Growing Rods for Early-Onset Spinal Deformity
Grant D. Hogue
Indications
Evaluated on a case-by-case basis
Patients with a rib-vertebral angle difference >20° and Cobb angle >20° should be considered high risk for progression of their curve
Children with significant growth remaining and
Curves with a Cobb angle >50°
Curves causing significant comorbidity to other body systems
Recommend magnetic resonance imaging (MRI) for curves that progress, have Cobb angle >20°, and/or have examination with absent abdominal reflexes or other concerning neurologic findings
Alternative treatments
Observation for curves <20° or curves that do not progress
Serial casting or bracing for progressive curves >20° and optimally younger than 2 years
Sterile Instruments/Equipment Table
Radiolucent table with supports as needed or spine frame table if patient is of sufficient size
Standard instrumentation for posterior spinal fusion
Advanced imaging of choice (fluoroscopy, navigation, robotics)
Manufacturer-specific instrumentation based on surgeon’s choice of traditional growing rod (TGR) or magnetically controlled growing rod (MCGR)
Patient Positioning
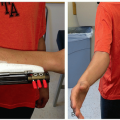
Patient positioning (Figure 8.1) will vary largely based on patient size and curve magnitude
Prone position with appropriate pads and gel rolls for support on a radiolucent flat top
Check that all rolls and padding devices are radiolucent
Prone on frame with head holder and pads
In patients with contractures, special accommodations must be made at the time of positioning
Surgical Planning
Anchor points: Rib, spine, and pelvis
Points of fixation are determined by the type of curve (idiopathic, neuromuscular, neurogenic), curve parameters (apex, end vertebrae, etc.), and local bone size/quality
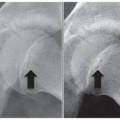
Occasionally shorter constructs (Figure 8.2) can be employed, but T2-L3 is typically a safe and predictable construct for most neurotypical patients
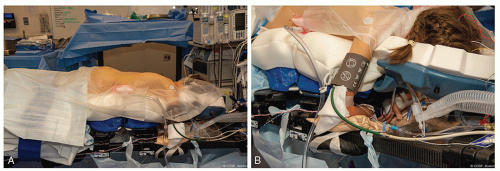
Figure 8-1 ▪ A, Patient positioned prone on Jackson style table with appropriately sized pads. B, Flexion contracture at the elbows require patient-specific positioning with supports/padding as appropriate. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
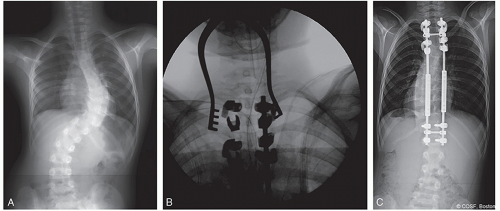
Figure 8-2 ▪ A, Preoperative posteroanterior (PA) image of ambulatory patient with early-onset scoliosis. B, Intraoperative fluoroscopic image of proximal hooks in a claw construct. C, Postoperative PA radiograph showing a “selective” construct in traditional growing rod (TGR) with inline connectors. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
With the current availability of pedicle screw sizes, many patients can be treated safely with all screw constructs, but secondary to pedicle size or bone quality, there are often times when hooks are the better choice
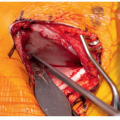
When using hooks exclusively at an anchor site, it is recommended to add a cross-link for augmentation of stability and a claw configuration (Figure 8.3)
Even in very small children, pedicle screws can generally be used in the lumbar spine
In cases of poor bone quality or perceived diminished implant strength, short rods can be added into the proximal construct to increase local stability or even to allow for fusion with staged insertion of the growing construct at a later date (see Figures 8.3 and 8.4)
Longer constructs should be considered in neuromuscular scoliosis patients with probable need for pelvic fixation
Three-segment proximal fixation has led to fewer anchor pullout complications in our practice
Surgical Approach
Standard midline posterior approach to the spine with subperiosteal dissection at the levels to be instrumented.
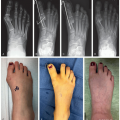
Can be either done with a single long incision or smaller incisions directly over the anchor levels and the rod connector(s) (Figure 8.4)
It is important to note that even if using 1 long incision, the only deep dissection is at the anchor levels
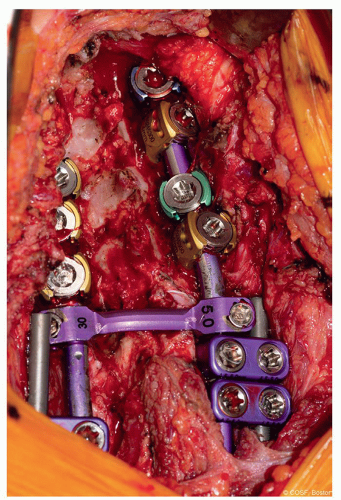 Figure 8-3 ▪ Intraoperative photograph of proximal hooks in a claw configuration with a cross-link for added stability. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
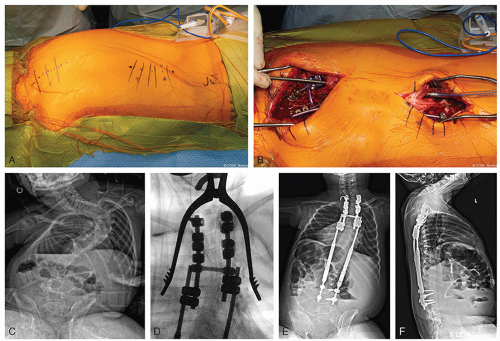 Figure 8-4 ▪ A, Intraoperative photograph of 2-incision technique for placement of growing instrumentation with planned subfascial tunneling. B, Passage of rod in the subfascial space with the assistance of a chest tube. C, Preoperative posteroanterior (PA) radiograph of a patient with scoliosis secondary to spinal cord injury. D, Intraoperative fluoroscopic image of a double-claw hook construct over 3 segments. E, Postoperative PA radiograph after insertion of magnetically controlled growing rod (MCGR). F, Postoperative lateral radiograph after insertion of MCGR. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Related posts: Occiput and Posterior Cervical Instrumentation Occiput and Posterior Cervical Instrumentation
 Decision-Making in Pediatric and Adolescent Hip Disorders Decision-Making in Pediatric and Adolescent Hip Disorders
 Clubfoot Casting and Heel Cord Lengthening Clubfoot Casting and Heel Cord Lengthening
 Radioulnar Synostosis Derotation Osteotomy Radioulnar Synostosis Derotation Osteotomy
 Neuromuscular Hip Surgery: Prevention to Reconstruction Neuromuscular Hip Surgery: Prevention to Reconstruction
 Minimally Invasive Techniques for Foot Deformity Correction Minimally Invasive Techniques for Foot Deformity Correction
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|