are anchored more deeply in the dermis.
Each hair follicle passes through three cycles: anagen (growth), catagen (involution), and telogen (rest) ( Fig. 43-1 ). A latency or exogen phase is noted in up to 80% of hair cycles. In exogen, the hair shaft is shed without regrowth, and a new anagen phase is turned on. Hair length is determined by the rate and duration of the anagen phase, which is terminated by an internal biologic “clock” built into every follicle. On average, anagen duration on the scalp varies from 2 to 6 years. The catagen phase marks the termination of the growing phase.
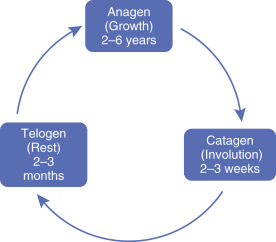
Catagen, a transitional phase of acute follicular regression, is irreversible and of relatively short duration, lasting only 2 to 3 weeks. The completion of catagen is marked by formation of the keratinized and depigmented club hair. Only 1% to 2% of scalp hairs are in catagen at any one time.
Telogen, the resting phase, begins when catagen is complete. With an average duration of 3 months, approximately 15% of scalp hairs are in telogen at any given time. Telogen hairs account for the 50 to 100 scalp hairs shed normally each day. The percentage of hairs in the telogen phase, called the telogen count, varies between individuals and even between parts of the scalp. The telogen hair (club hair) is shed during the exogen phase, which may or may not coincide with the new anagen phase. The next anagen phase begins anew from the reservoir of follicular stem cells residing in the bulge area, near where the arrector pili muscle inserts into the hair follicle. These stem cells proliferate rapidly downwards to form a new anagen hair.
Alopecia
Alopecia has traditionally been subdivided into three main categories: scarring (cicatricial), nonscarring (noncicatricial), and hair shaft disorders. In addition, Solomon proposed the term “biphasic alopecia” to describe forms of alopecia that are nonscarring early in their course, yet result in scarring later in their course. Examples of biphasic alopecia include patterned hair loss and traction alopecia. Another proposed classification scheme divides hair loss into permanent and nonpermanent alopecia. For the purposes of our discussion, we will continue to use the terms scarring and nonscarring, as they are widely accepted and firmly entrenched in the literature.
Hair loss in the setting of systemic disease may occur through one of five mechanisms ( Table 43-1 ): telogen effluvium, anagen arrest, and hair miniaturization (all forms of nonscarring alopecia); scarring alopecia; and hair shaft disorders. An important concept in the evaluation and diagnosis of hair disorders is that more than one mechanism may be operating at a given time. This can amplify the degree of hair loss, modify its pattern, and complicate the clinical picture.
| Telogen effluvium |
| Anagen arrest |
| Androgenetic alopecia/hair miniaturization |
| Scarring alopecia (cicatricial alopecia) |
| Hair shaft disorders |
Telogen Effluvium
The most common cause of hair loss associated with systemic disease is telogen effluvium (TE). This form of nonscarring alopecia manifests with diffuse, nonscarring hair shedding, often with an abrupt onset. The shedding is a result of disruption of the normal hair cycle such that a large number of hairs synchronize their growth cycles reaching a catagen and subsequent telogen phase around the same time. This can be triggered by a metabolic or hormonal stress or by drugs (severe illness, infections, medications, surgical procedures or anesthesia, and endocrinopathies). About 3 to 4 months (the time it takes for a hair to move through catagen and the early stages of telogen), after a precipitating event, normal-appearing club hairs begin to fall out in large numbers. Often the patient may recall one of the precipitating events listed in Table 43-2 .
| Injury or physiologic stress |
| Postfebrile state (extremely high fevers, e.g., malaria) |
| Severe infection, including HIV |
| Severe chronic illness |
| Following a general surgical procedure |
| Hypothyroidism and other endocrinopathies |
| Extreme dieting and/or weight loss |
| Drugs |
| Heavy metals |
| Physiologic effluvium of the newborn |
| Postpartum state |
| Early stages of androgenetic alopecia |
According to Headington, telogen effluvium can be further divided into five subtypes, depending on which portion of the hair cycle is pathologically lengthened or shortened. These subtypes are immediate anagen release, delayed anagen release, short anagen, immediate telogen release, and delayed telogen release. There is much overlap between the types, and it is often impossible to distinguish one from another in the clinical setting.
Immediate Anagen Release
Immediate anagen release accounts for most cases of telogen effluvium. Most drugs and physiologic stressors including febrile illness trigger hair loss by this mechanism. As the name suggests, the anagen phase is cut short, and hairs prematurely enter the telogen phase. Immediate anagen release has a rapid onset, usually about 3 to 5 weeks after the inciting event.
Delayed Anagen Release
Delayed anagen release occurs when hairs are retained in the anagen phase longer than usual and then move on to the catagen and telogen phase around the same time. A classic example of delayed anagen release is postpartum telogen effluvium. Metabolic and endocrine changes during pregnancy prolong the anagen phase. Upon normalization of these factors after delivery, hairs enter telogen, and new mothers experience heavy hair shedding. This also accounts for the loss of lanugo hairs in a newborn, which occurs in a synchronous molt shortly after birth. This neonatal shedding is sometimes referred to as a physiologic effluvium.
Short Anagen
Idiopathic shortening of the anagen cycle may result in a mild but persistent increased shedding. Because the duration of anagen is a major factor in determining hair length, short anagen precludes growth of long hair. Some believe that this is the mechanism underlying chronic telogen effluvium. Notably, shedding is typically not noticed until the duration of anagen is reduced by 50%.
Immediate Telogen Release
Immediate telogen release results from a shortening of the normal telogen cycle. There is good evidence that drugs such as minoxidil exert their effect via immediate telogen release, with affected follicles promptly stimulated to enter anagen. Telogen release typically begins within days of the insult, which accounts for the increased shedding some patients experience in the first days and weeks of minoxidil use.
Delayed Telogen Release
Delayed telogen release is far more common in the animal kingdom than in humans. It is by this mechanism that some animals shed their winter fur when spring arrives. Hair is shed synchronously as large numbers of telogen hairs are released, giving way to a new anagen cycle. Although the exact mechanism is not clear, this process is thought to be driven by a neuro-optic signal. Delayed telogen release may also account for the seasonal shedding that some humans experience.
Telogen Effluvium and Drugs
Medications usually cause telogen effluvium in the form of immediate anagen release. Some of the more commonly associated drugs are listed in Table 43-3 . While these medications span a wide range of drug classes, cardiovascular medications are heavily represented (anticoagulants, beta blockers, angiotensin-converting enzyme inhibitors). A few (i.e., captopril, quinacrine, nadolol, sulfasalazine) have been associated with a histologically inflammatory telogen effluvium. In the last 10 years, a number of new, biologically targeted, chemotherapeutic agents have become available. Among these new agents are sunitinib, a multitargeted tyrosine kinase inhibitor, associated with alopecia in 6% of patients. Interestingly, sunitinib reportedly causes hair color change in approximately 10% of patients. While the mechanism of alopecia in patients taking sunitinib is not clear, telogen effluvium has been histologically confirmed in a patient taking a similar medication, nolotinib. Similarly, selumetinib, a MEK1 and MEK2 inhibitor, causes alopecia in 9% of patients.
| Retinoids (etretinate, isotretinoin) |
| Anticoagulants (coumadin, heparin) |
| Antithyroid (propylthiouracil, methimazole) |
| Anticonvulsants (phenytoin, valproic acid, carbamazepine) |
| Heavy metals |
| β-Adrenergic blockers |
| Amphetamine |
| Bromocriptine |
| Captopril |
| Enalapril |
| Danazol |
| Levodopa |
| Lithium |
| Pyridostigmine |
Telogen Effluvium and Androgenetic Alopecia
Telogen effluvium and androgenetic alopecia are both relatively common diagnoses. When the two conditions coexist, patients experience a pattern hair loss that progresses more quickly than the usual course. Early-onset androgenetic alopecia is often accompanied by a brisk and episodic telogen effluvium. Androgenetic telogen effluvium is related to shortened cycle times as large scalp terminal hairs are miniaturized and shortened secondary to decreased matrix volume and reduced duration of anagen, respectively. Hair shedding is obvious only when large terminal hairs are being shed. With ensuing hair cycles, the involved follicles produce progressively miniaturized (vellus) hairs, whose loss is inapparent.
Chronic Telogen Effluvium
The usual course of telogen effluvium is self-limited. Chronic telogen effluvium occurs when the duration of hair shedding exceeds 6 months. Most common in middle-aged women, this is a diffuse, chronic, fluctuating form of hair loss that affects the entire scalp. Sometimes confused with androgenetic alopecia, chronic telogen effluvium may cause diffuse thinning and bitemporal recession, but severe and obvious balding is rare. Notably, chronic telogen effluvium is a diagnosis of exclusion rather than being linked to an identifiable underlying etiology.
Diagnosis and Treatment
The distinctive history of abrupt onset, diffuse hair shedding and an identifiable inciting event make telogen effluvium a straightforward clinical diagnosis. Despite this, androgenetic alopecia and diffuse alopecia areata should be considered in the differential diagnosis. Patients with telogen effluvium often describe loss of the most hair when showering in addition to finding hairs on clothing, on the bathroom floor, and in their vehicles. Such heavy loss sometimes prompts patients to collect their lost hairs and bring them to an office visit. A patient who presents with a large bag of shed hair is very likely to have telogen effluvium as their diagnosis. Reduced hair volume is typically apparent to the patient after the loss of about 20% of the hair. However, normal hair density may be reduced by up to 50% before thinning is apparent to clinicians. If alopecia is clinically obvious, the loss appears diffuse ( Fig. 43-2 ). In the typical patient with telogen effluvium, the telogen count seldom exceeds 50%. However, in some documented cases, telogen counts can reach up to 80%. Patients with more than 80% telogen hair counts probably do not represent a simple case of telogen effluvium. A detailed medical, dietary, and drug history is essential in establishing a diagnosis of telogen effluvium.

Physical examination of any patient with hair loss should begin with an overall inspection of the patient’s hair density. The scalp of a patient with telogen effluvium should appear within normal limits, without erythema or scale (unless there is a secondary diagnosis). A hair pull test, in which 25 to 50 hairs are pulled with firm and consistent traction from root to tip, should be done in four quadrants. Patients with telogen effluvium will have a positive result, i.e., more than three hair shafts, the roots of which show the depigmented, keratinized, clubbed morphology of telogen hairs ( Fig. 43-3 ). The patient should not have shampooed for at least one day prior to the hair pull test. A forcible hair pluck extracts a mixture of normal anagen and telogen hairs and an occasional catagen hair. The percentage of telogen hairs is increased, a criterion without which the diagnosis of telogen effluvium cannot be established with certainty ( Fig. 43-4 ). On biopsy, a 4-mm scalp punch specimen should contain 25 to 50 terminal follicles. When more than 12% to 15% of hairs are in telogen, a diagnosis of telogen effluvium is likely.