Clinical Presentation
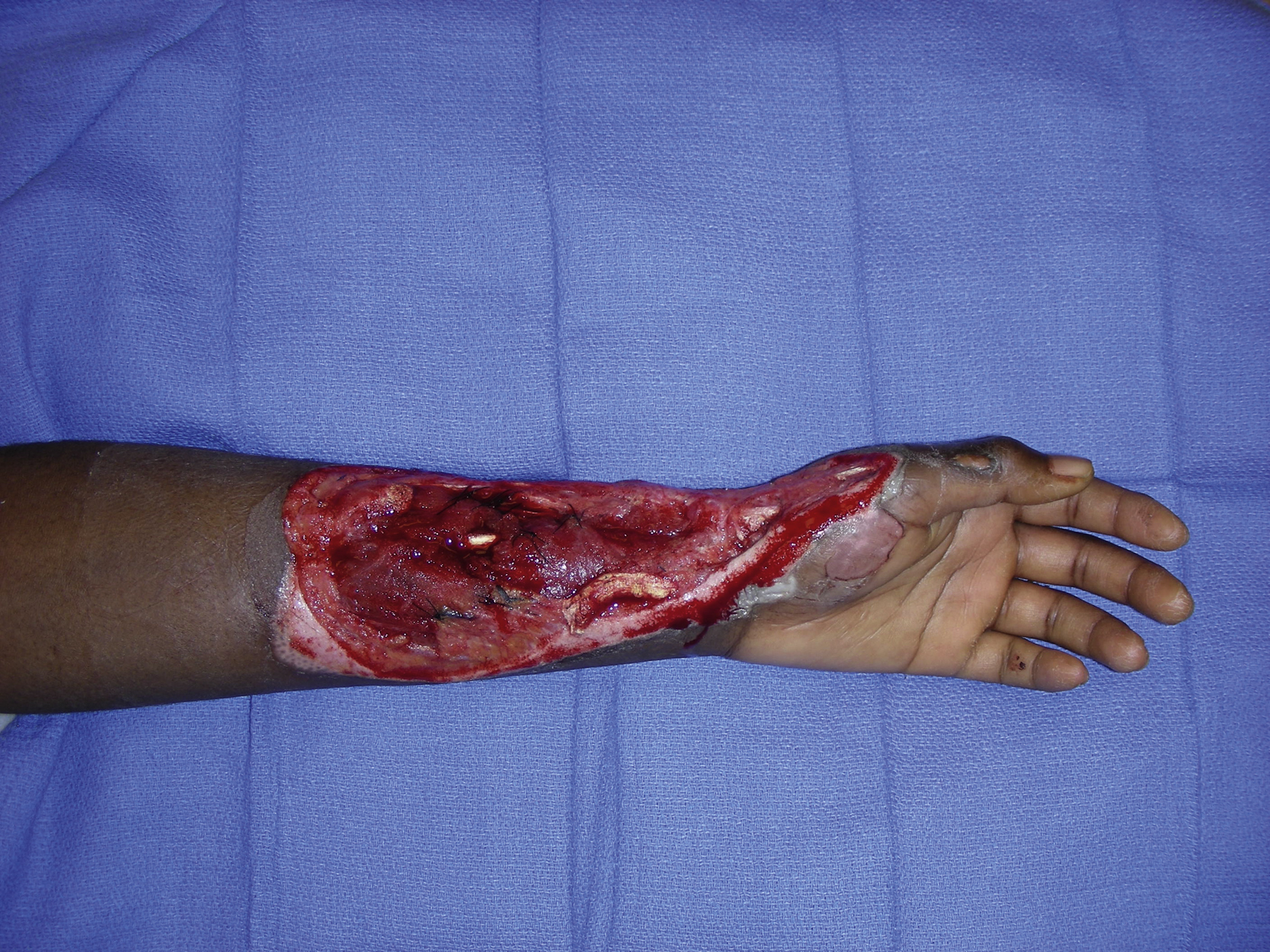
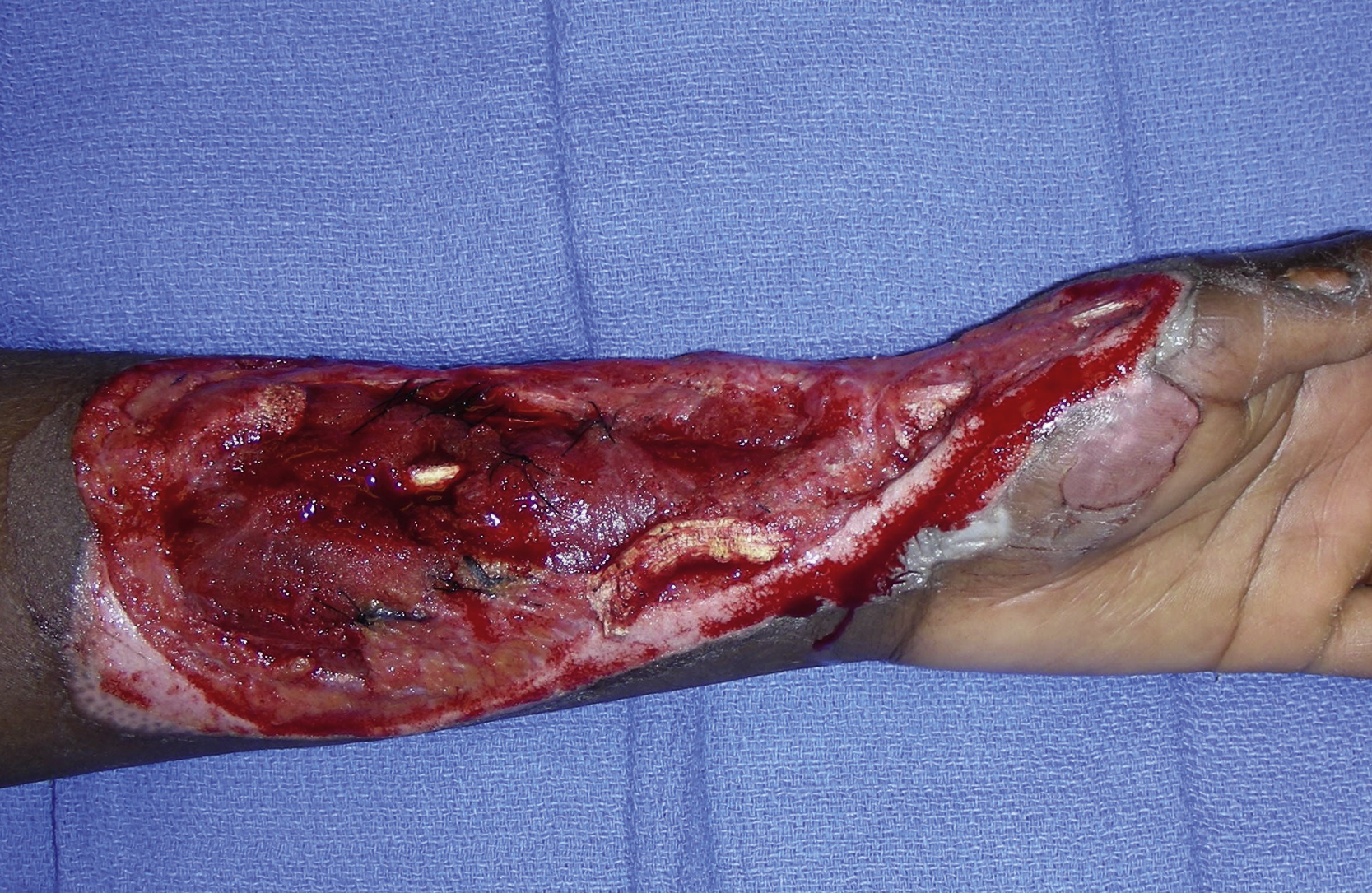
A 24-year-old Black American female sustained an avulsion injury to her left forearm wound secondary to a motor vehicle accident. She sustained a large complex soft tissue wound, measuring 18 × 8 cm, in the left volar forearm with multiple flexor digitorum superficialis muscle injuries and a transection of the median nerve with a 5-cm gap. The radial artery and its accompanied veins within the wound were also transected ( Figs. 18.1 and 18.2 ). The plastic surgery service was consulted to provide a soft tissue reconstruction for her forearm as well as the medial nerve reconstruction once she was cleared by the trauma service.
Operative Plan and Special Considerations
Based on the location and size of the soft tissue defect in the forearm as well as the nature of the reconstruction to provide a good skin coverage to the forearm, a free anterolateral thigh (ALT) perforator flap was offered to this patient for the reconstruction of such a large forearm wound. The ulnar artery system was also evaluated for its patency and adequacy to ensure an adequate blood supply to the hand. In addition, perforators in each thigh’s potential donor site were mapped by duplex scan so that a preferred site for free ALT perforator flap harvest could be chosen. The sural nerve from the left leg was prepared as a nerve graft donor site for the cable nerve grafting of the medial nerve gap.
Operative Procedures
Under general anesthesia, the procedure started by debriding the left forearm wound followed by Pulsavac irrigation. After debridement, all flexor digitorum superficialis muscles were repaired accordingly with 3-0 vicryl suture and both proximal and distal ends of the median nerve in the forearm were identified after further dissection. Both nerve ends were tagged with a 4-0 Prolene suture. The zigzag incisions were made proximally toward the antecubital fossa. The stump of the radial artery was identified and dissected further proximally toward the bifurcation of the radial artery and the ulnar artery in order to make sure the artery microvascular anastomosis would be outside the zone of injury. The vena comitans and the radial artery appeared to be very small. However, the superficial medial antecubital vein appeared to be a good size and could be used as a recipient vein for venous microvascular anastomosis.
An 18 × 8 cm skin paddle was marked within the left ALT territory. Three perforators were identified by preoperative duplex scan ( Fig. 18.3 ). With suprafascial dissection, two perforators were identified but only one appeared to be large with a strong arterial signal. Therefore, the flap could be based on this larger perforator. The fascia was incised around the perforator. After a course of septocutaneous dissection, the descending branch of the lateral circumplex femoral vessel was identified. The end of the descending branch distal to the junction of the perforator was divided and two visible motor nerves were preserved. The pedicle dissection was performed between the vastus lateralis and rectus femoris muscles toward the profunda vessels. The pedicle vessels were individually separated and divided with hemoclips and the flap dissection was completed ( Fig. 18.4 ).


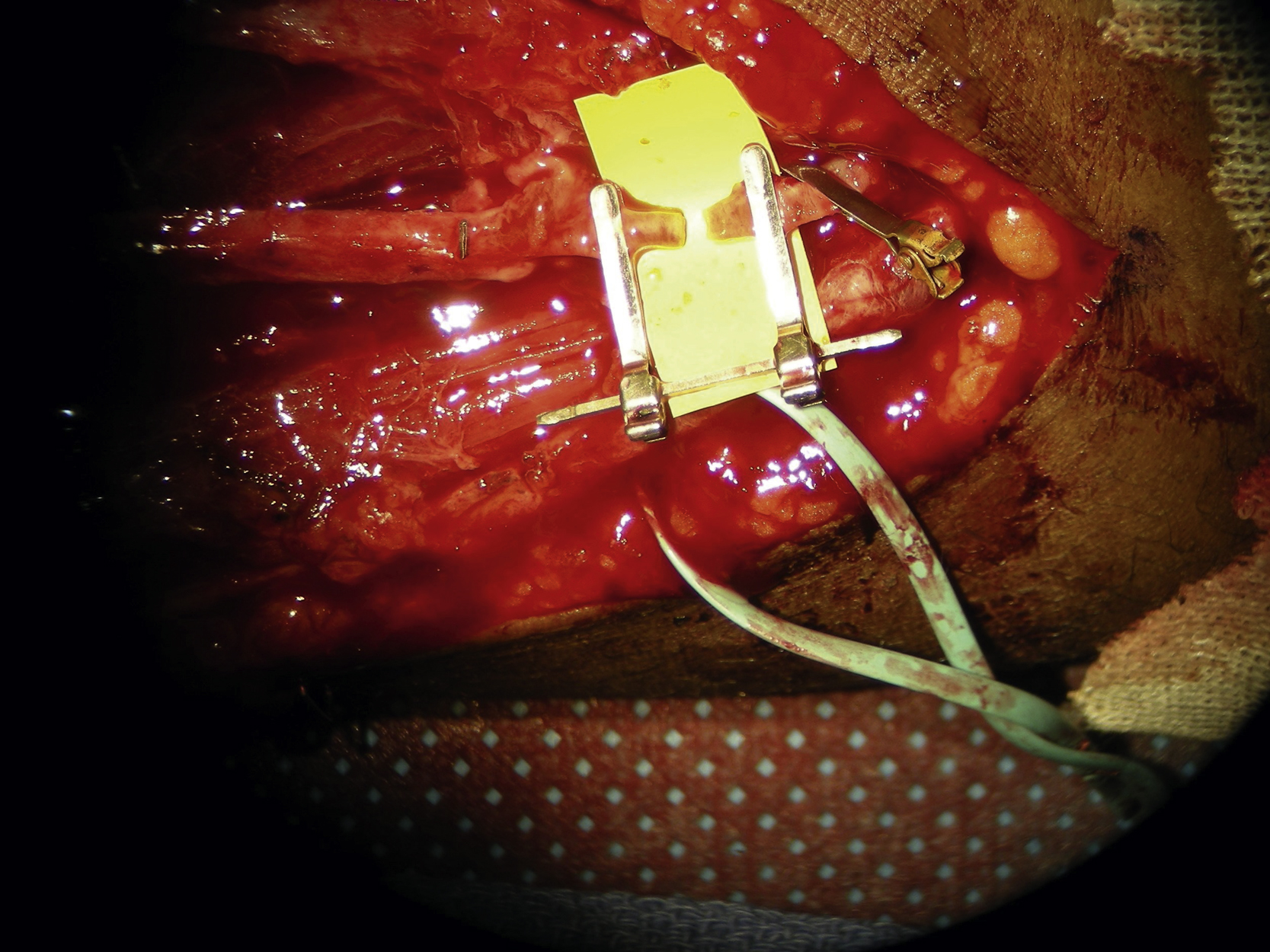
The pedicle was prepared under loop magnification. One artery and two veins were identified. The artery was flushed with heparinized saline solution. One good vein was selected for microvascular anastomosis. Both microvascular anastomoses were performed under a microscope. The arterial microanastomosis to the radial artery stump was performed in an end-to-end fashion with interrupted 8-0 nylon sutures ( Fig. 18.5 ). The venous microanastomosis to the superficial antecubital vein was also performed in an end-to-end fashion with a 2-mm coupler ( Fig. 18.6 ). Once all the clamps had been released, the flap appeared to be well perfused. The flap was temporarily inset into the forearm wound.