Eczematous eruptions are characterized as inflamed papules and plaques, often in association with pruritus and serous discharge. The specific subtype of eczematous dermatitis is based upon the clinical morphology, distribution of lesions, and in many cases the history of exposure. Biopsy of the skin in these conditions is usually not helpful except to consider alternative diagnoses with distinct histopathologic features. In children, by far the most prevalent type of eczematous eruption is atopic dermatitis (AD).
Atopic Dermatitis
AD, one of the most common skin disorders seen in infants and children, begins during the first 6 months of life in 45% of children, the first year of life in 60% of affected individuals, and before 5 years of age in at least 85% of affected individuals. Although the term eczema is commonly used, AD is a more precise term to describe this subset of dermatitis or inflammation of skin. The concept of atopy (derived from the Greek atopia , meaning different or out of place ) was originated by Coca and Cooke in 1923. Although initially only asthma and allergic rhinitis were included in this category, Wise and Sulzberger in 1933 coined the term AD, noting the association of this form of eczema with other atopic disorders.
Prevalence and Association with Other Atopic Disorders
The prevalence of AD in American children is 10% to 13%, which is consistent with the prevalence in Scandinavia and Japan and represents a marked increase during the past several decades. Studies performed before 1960 estimated the prevalence to be up to 3%. Of these, 67% have mild disease, 26% have moderate disease, and 7% have severe AD. AD severity is increased in older children, the eldest child in the family, and in children with African-American or Hispanic race/ethnicity. AD occurs more often in urban areas than in rural areas, in blacks, in smaller families, and in higher socioeconomic classes, suggesting that exposure to antigenic pollutants and lack of exposure to infectious agents or other antigenic triggers early in life may play a role in the development of the dermatitis. The subsequent steady increase has paralleled the increase seen in children with asthma, suggesting a shared mechanism or triggers. In fact, AD is often the first manifestation of the “atopic march,” with the later development of sensitization to foods and environmental allergens, asthma and allergic rhinitis. Children with AD overall have a threefold increased risk of developing asthma and a threefold increased risk of developing allergic rhinitis compared with children without AD. Greater severity, earlier onset, persistence of the AD, and parental history of allergic disease further increase the odds of developing other atopic disorders. Overall, asthma occurs in up to 50% of children who develop AD during the first 2 years of life; allergic rhinitis develops in 43% to 80% of children with AD. In addition to the higher prevalence of comorbid asthma, hay fever, and food allergies, severe AD in children is correlated with poorer overall health, impaired sleep, and increased healthcare utilization. Some have classified AD into an immunoglobulin (Ig) E-associated form (“true” or “extrinsic” AD in 70% to 80% of patients) and a non-IgE-associated form (“nonatopic” or “intrinsic” AD). Although the significance of having high IgE levels is unclear, recent biomarker studies in adults have shown that individuals with intrinsic AD show similar activation of T helper (Th) 2 cytokines, but increased Th17 cytokines in comparison with adults with extrinsic AD.
Genetic Alterations
A role for causative genetic alterations is suggested by the concordance of 77% in monozygotic twins and the greater probability of having AD if one or, even more so, both parents have AD. Loss-of-function mutations in profilaggrin ( FLG ) cause ichthyosis vulgaris, a common genetic disorder characterized by dry, scaling skin and hyperlinear palms (see Chapter 5 ) that has long been known to be associated with AD. Mutations in FLG occur in 10% to 30% of AD patients. In addition to the tight linkage of AD with genes of the epidermal differentiation complex (particularly encoding filaggrin), genome-wide association (GWA) studies have shown numerous other associated loci, primarily suggesting a role for epidermal barrier function and innate-adaptive immunity in the pathogenesis of AD.
Understanding Atopic Dermatitis Pathomechanism as a Guide to Therapy
The “inside-out” concept of AD pathogenesis focuses on immune abnormalities as being primary, whereas the “outside-in” theory considers the epidermal barrier dysfunction (a form of “innate immunity”) as primary. Nevertheless, AD results from the complex interaction between immune dysregulation, epidermal barrier dysfunction, and environmental interactions with skin. Understanding these alterations have led to new therapies for AD (see the Management section).
In the acute phase of AD, environmental triggers including irritants, allergens, microbes, and mechanical injury (scratching or rubbing) activate the skin’s innate immune system, which includes epidermal Langerhans cells, keratinocytes, and local immune cells. Expression of cytokines, particularly thymic stromal lymphopoietin (TSLP), interleukin (IL)-25 and IL-33, activate group 2 innate lymphoid cells (ILC2s), leading to Th2 cell activation. Th2 cells express IL-4, -5, and -13, which promote eosinophilia and IgE production but suppress the expression of epidermal barrier proteins as well as antimicrobial peptides such as β-defensins and cathelicidin. This reduction in antimicrobial peptide production likely contributes to the propensity toward development of skin infection in AD patients. TSLP and another Th2 cytokine, IL-31, are thought to mediate AD pruritus. Systemic circulation of keratinocyte-derived TSLP has been suggested to promote the development of allergic sensitization in both the gastrointestinal (GI) tract and the lungs.
Recent studies show that AD T cells also differentiate into Th22 cells, which produce IL-22 and thereby stimulate expression of keratinocyte S100As. IL-22 has been implicated in the thickening of skin with lichenification. The role of Th17 cells in AD is not well understood, but increased levels of IL-17 are found (although not to the extent of Th2 cytokines and IL-22), particularly in patients with intrinsic (vs. extrinsic) AD. With chronic AD, the Th2 and Th22 cytokine profiles are accentuated, and in addition, Th1 cytokines are detected (predominantly interferon-γ).
Elevation of cytokines and chemokines in lesional and nonlesional skin, as well as in blood, are biomarkers of disease activity. In adult AD skin, the levels of IL-13, IL-22, CCL17 (TARC), and S100A biomarkers have been found to correlate with disease responses to cyclosporine A and narrow-band ultraviolet light. In the blood, levels of IL-33, Th2 and Th22 cytokines/chemokines, and periostin, a Th2 cytokine-induced extracellular matrix protein, are increased in AD and correlate with disease severity.
The intact epidermis itself also plays a role in the skin’s innate immune system, because it functions as a barrier against water loss (preventing dry skin) and penetration of high molecular weight allergens such as dust mite antigens, foods, and microbes. This barrier can be altered by decreased expression of structural proteins (particularly filaggrin) and lipids (particularly ceramides) or by increased expression of proteases (especially kallikrein 5) that break down barrier proteins and increase TSLP. Filaggrin is the major component of the stratum granulosum of epidermis and binds to keratin. Its precursor, profilaggrin, contains 10 to 12 monomers of filaggrin, and fewer monomers within the profilaggrin gene (i.e., 10 vs. 12) have been linked to an increased risk of developing AD, which complements the known increased risk of developing AD with filaggrin insufficiency from null mutations in profilaggrin, as occurs in patients with ichthyosis vulgaris (see Chapter 5 ). Filaggrin is also broken down into amino acids, such as urocanic acid, that promote skin hydration, providing another explanation for the dry skin of AD and ichthyosis vulgaris. AD in association with mutations in FLG has been shown to be more severe and more persistent. Although little is known about epidermal lipids in AD, decreased content of long-chain ceramides may also contribute to the defect, and many emollients now contain ceramides in an effort to correct the ceramide deficiency. One moisturizer contains both ceramides and filaggrin breakdown products (Cetaphil Restoraderm cream).
Clinical Features
The cardinal features of AD are pruritus, chronicity, and the age-specific morphology and distribution of lesions ( Box 3-1 ). Extent of involvement may range from mild and limited, for example to flexural areas, to generalized and severe. AD has been divided into phases based on patient age and the distribution of lesions (infantile, childhood, and adult), but there is considerable overlap (e.g., infants may show the typical distribution of adult AD).
Essential Feature
Pruritus (or parental reporting of itching or rubbing) in past 12 months
Plus Must Have at least Three of the Following
History of generally dry skin in past year
Personal history of allergic rhinitis or asthma (or history in first-degree family member if child <4 years old)
Onset before 2 years of age (unless currently <4 years of age)
History of skin crease involvement (antecubital or popliteal fossae; front of ankles; neck; periorbital)
Visible flexural dermatitis (if child <4 years, include cheeks or forehead, and extensor surface of limbs)
The infantile phase of AD reflects the manifestations of AD from birth to 6 months of age. It is characterized by intense itching, erythema, papules, vesicles, oozing, and crusting. In infants, it usually begins on the cheeks, forehead, or scalp ( Figs. 3-1, 3-2, and 3-3 ) and then may extend to the trunk ( Fig. 3-4 ) or particularly the extensor aspects of the extremities in scattered, ill-defined, often symmetrical patches. Generalized xerosis is common. Exacerbation of facial dermatitis on the medial cheeks and chin is often seen concomitant with teething and initiating foods. This localization likely reflects exposure to irritating saliva and foods, although contact dermatitis or urticaria may contribute. By 8 to 10 months of age the extensor surfaces of the arms and legs often show dermatitis ( Fig. 3-5 ), perhaps because of the role of friction associated with crawling and the exposure of these sites to irritant and allergenic triggers such as those found in carpets. Although dermatitis of the antecubital and popliteal fossae, periorbital areas, and neck are more commonly involved in older children and adolescents, these sites may be affected in infants and young children as well ( Fig. 3-6 ). Typically, lesions of AD spare the groin and diaper area during infancy ( Fig. 3-7 ), which aids in the diagnosis. This sparing likely reflects the combination of increased hydration in the diaper area, protection from triggers by the diaper, and inaccessibility to scratching and rubbing. The “headlight sign” has been used to describe the typical sparing of the nose and medial cheeks in AD, even when there is extensive facial involvement elsewhere (see Figs. 3-2 and 3-3 ).







Not uncommonly, infants initially show signs of seborrheic dermatitis, particularly during the first month or two of life. The associated pruritus and the dry (rather than greasier) scale suggest the combination of both disorders (see Fig. 3-3 ); the seborrheic component usually clears by 6 to 12 months, whereas the AD features persist. Alopecia may accompany the scalp involvement because of inflammation and chronic rubbing.
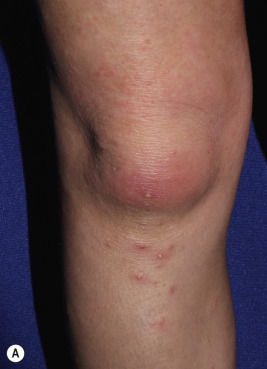
The childhood phase of AD usually occurs from 2 years of age to puberty. Affected persons in this age group are less likely to have exudative and crusted lesions and have a greater tendency toward chronicity and lichenification ( Fig. 3-8 ). Eruptions are characteristically drier and more papular and often occur as circumscribed scaly patches. The classic areas of involvement in this group are the wrists, ankles, hands, feet, neck, and antecubital and popliteal regions ( Figs. 3-9 and 3-10 ). Facial involvement switches from cheeks and chin to periorbital ( Fig. 3-11 ) and perioral, the latter sometimes manifesting as “lip-licker’s dermatitis” (see Figs. 3-33 and 3-50 ). Dermatitis of the nipples ( Fig. 3-12 ) occurs in some infants and children and can be exacerbated by rubbing on clothing. Pruritus is often severe. Some children with AD show “nummular” or coin-shaped lesions with sharply defined oval scaly plaques on the face, trunk, and extremities (see Nummular Dermatitis section). In African-American children, the lesions of AD are often more papular and follicular-based (see Fig. 3-7 ; Fig. 3-13 ). Although localization at flexural areas is more common, some children show an inverse pattern with involvement primarily of extensor areas. Lymphadenopathy may be a prominent feature in affected children ( Fig. 3-14 ), reflecting the role of lymph nodes in handling local infection and inflammation. Nail dystrophy may be seen when fingers are affected, indicating involvement of the nail matrix; children may show secondary staphylococcal or pseudomonal paronychia.







The adult phase of AD begins later in childhood and often continues into adulthood. Predominant areas of involvement include the flexural folds ( Fig. 3-15 ), the face and neck, the upper arms and back, and the dorsal aspect of the hands, feet, fingers, and toes. The eruption is characterized by dry, scaling erythematous papules and plaques and by the formation of large lichenified plaques from lesional chronicity. Weeping, crusting, and exudation may occur from the AD itself, but usually is the result of superimposed staphylococcal infection or allergic contact dermatitis (ACD). Prurigo nodularis, well-circumscribed, usually hyperpigmented thickened papules, most common on the lower extremities, is most commonly seen during adolescence ( Fig. 3-16 ).


Postinflammatory hypopigmentation may be seen at any age, especially in individuals with darker skin (see Fig. 3-15 ; Fig. 3-17 ). The pigmentary changes are transient and are reversible when the underlying inflammation is controlled; however, 6 months or more may be required for repigmentation, and sun exposure will accentuate the differences between uninvolved and hypopigmented skin areas. In contrast, hyperpigmentation is predominantly noted at sites of lichenification, because the thickened epidermis accumulates epidermal melanin pigment, especially in darker skinned individuals. Children with lichenification show accentuation of skin markings (see Fig. 3-8 ; Figs. 3-18 and 3-19 ). Parents may mistake the postinflammatory pigment change seen in some children for scarring or a toxicity of topically applied medications and need reassurance. AD lesions are not usually scarring, but secondary infection and deep gouging of lesions can leave residual scarring and permanent depigmentation (see Fig. 3-19 ).



Other Clinical Signs
Several other clinical signs are seen with increased incidence in children with AD, although they may appear in children without AD as well. Dermographism, a manifestation of the triple response of Lewis that occurs in approximately 5% of the normal population, is characterized by a red line, flare, and wheal reaction. A red line develops within 15 seconds at the exact site of stroking, followed within 15 to 45 seconds by an erythematous flare (because of an axon-reflex vasodilation of arterioles). The response finally eventuates in a wheal (because of transudation of fluid from the injured capillaries in the original stroke line) 1 to 3 minutes later. Individuals with AD often demonstrate a paradoxical blanching of the skin termed white dermographism ( Fig. 3-20 ). The initial red line is replaced, generally within 10 seconds, by a white line without an associated wheal. Patients with AD may also show circumoral pallor, thought to relate to local edema and vasoconstriction.

Follicular hyperkeratosis or chicken-skin appearance, particularly on the lateral aspects of the face, buttocks, and outer aspects of the upper arms and thighs, is termed keratosis pilaris (see Figs. 7-24 and 7-25 ). Keratosis pilaris is not seen at birth but is common from early childhood onward and often persists into adulthood. Each lesion represents a large cornified plug in the upper part of the hair follicles, often with surrounding inflammation and vasodilation. Keratosis pilaris is more commonly associated with AD in children with ichthyosis vulgaris. Moisturizers alone tend to be insufficient as therapy for keratosis pilaris, and keratolytic agents such as urea or α-hydroxy acids are required. Their use is limited, however, by the increased potential for irritation in children with AD. Treatment should be discouraged unless of significant cosmetic importance, because keratosis pilaris is almost always asymptomatic.
Lichen spinulosus manifests as round collections of numerous tiny, skin-colored to hypopigmented dry spiny papules ( Fig. 3-21 ). More common in African-American children, lichen spinulosus usually occurs on the trunk or extremities. Lesions tend to be asymptomatic and may respond to application of emollients and mild topical corticosteroids. Children with AD also show an increased incidence of pityriasis alba, nummular dermatitis, dyshidrotic eczema, and juvenile plantar dermatosis (see related sections).

Individuals with atopic disorders have a distinct tendency toward an extra line or groove of the lower eyelid, the so-called “atopic pleat” ( Fig. 3-22 ). Seen just below the lower lid of both eyes, the atopic pleat may be present at birth or shortly thereafter and is often retained throughout life. This groove (commonly referred to as a Dennie–Morgan fold ) may result from edema of the lower eyelids and skin thickening; it represents a feature of the atopic diathesis rather than a pathognomonic marker of AD. The atopic pleat has been found with increased incidence in African-American children. Slate-gray to violaceous infraorbital discolorations (“allergic shiners”), with or without swelling, are also seen in patients with allergies and in patients with AD. Allergic shiners are thought to be a manifestation of vascular stasis induced by pressure on underlying venous plexuses by edema of the nasal and paranasal cavities; the swelling and discoloration become more prominent as a result of repeated rubbing of the eyes and postinflammatory pigment darkening. Another clinical feature, an exaggerated linear nasal crease, is caused by rubbing of the nasal tip (the so-called “allergic salute”) and occurs in 7% of schoolchildren. Milia (tiny inclusion cysts; see Chapter 9 ) of the periorbital area are common in preadolescents ( Fig. 3-23 ), may resemble acne, and are thought to result from the recurrent rubbing.


Many patients with atopic conditions exhibit an increased number of fine lines and accentuated markings of the palms ( Fig. 3-24 ). These accentuated palmar markings often are a clue to the concurrent diagnosis of ichthyosis vulgaris (see the previous discussion of the pathomechanism and also Chapter 5 ), a relatively common semi-dominant genetic disorder seen with increased incidence in children with AD. Although individuals with either AD or ichthyosis vulgaris may show accentuated markings on the palms and soles, the characteristic generalized scaling with larger and more severe scaling on the lower extremities, worsening during winter months, and often positive family history of patients with ichthyosis vulgaris further helps to distinguish these conditions.

Allergic keratoconjunctivitis (AKC) is a chronic noninfectious inflammatory condition and is one of the most severe ophthalmic complications associated with atopic dermatitis. AKC has been described in up to 30% of children with AD. It typically begins during late teenage years but has been described as early as 7 years of age. Patients experience chronic itching and pain of the eyes, as well as tearing, redness, and blurred vision. It requires prompt and effective treatment to prevent permanent vision loss; moderate to severe eye irritation, increased redness, discharge, and any visual symptoms are features that require more urgent referral to an ophthalmologist. Complications of AKC include cataracts, keratoconus, infectious keratitis, blepharitis, tear dysfunction, and steroid-induced glaucoma. Treatment options include a combination of mast cell inhibitors, antihistamines, corticosteroids, and calcineurin inhibitors.
Posterior subcapsular cataracts have been described in up to 13% of adult patients with severe AD. Rarely seen in children, these cataracts are usually asymptomatic. Keratoconus (elongation and thinning of the corneal surface) has been reported in about 1% of patients with AD and seems to develop independently of cataracts. Keratoconus is exacerbated by continuous rubbing of the eyes and may require corneal transplantation.
Infectious Complications
In contrast to a prevalence of a carrier state in 5% to 20% of individuals who have no atopic condition, Staphylococcus aureus is recovered in up to 90% of patients from lesions of AD—up to 76% from uninvolved (normal) skin and 50% to 60% from the anterior nares. The increased adherence of S. aureus to the epidermal cells of individuals with AD and a failure to produce endogenous antimicrobial peptides in the inflamed skin of patients with AD may account for the high rate of S. aureus colonization and infection. Although secondary infection in AD is usually from S. aureus (72%), 16% of cultures in infected patients with AD yield S. pyogenes, and 14% are mixed cultures. Patients infected with group A streptococcus were more likely to be febrile, to have facial and periorbital involvement, have bacteremia and cellulitis, and to be hospitalized compared with those infected with S. aureus alone.
The pyoderma associated with AD is usually manifested by erythema with exudation and crusting ( Fig. 3-25 ), particularly at sites of scratching, and occasionally by small pustules at sites of dermatitis ( Fig. 3-26 ). This complication must be considered whenever a flare of chronic AD develops or fails to respond to appropriate therapy. S. aureus exacerbates the AD through: (1) release of superantigen toxins, which enhance T-cell activation; (2) activation of superantigen-specific and allergen-specific T cells ; (3) expression of IgE antistaphylococcal antibodies ; and (4) increased expression of Th2 cytokines (including IL-31 and TSLP, which are known to cause pruritus directly) and increased expression of IL-22, which is associated with epidermal thickening. Superantigen production also increases the expression of an alternative glucocorticoid receptor that does not bind to topical corticosteroids, leading to resistance. Other factors produced by S. aureus are likely to exacerbate AD as well. These observations emphasize the role of S. aureus as an important trigger of AD and endorse therapies that decrease the numbers of bacteria on the skin.


Although methicillin-resistant S. aureus (MRSA) colonization and superinfection of AD is increasing, the majority of children with AD harbor methicillin-sensitive S. aureus (MSSA). MRSA infection may manifest as pustules ( Fig. 3-27, A ), abscesses ( Fig. 3-27, B ) or crusting that is indistinguishable clinically from MSSA infection but much more difficult to eradicate; suppression of MRSA often requires that the entire family (including pets, who can harbor MRSA) be treated initially or even on an intermittent basis to reduce colonization and familiar infections, such as with intranasal mupirocin ointment and once to twice weekly bleach baths or sodium hypochlorite-containing cleansers.

Greater cutaneous dissemination of certain viral infections has also been noted in children with AD and has been attributed to defects in the generation of antimicrobial peptide and the relative deficiency of Thl cytokine generation and cytotoxic T-cell function. Molluscum contagiosum is a cutaneous viral infection of childhood that most commonly affects the trunk, axillae, antecubital, popliteal fossae, and crural areas (see Chapter 15 ). Lesions are usually small, dome-shaped papules that often show central umbilication. The often-extensive molluscum lesions tend to be most numerous at sites of active dermatitis and can induce pruritus as well as dermatitis around the molluscum papules (“molluscum dermatitis”).
Eczema herpeticum (EH, also termed Kaposi varicelliform eruption) describes the explosive development of a vesiculopustular eruption caused by herpes simplex virus in an individual with an atopic condition. Children with more severe AD and other atopic conditions are at greatest risk. Herpes simplex virus has been associated with having fewer circulating and skin-resident T cells that express interferon-γ. The clustering and often umbilication of the vesicles is characteristic ( Figs. 3-28 and 3-29 ), with sites of the dermatitis most commonly affected. The diagnosis can be verified by direct fluorescent assay and viral culture. If these tests are not available, a Tzanck test can be performed by scraping the floor of vesicles and, after staining the smear with Giemsa or Wright stain, searching for multinuclear virus “giant cells” or balloon cells.


Hospitalization may be necessary, especially in infants under 1 year of age and in association with fever and/or systemic symptoms. Early administration of acyclovir has been shown to lead to better outcomes for EH, and use of topical corticosteroids or calcineurin inhibitors has not been associated with poorer outcomes in children hospitalized with EH. Systemic antibiotics should be administered if secondary bacterial infection is strongly suspected but should not be used empirically. Eczema vaccinatum was a problem when smallpox vaccinations were compulsory, most commonly contracted by accidental contact with a recently vaccinated individual. The global threat of bioterrorism and consideration of smallpox vaccinations has again brought to attention the risk of eczema vaccinatum for patients, particularly children, with AD. Eczema vaccinatum is characterized by the widespread cutaneous dissemination of vaccinia viral lesions that manifest as firm, deep-seated vesicles or pustules that are all in the same stage of development (see Chapter 15 ). Lesions may become umbilicated or confluent. Eczema coxsackium is a recently coined term to describe the unusual cutaneous concentration in sites of previous or current AD of vesicles and erosions from Coxsackie A6 and, less commonly, Coxsackie A16 infection, which could be confused with EH. Fever, oral erosions/ulcerations, and sore throat/mouth are among the most common associated symptoms. Lesions clear spontaneously in an average of 12 days but may persist for a month. Reactivity to Malassezia has been blamed for recalcitrant AD of the head and neck in adolescents. Although there are no documented differences in Malassezia species colonization, patients with head and neck AD are more likely to have positive skin-prick test results and Malassezia -specific IgE compared with healthy control subjects and patients with atopy without head and neck dermatitis. These patients may benefit from a 1- to 2-month course of daily itraconazole or fluconazole followed by long-term weekly treatment.
Differential Diagnosis
AD is a chronic fluctuating disease. The distribution and morphology of lesions vary with age, but itching is the cardinal symptom of this disorder. Although many skin conditions may occasionally resemble AD, certain characteristics assist in their differentiation.
Seborrheic dermatitis is characterized by a greasy yellow or salmon-colored scaly eruption that may involve the scalp, cheeks, trunk, extremities, and diaper area. The major differentiating features include a tendency toward earlier onset, characteristic greasy yellowish or salmon-colored lesions with a predisposition for intertriginous areas, a generally well-circumscribed eruption, and a relative absence of pruritus (see below). Infants may show both atopic and seborrheic dermatitis (see Fig. 3-2 ), with progression or persistence of the atopic lesions as the seborrheic dermatitis subsides.
Contact dermatitis can be divided into irritant contact dermatitis and ACD. Primary irritant dermatitis is commonly seen in infants and young children. It is most commonly seen on the cheeks and the chin (owing in part to the irritation of saliva), the extensor surfaces of the extremities (as a result of harsh soaps, detergents, or rough fabrics), and the diaper area (primarily from feces and vigorous cleansing). Primary irritant dermatitis is generally milder, less pruritic to asymptomatic, and not as eczematous and oozing as the eruptions seen in association with AD. Irritant dermatitis may also result from bubble baths, personal care products, and in handled materials such as modeling clays. Irritant contact dermatitis to saliva and to exposure to harsh soaps and fabrics occurs more often in children with concomitant AD. Although the diaper area in AD is typically normal, irritant diaper dermatitis can occur.
ACD, although relatively uncommon in the first few months of life, can mimic almost any type of eczematous eruption and is characterized by a well-circumscribed pruritic, erythematous, papular, and vesicular eruption. Although such eruptions involute spontaneously on identification and removal of the cause, this disorder often requires a carefully detailed history and prolonged observation before the true causative agent is identified. ACD to nickel occurs often in children with AD and may be misdiagnosed as recalcitrant periumbilical AD. Patients with recalcitrant AD may have concomitant allergic contact reactions, particularly to nickel and less often to topically applied medications and emollients, suggesting the role for patch testing. Positive patch tests for potential allergens other than nickel have been described in up to 45% of children with AD, and half of these are reactions to components in the emollients (avena extract; wheat protein; calendula; lanolin). Children with AD may react to fragrance, antiseptics (chlorhexidine), and even their topical steroid.
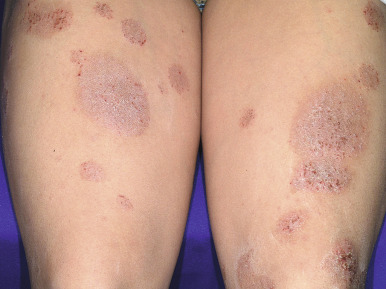
Nummular dermatitis is a distinctive disorder characterized by coin-shaped lesions. Measuring 1 cm or more in diameter, lesions of nummular dermatitis develop on dry skin and are more often seen during dry winter months. The eruption is characterized by discrete erythematous round plaques formed by the confluence of papules and vesicles ( Figs. 3-30 and 3-31 ). Nummular lesions tend to be more recalcitrant to topical therapy and, not uncommonly, become infected so that concomitant treatment of secondary staphylococcal infection and measures to limit staphylococcal overgrowth (such as dilute sodium hypochlorite baths) should be considered.

The lesions of psoriasis, another common skin disease of children, are bright red and topped with loosely adherent silvery micaceous scale (see Chapter 4 ). Psoriatic lesions usually show a sharply delineated edge and have a predilection for the extensor surfaces (particularly the elbows and knees), the scalp, the buttock, and the genital regions. Approximately 5% of children with psoriasis also show dermatitis, either as typical psoriasis and atopic dermatitis lesions or a psoriasiform dermatitis; these children often have a family history of both atopy and psoriasis.
Scabies in infants and children is commonly complicated by eczematous changes because of scratching and rubbing of involved areas or the application of harsh topical therapeutic agents. The diagnosis of scabies is best made by the history of itching, a characteristic distribution of lesions, the recognition of primary lesions (particularly the pathognomonic burrow when present), positive identification of the mite on microscopic examination of skin scrapings, and the presence of infestation among the patient’s family or associates (see Chapter 18 ).
Langerhans cell histiocytosis (LCH) most commonly occurs before 3 years of age (see Chapter 10 ). In affected neonates, reddish-brown, purpuric, crusted papules or vesiculopapules are typically present. In infants this skin eruption is often characterized as a scaly, erythematous seborrheic eruption on the scalp, behind the ears, and in the intertriginous regions. On close inspection the presence of reddish-brown, petechial or purpuric lichenoid papules or vesicular or crusted papules in infants is typical. Cutaneous biopsy and identification of CD1a+ Langerhans cells by immunostaining confirms the diagnosis of LCH.
Acrodermatitis enteropathica is an autosomal recessive disorder characterized by vesiculobullous eczematoid lesions of the acral and periorificial areas, failure to thrive, diarrhea, alopecia, nail dystrophy, and frequent secondary bacterial or candidal infection (see Chapters 2 and 24 ). The characteristic distribution of lesions accompanied by listlessness, diarrhea, failure to thrive, and low serum zinc levels differentiate lesions of acrodermatitis enteropathica from those of AD. Usually a disorder in formula-fed babies with the hereditary form, acrodermatitis enteropathica may also occur in breastfed babies owing to deficient zinc secretion into maternal breast milk.
Dermatitis during the neonatal or infantile periods is also seen in immune dysregulation, polyendocrinopathy, enteropathy, X-linked (IPEX) syndrome, which manifests with early onset intractable diarrhea and type 1 diabetes mellitus as well. The disorder is often fatal during the first year of life. The cutaneous manifestations are seen in 70% of affected babies and tend to be the first sign. Although an atopic-like dermatitis is most common, the eruption has also been described as psoriasiform or resembling ichthyosiform erythroderma. Lesions are often pruritic, secondarily infected by S. aureus , and resistant to treatment with topical corticosteroids. Other common cutaneous manifestations include severe cheilitis, onychodystrophy, and alopecia.
Infections of the upper and lower airways and GI tract are also common, and affected patients may succumb to sepsis. Food allergies and high levels of IgE and eosinophils are also associated. The autoimmune enteropathy is characterized by persistent, watery, and sometime mucoid or bloody diarrhea during the neonatal period, resulting in malabsorption and failure to thrive. The type 1 diabetes is difficult to control and results from lymphocytic infiltration of the pancreas. Other autoimmune symptoms, such as hypothyroidism, cytopenia, hepatitis, nephropathy, and arthritis can develop in patients who survive the initial acute phase.
IPEX syndrome results from mutations in FOXP3, leading to absent or dysfunctional regulatory T cells and self-reactive T-cell activation and proliferation. Detection of enterocyte autoantibodies helps to make the diagnosis. Treatment generally includes supportive care and systemic immunosuppressive therapy (steroids, methotrexate, tacrolimus), although rapamycin has shown promise. Stem-cell transplantation is the curative treatment if a suitable donor can be found.
Typical AD may be a feature of several forms of immunodeficiency, most notably in Wiskott–Aldrich syndrome (WAS) and the hyperimmunoglobulinemia E syndrome (HIES) (see related sections). These disorders are distinguished from AD by their recurrent noncutaneous infections and other characteristic features (e.g., thrombocytopenic purpura, bloody diarrhea, and purpuric lesions in WAS and facial and intertriginous staphylococcal abscesses in HIES).
Prognosis and Effect on Quality of Life
Although studies in the past have shown that AD tends to clear in 43% of children by age 3 and in up to 70% by puberty, recent studies have shown a 1-year prevalence of AD in adults of up to 10.2% and that more than 80% of children with mild to moderate AD have recurrent symptoms or require medication use at least into the second decade of life. Longitudinal studies are needed to verify data suggesting that most patients with AD have persistence of at least some form of their skin disease (often hand eczema) into adulthood.
The quality of life in infants, children, and adolescents with moderate to severe dermatitis is significantly reduced, and having severe AD during childhood can have a great impact on psychosocial development. Infants with AD have been shown to be excessively dependent and fearful. Sleep disturbance affects up to 60% of children with AD overall and 83% of children during flares. Neurocognitive function is impaired in children with sleep problems. Even in clinical remission, children with AD show more sleep disturbance than healthy children, including increased nocturnal wakefulness and a longer latency to rapid-eye-movement (REM) sleep. Recent studies have also shown a strong association of AD with attention-deficit/hyperactivity disorder (ADHD) that is associated with more severe disease and sleep deprivation, reinforcing the impact of these factors on neurocognitive function. Disfigurement associated with moderate to severe AD, coupled with the reduction in sleep, restlessness, and fatigue at school, as well as limitations in participation in sports, isolates the affected child and strains relationships with peers and with teachers. AD is also associated with an increased odds ratio of depression, anxiety, conduct disorder, and learning delay. Children with AD have a higher risk of injury requiring medical attention, related both to comorbid psychiatric and behavioral disorders and their atopy.
As a chronic disorder that requires frequent attention, the family carries a high financial burden of parental missed days from work for doctor visits and home care, lost wages owing to interruption of employment, expensive medications, and the costs of special or additional bedding, clothes, and food. The socioeconomic impact of AD in the United States alone is estimated to be $364 million to $3.8 billion annually. The demonstrated average reduction by 1 to 2 hours of parental sleep nightly also translates into increased parental stress and the tendency of affected children to cosleep with parents affects family dynamics. These stressful psychological factors often exacerbate the AD, as may concurrent infectious illness or the stress of assignments at school.
Management
The management of AD requires patient and parent education, avoidance of irritants and allergic triggers, good moisturization, and use of anti-inflammatory medications ( Table 3-1 ). Patient compliance is the main reason for poor outcome and is fueled by concerns about the use of topical corticosteroids and calcineurin inhibitors (see below). Aggressively but safely managing AD flares is important in preventing the exacerbation of disease by delayed or inadequate treatment. The National Eczema Association (NEA) offers a website for education and patient support ( www.nationaleczema.org ). Age-specific structured educational programs have improved objective and subjective severity scores, and educational videos may improve severity beyond direct education. Written action plans have been shown to improve adherence to therapy. Several new reviews of AD management for children have been published.
| Mild | Moderate | Severe |
|---|---|---|
|
* Barrier repair may be accomplished by application of effective emollients or from barrier-repair agents.
Use of Emollients and Bathing
In general, dryness is worse during cold months when it is aggravated by heat in the house and low humidity. Key to maintaining hydration is the application of a good emollient, particularly within minutes after bathing. In general, the thicker and greasier the emollient, the higher the content of oil relative to water and the more effective the emollient (e.g., ointment is better than cream, which is better than lotion). Nevertheless, nonointment emollients, particularly ceramide-dominant creams, can be substituted when use of a greasy ointment is objectionable and may have inherent anti-inflammatory properties. Some patients, especially those with sensory issues and poor tolerance of ointments and creams, find oils to be helpful, although in general oils do not penetrate the skin as well as oil–water mixtures. Purified sunflower seed oil improves the AD skin barrier, whereas olive oil and mustard seed oil are detrimental to skin barrier recovery and can cause erythema, emphasizing that oils are not interchangeable. Similarly, virgin coconut oil is superior to mineral oil in reducing AD severity and to olive oil in decreasing S. aureus . “Barrier repair” agents, such as N-palmitoyl ethanolamine (MimyX), ceramide-dominant, physiological-lipid based cream (EPI Ceram), and MAS063DP (Atopiclair), also show mild anti-inflammatory properties and may be beneficial for children with mild to moderate AD but are much more costly than emollients.
Preventing the Development of Atopic Dermatitis with Early Use of Emollients
Infants in at-risk families (i.e., with at least one parent or sibling who has AD) have a 30% to 50% chance of developing AD by 2 years of age. Early evidence suggests that limiting the use of skin cleansers and applying an oil-in-water emollient at least once daily may lower the risk or decrease the AD severity.
Water hardness has been shown to be associated with an increased prevalence of AD, and a preliminary analysis suggests that hard water also increases the development of AD in at-risk infants. Although ion-exchange water softeners do not lower the prevalence of AD, other techniques to soften water without adding ions have yet to be tested. Several trials have shown no protective effect of material dietary avoidance during pregnancy and in most cases during lactation on the incidence of AD during the first 18 months of life.
Use of Bathing for Atopic Dermatitis
Although water exposure can increase xerosis through evaporative loss, daily baths hydrate the skin, especially if the water loss is prevented by emollient application within a few minutes after bathing. Baths are also fun for infants and children, contribute to parent–child bonding, and remove surface bacteria and desquamated scale. Whether to limit the duration of bathing is controversial, but many recommend limiting the bath to approximately 10 minutes. Older children and adolescents should be instructed to avoid excessively warm baths and showers. Only mild soaps with lower pH to suppress protease activation (such as Dove or Basis) or soapless cleansers (such as Cetaphil, CeraVe, or Aquanil) should be used if a cleanser is felt to be needed. Bubble baths are contraindicated in moderate to severe AD. Bath oils are only slightly beneficial and because they tend to make the tub slippery should be used sparingly and cautiously.
The addition of dilute sodium hypochlorite (bleach) to the bath (1 mL/L or ¼ cup per half-tub of water) or use of a sodium hypochlorite wash is helpful in controlling the dermatitis of children who with a history of skin infection (see Topical Anti-Inflammatory Medications section). Although the antibacterial effect has been implicated in AD improvement, the recently demonstrated anti-inflammatory effect of sodium hypochlorite may also play a role (see Treatment of Secondary Cutaneous Infections section). Children may complain about sitting in a tub bath because of stinging, particularly during acute exacerbations with raw skin and crusting. In such instances, the addition of 1 cup of salt or baking soda may make the bath more tolerable until more aggressive therapy such as treatment of the secondary infection with oral antibiotics leads to improvement.
Wet wraps of plain water can be applied at night after bathing and emollition or after application of the topical anti-inflammatory agent to decrease pruritus and the sensation of burning at night. Short-term use (up to 14 days) of wet wraps over topical corticosteroids is more efficacious than wraps over bland emollients alone but can be associated with transiently increased steroid absorption. Although wet gauze bandage wraps (such as Kerlix or Kling) are often used in a hospital setting, dressing the young child at home in moist pajamas and socks that cling to the skin and are topped by a dry layer to avoid excessive cooling can be very soothing and promote sleep. Unna boots can also be loosely applied to the legs or arms at night (under self-adherent wraps) to decrease pruritus and protect from scratching.
Open wet compresses may be useful in children with weeping, oozing, or crusted lesions. Aluminum acetate (as in Burow solution, 1:20 or 1:40) is germicidal and suppresses the weeping and oozing of acutely inflamed lesions. Burow solution 1:40 is prepared by dissolving one packet or effervescent tablet (Domeboro) in a pint of cool or tepid tap water. These compresses are applied with a soft cloth such as a man’s handkerchief or strips of bed-sheeting two to three times daily for 10 to 15 minutes for up to 5 days. Washcloths and heavy toweling interfere with evaporation and therefore are not as effective. Compresses should be lukewarm, moderately wet (not dripping), and remoistened at intervals. After the compress, the topical anti-inflammatory agent may be applied.
Avoidance of Irritant Triggers
Many patients have problems with eccrine sweating and sweat retention during the summer months, leading to increased pruritus, especially in the face of lichenification and significant dermal inflammation. The increased vasodilation of already inflamed skin from increased summer heat further contributes to pruritus and cutaneous warmth. Nevertheless, children with AD should be encouraged to participate as actively in sports as possible. Swimming is an excellent sport for children with AD if exposure to chlorinated pool water is tolerated. Children should be coated with an emollient (after sunscreen application) as a protectant against pool chemicals; rinsing immediately after swimming with application of emollient may decrease the risk of irritation. Children should also be kept cool after application of the thick emollient, or if sweating is anticipated, a less occlusive moisturizer should be applied. Air-conditioning is important during hot weather to decrease pruritus. The pruritus and erythematous papules of miliaria rubra, which can develop when sweating and are prevented by an occlusive moisturizer, can be confused by parents with exacerbation of the dermatitis, setting up a cycle of worsening involvement from repeated application of the occlusive emollient. Recognition and education in decreasing the frequency of emollient application are vital in this situation.
Overdressing children during winter months should also be avoided to prevent overheating. The low humidity of winter months and use of indoor heating also increases skin xerosis and may promote dermatitis; humidifiers maybe useful but may increase the exposure to mold allergens if they are not cleaned often. Saliva is a major irritant for infants with AD, and exposure to large amounts of saliva with teething and eating, including saliva mixed with food, exacerbates the facial dermatitis. Protecting the face before meals or naptime with a thick, protective emollient may be helpful. Similarly, older children with AD are at risk for lip-licker’s dermatitis because of the irritant effects of saliva.
Attention to clothing is also important. Soft cotton clothing is recommended over wool or other harsh materials, which tend to precipitate itching and scratching, and in one study fabric softener decreased skin dryness. There is only low-quality evidence regarding AD improvement or decrease in bacterial colonization from use of special textiles, particularly silk and silver-coated cotton, but there is no evidence of harm. Affected children should avoid use of harsh soaps and detergents, fabric softeners, products with fragrance, and bubble baths. Smoking of cigarettes in homes of children with AD should be avoided, because it can lead to an increase in irritation and pruritus and may also increase the tendency toward subsequent development of asthma.
Avoidance of Triggering Allergens
It may be possible to identify potential allergen triggers by taking a careful history and doing selective allergy tests. However, triggers that can easily be avoided are difficult to find for most affected individuals, and without a documented or proven food allergy, avoiding potentially allergenic foods as a means of managing AD is not recommended. Testing for allergy to milk, egg, peanut, wheat, and soy is recommended in children younger than 5 years of age with moderate to severe AD who have persistent AD despite optimized management with topical therapy and/or have a reliable history of an immediate reaction after ingestion of a specific food. Food antigen-specific IgE (sIgE) levels correlate better than a radioallergosorbent test (RAST) and prick tests, but the level of sIgE is not clinically useful for predicting the development of clinically relevant food allergy. Negative skin-prick tests or serum allergen-specific IgE levels are highly predictive at eliminating potential allergens. However, at 6 months of age, 83% of patients with severe AD show IgE food sensitization to milk, eggs, and/or peanuts, and 65% of these children retain food sensitivity by 12 months of age. In comparison, 5% of 6-month-old infants and 11% of 12-month-old infants without atopy show IgE food sensitization. Fewer than 40% of children with moderate to severe AD with food sensitization show reactivity during food challenges, and many of these eruptions are urticarial. In a recent longitudinal study, 16% of more than 1000 infants with AD (all severities) developed food allergies, particularly to peanut (7%), milk (4%), and egg (4%) with the highest risk in infants with greater AD severity. Foods may also induce extracutaneous manifestations in pediatric patients with AD, particularly involving the GI tract. Foods may also act as irritants, especially citrus foods, and that reactions to chemicals in foods, such as tartrazine or other colorings, may occur. For children in whom food allergies are suspected to be relevant, comanagement with a pediatric allergist is recommended.
Despite the fact that maternal dietary antigens are known to cross the placenta, most studies have provided no evidence that avoidance of maternal dietary antigens during pregnancy or lactation has a protective effect during the first 18 months of life on the development of AD or on food sensitization by 7 years of age. As a result, breastfeeding without restricting maternal diet as a strategy to prevent food allergy is recommended until 4 to 6 months unless contraindicated for medical reasons. Despite earlier studies suggesting the opposite, more recent analyses have shown that peanut, milk, and wheat intake during pregnancy is associated with reduced allergy and asthma in children, although reduction in developing AD only correlated with wheat consumption. As a result, hydrolyzed infant formulas, rather than cow’s-milk or soy-milk formulas can be given to at-risk infants who are not exclusively breastfed if available and affordable, but they may not affect the risk of AD. Solid foods, including potentially allergenic foods, should not be delayed beyond 4 to 6 months of age in at-risk infants.
The most common food allergens often contaminate other foods and are difficult to avoid entirely. Restrictions in diet should not worsen the quality of the patient’s and family’s life more than the AD itself. Challenges of agents that may trigger IgE reactivity are best conducted under medical observation, because anaphylaxis has occasionally been reported. It should be remembered that excessively restrictive diets in atopic children may lead to weight loss, calcium deficiency, hypovitaminosis, and kwashiorkor. Proper nutritional counseling and supplementation should be included in management, including warning against the use of protein-poor rice and almond milk for cow’s milk, hydrolyzed, and elemental formulas. After the first few years of life, the risk of significant reactivity to food diminishes (particularly with eggs, milk, soy, and wheat). Unless a careful dietary history suggests food sensitivity as a trigger, improvement through dietary manipulation in children older than 5 years is rarely noted.
In contrast to potential reactivity to foods, reactivity of children and adolescents with AD to aeroallergens increases with age. The most common aeroallergen triggers are house-dust mites ( Dermatophagoides pteronyssinus ), grass pollens, animal dander, and molds, particularly Alternaria . Plant pollens, particularly ragweed, also contain an oleoresin capable of producing sensitization and eczematous contact dermatitis. Air-borne dermatitis may involve the exposed surfaces of the face, neck, arms, legs, and “V” area of the chest but can be distinguished from photosensitivity, which results in sharper lines of demarcation between normal skin and eczematous skin. Exacerbation of facial dermatitis during pollen season or after children contact a pet should alert parents to the possibility of allergy to an aeroallergen or contact allergen (see Allergic Contact Dermatitis section). Cat exposure during infancy can increase the risk of developing AD, especially in infants with an FLG mutation. Cat exposure in children with AD has been shown to increase the risk of developing asthma, although dog exposure may be protective. Epicutaneous application of aeroallergens by atopy patch test on unaffected atopic skin shows reactivity as an eczematoid patch in 30% to 50% of patients with AD but tends to be negative in patients with only respiratory allergy to these triggers or in healthy volunteers. However, patch tests have not been standardized, and their performance and interpretation vary widely. The value toward AD control of mite-allergen avoidance measures (encasing mattresses and pillows, washing bedding in hot water weekly, vacuuming living areas and bedrooms frequently, keeping only soft nonfurry toys, cleaning carpets regularly or removing them, and eliminating pets) is controversial, and a meta-analysis found no value in encasing mattresses to prevent allergic diseases or symptoms. Immunotherapy for food allergies or aeroallergens has long been controversial as treatment for AD, unlike its efficacy for treating allergic rhinitis and extrinsic asthma; recent double-blind, placebo-controlled studies, however, suggest some value of specific oral and sublingual immunotherapy, including to peanuts.
Topical Anti-inflammatory Medications
Topical corticosteroids have been the mainstay of treatment for AD (see Table 3-1 ), and are available in a wide range of potencies from the weakest class VII corticosteroids (e.g., hydrocortisone acetate) to the ultrapotent class I steroids ( Table 3-2 ). The use of more potent topical corticosteroids, particularly when applied to large surface areas, under occlusion, or for long periods may lead to adverse effects ( Box 3-2 ), most commonly local atropy. The face and intertriginous areas are the most susceptible sites and may show local effects, even when weaker steroids are used for prolonged periods. Because of their increased body surface area-to-weight ratio, small children have the greatest risk of systemic absorption of topically applied steroids. Concern about the use of topical steroids has led to “steroid phobia” among families and even physicians. As a result, compliance may be decreased and weak topical steroids insufficient for adequate control may be used. In a recent study, 81% of parents or adult patients with AD had fears about the use of topical steroids, and 36% admitted nonadherence as a result. Recently, topical steroid addiction has been cited as an adverse effect of topical corticosteroids, but it is virtually never seen in children with AD who use topical steroids and should not discourage the use of topical steroids in pediatric patients. In older patients with AD, this disorder is characterized by a burning/stinging, sharply delineated erythematous eruption, primarily on the face and genital region, occurring days to weeks after discontinuation of prolonged, inappropriate, and frequent use of moderate- to high-potency topical corticosteroids. In general, group I corticosteroids are not recommended for patients younger than the age of 12 years, should not be used in intertriginous areas or under occlusion, and require a rest period after 14 days of use. Use of this group of ultrapotent steroids is usually reserved for lichenified plaques and recalcitrant dermatitis of the hands and feet and should be limited. Considering the widespread use of topical corticosteroids, few local adverse reactions occur when topical steroids are carefully chosen and used appropriately based on site of application and severity of the dermatitis ( Fig. 3-32 ). As such, even potent topical corticosteroids may safely be used in small areas for short periods.
| Class | Drug | Dosage Form(s) | Strength (%) |
|---|---|---|---|
| I. Very high potency | |||
| Augmented betamethasone dipropionate | Ointment | 0.05 | |
| Clobetasol propionate | Cream, ointment, foam | 0.05 | |
| Diflorasone diacetate | Ointment | 0.05 | |
| Halobetasol propionate | Cream, ointment | 0.05 | |
| II. High potency | |||
| Amcinonide | Cream, lotion, ointment | 0.1 | |
| Augmented betamethasone dipropionate | Cream | 0.05 | |
| Betamethasone dipropionate | Cream, ointment, foam, solution | 0.05 | |
| Desoximetasone | Cream, ointment | 0.25 | |
| Desoximetasone | Gel | 0.05 | |
| Diflorasone diacetate | Cream | 0.05 | |
| Fluocinonide | Cream, ointment, gel, solution | 0.05 | |
| Halcinonide | Cream, ointment | 0.1 | |
| Mometasone furoate | Ointment | 0.1 | |
| Triamcinolone acetonide | Cream, ointment | 0.5 | |
| III-IV. Medium potency | |||
| Betamethasone valerate | Cream, ointment, lotion, foam | 0.1 | |
| Clocortolone pivalate | Cream | 0.1 | |
| Desoximetasone | Cream | 0.05 | |
| Fluocinolone acetonide | Cream, ointment | 0.025 | |
| Flurandrenolide | Cream, ointment | 0.05 | |
| Fluticasone propionate | Cream | 0.05 | |
| Fluticasone propionate | Ointment | 0.005 | |
| Mometasone furoate | Cream | 0.1 | |
| Triamcinolone acetonide | Cream, ointment | 0.1 | |
| V. Lower-medium potency | |||
| Hydrocortisone butyrate | Cream, ointment, solution | 0.1 | |
| Hydrocortisone probutate | Cream | 0.1 | |
| Hydrocortisone valerate | Cream, ointment | 0.2 | |
| Prednicarbate | Cream | 0.1 | |
| VI. Low potency | |||
| Alclometasone dipropionate | Cream, ointment | 0.05 | |
| Desonide | Cream, gel, foam, ointment | 0.05 | |
| Fluocinolone acetonide | Cream, solution, oil | 0.01 | |
| VII. Lowest potency | |||
| Dexamethasone | Cream | 0.1 | |
| Hydrocortisone | Creams, ointments, lotions, solutions | 0.25, 0.5, 1 | |
| Hydrocortisone acetate | Creams, ointments | 0.5–1 | |

The choice of treatment will depend on the severity and localization of the dermatitis, the age of the pediatric patient, and the history of use of topical anti-inflammatory agents. The least potent preparation that adequately controls the disease process should be used. For children with mild to moderate disease, intermittent use of a low-strength topical steroid with emollient application to maintain clearance usually suffices. However, children with moderate to severe disease often show a cycle of rapid recurrent flaring when topical anti-inflammatory suppression is discontinued. A commonly used regimen to maintain control in these children while minimizing the risk of chronic steroid application is to apply midpotency to potent topical steroids for acute flares (e.g., for a few days to up to 2 weeks twice daily) followed by intermittent therapy with topical steroid, or to avoid continuing steroid altogether, with a topical calcineurin inhibitor. Studies have suggested that topical calcineurin inhibitors can be applied three times weekly to recurrently affected sites to retain control of the dermatitis once improved with the use of topical steroids.
The potency of a topical corticosteroid is largely determined by vasoconstrictor assay and is related to its vehicle as well as to its chemical formulation. Vasoconstrictor assays reveal that generic formulations tend to vary in their clinical activity and their vehicles may at times contain agents differing from those of brand-name formulations. Thus care must be taken in considering substitution of generic formulations for brand-name corticosteroids. The concentration of each topical corticosteroid is only significant with respect to potency relative to other corticosteroids of the same chemical formulation. Accordingly, hydrocortisone acetate 2.5% is much weaker than triamcinolone acetonide 0.1%, which in turn is weaker than clobetasol propionate 0.05%, even though the concentrations would suggest the opposite. It also should be recognized that hydrocortisone acetate differs chemically from hydrocortisone butyrate, hydrocortisone probutate, and hydrocortisone valerate, which as midpotency steroids are stronger than hydrocortisone acetate. Halogenated steroids are usually stronger than nonhalogenated steroids.
Ointments are the most commonly chosen vehicle for treating AD. Corticosteroid ointments afford the advantage of occlusion, more effective penetration, and in general greater efficacy than equivalent cream or lotion formulations. Ointments are particularly effective in the management of dry, lichenified, or plaque-like areas of dermatitis. Ointment formulations, however, may occlude eccrine ducts, inducing sweat retention and pruritus, and hair follicles, leading to folliculitis. As with emollients, formulations in ointments may not be as well tolerated during the summer months of increased heat, perspiration, and high humidity. Creams often contain additives that may be irritating or sensitizing. Creams and lotions, however, are more cosmetically elegant and afford the advantages of greater convenience and acceptability during hot weather and in intertriginous areas. Traditional gels and foams are not well tolerated in individuals with AD, but they may be most effective in the management of acute weeping or vesicular lesions. Topical corticosteroids in emollient-based foam formulations and hydrocolloid gels (in contrast to the alcohol-containing foams and gels) are particularly useful for hairy areas, to avoid occlusion, and for cosmesis. Oil preparations are most commonly used for scalp dermatitis. Best applied to a wet scalp, oil formulations can be shampooed out after at least 1 hour to overnight. A fluocinolone acetonide oil preparation, however, has been shown to be helpful after the bath for children with extensive AD.
Occlusion of treated areas with polyethylene film such as Saran wrap or the use of corticosteroid-impregnated polyethylene film (Cordran tape) enhances the penetration of corticosteroids up to 100-fold. This mode of therapy is particularly effective for short periods (8 to 12 hours a day on successive days) for patients with chronic lichenified or recalcitrant plaques of dermatitic skin. Occlusive techniques, however, are contraindicated for prolonged periods of time and are not recommended in infected or intertriginous areas. Given that the diaper is an occlusive dressing, application of steroids in the diaper area of infants should be avoided or limited to short-term use of low-strength topical steroids.
For sites of severely lichenified dermatitis, salicylic acid can be compounded into preparations with steroids to improve penetration. Tar (liquor carbonis detergens or crude coal tar) can be also be used as an adjunctive therapy in patients with chronic dermatitis in the form of tar baths (e.g., Cutar) or compounded with topical corticosteroids (e.g., compounding triamcinolone 0.1% with 6% salicylic acid and 5% to 10% liquor carbonis detergens in Aquaphor ointment). The objectionable odor, staining properties, potential for irritation, risk of causing folliculitis, and low potential risk of later carcinogenesis make tar a choice only for only selected patients.
A variety of steroid-free topical anti-inflammatory agents have been introduced to allow patients to decrease their application of topical steroids and thus associated risks. Topical calcineurin inhibitors (tacrolimus ointment 0.03% and pimecrolimus cream 1%) have been approved for the past decade as an alternative therapy for AD in children older than 2 years of age. Several studies and anecdotal reports have suggested good efficacy and safety for tacrolimus ointment 0.1% (above 2 years of age) and for tacrolimus 0.03% ointment and pimecrolimus cream in infants under 2 years of age, but their use is off-label. Tacrolimus and pimecrolimus prevent the formation of a complex that includes calcineurin, a phosphatase. Without this complex, the phosphate group from the nuclear factor of activated T cells (NF-AT) cannot be cleaved, the NF-AT transcription factor cannot be transported to the nucleus, and production of cytokines associated with T-cell activation is inhibited. Tacrolimus and pimecrolimus also inhibit mediator release from mast cells and basophils and decrease IgE receptor expression on cutaneous Langerhans cells.
To date, the only confirmed safety issue associated with the use of calcineurin inhibitors in children is burning or pruritus with application, described in the minority of affected children, particularly those with active inflammation. This sensation has been shown to result from stimulation of TRPV1 receptors in skin with depletion of substance P. Calcineurin inhibitors do not show the atrophogenic potential of the corticosteroids and can be safely used on the head, neck, and intertriginous areas. Furthermore, no adverse effects on the eyes have been found, allowing safe application in periorbital areas. No increase in cutaneous infections has been noted in children. Tacrolimus ointment shows good efficacy in children with moderate to severe AD the efficacy of the 0.1% ointment is comparable to a midpotency topical corticosteroid, and that of the 0.03% ointment to a low-potency steroid. Pimecrolimus cream is also comparable to a low-potency steroid and is indicated for pediatric patients with mild to moderate AD. Assays of systemic absorption of tacrolimus and pimecrolimus have shown transient low levels in the blood, if at all, and no adverse effects on systemic immunity have been demonstrated.
In 2006, the US Food and Drug Administration placed a black box warning on the class of calcineurin inhibitors based on the theoretical potential for topical calcineurin inhibitors to cause skin carcinogenesis and lymphoma. This theoretical risk was based on the known risk of malignancy (posttransplant lymphoproliferative disease and nonmelanoma skin cancer) in transplant patients who are profoundly immunosuppressed by systemically administered tacrolimus and in animal studies when treated with 26 to 47 times the maximum recommended dosage. However, the number of malignancies and lymphomas is very low in AD children in postmarketing registries, and task forces of the American College of Allergy, Asthma, and Immunology; the American Academy of Allergy, Asthma, and Immunology; and the American Academy of Dermatology found no evidence to support the issuance of a black box warning. Nevertheless, pimecrolimus and tacrolimus are best used intermittently in rotation with topical steroids, and patients need to be advised of these potential risks, as well as to practice sun protection while using these agents. Several new nonsteroidal anti-inflammatory medical devices (also known as “barrier-repair agents”; see related text) have also become available for mild to moderate dermatitis and may decrease the need for steroid application. Phosphodiesterase 4 inhibitors (oral apremilast and topical crisaborole) are currently in trials as new nonsteroidal approaches for treating AD.
Role of Antihistamines
Reduction of the pruritus of AD is best achieved by application of topical anti-inflammatory medications. Sedating antihistamines, such as hydroxyzine, diphenhydramine, and doxepin, may help itchy children fall asleep, although they have little direct effect on the pruritus itself. Nonsedating antihistamines may be valuable as treatment for other atopic conditions such as allergic rhinitis and have been shown to decrease the risk of urticaria, but their value in decreasing pruritus is unclear, because they are usually nonsedating. Long-term use in young children has not led to behavioral, cognitive, or psychomotor developmental abnormalities. Regardless, many pediatric dermatologists use both sedating and nonsedating antihistamines as part of an overall atopic dermatitis treatment program and attest to their clinical benefit.
Treatment of Secondary Cutaneous Infections
Antistaphylococcal antibiotics are important in the management of patients with heavy S. aureus colonization or infection because of the role of S. aureus overgrowth in triggering dermatitis. Topical antibiotics, such as mupirocin, or fusidic acid (not currently available in the United States) can be used for localized impetiginized lesions, but systemic antibiotics are required for more extensive involvement. Despite the increase in community-acquired (CA) MRSA nationally, most atopics still harbor MSSA (84% to 93%). As a result, cephalexin is still used most commonly (and successfully) to empirically treat secondarily infected dermatitis and will cover both staphylococcal and streptococcal organisms. The chronic administration of systemic antistaphylococcal therapy for AD should be avoided in an effort to minimize the risk of development of MRSA in the atopic population.
Dilute sodium hypochlorite (bleach) baths are now standard of care as a maintenance measure for decreasing flares in moderate to severe AD. The addition of ½ cup of 5% to 6% sodium hydroxide per full tub of water (1 mL/L or 4 mL per gallon) markedly reduces the severity and extent of the dermatitis in children with a history of staphylococcal infections. Even daily maintenance dilute sodium hypochlorite baths are generally well tolerated and may be needed for more severe AD. A washcloth can be used to distribute the bleach-bath water to the head and neck, avoiding the eyes and mouth. If skin erosions from secondary infection make bathing uncomfortable, postponing bleach baths until after the first few days of treatment may be necessary. If a bath is not possible, a 5- to 10-minute wet compress with bleach solution or a shower using a sodium hypochlorite-containing wash (such as CLn) can be used. Intermittent application of mupirocin ointment to the nares and hands of patients and caregivers twice daily for five sequential days each month, and use of gentle antibacterial soaps may also decrease colonization.
Antiviral treatment of cutaneous herpes simplex infections is important in preventing widespread dissemination, which rarely is life-threatening. Administration of oral acyclovir (100 mg tid to qid for children under 6 years of age; 200 mg qid for older children) for a week usually controls the infection. More extensive involvement may require hospitalization and intravenous acyclovir treatment, especially in younger children. For children with recurrent EH, a course of prophylactic administration of oral acyclovir once daily for 6 months or longer effectively suppresses the recurrences. Adjunctive therapies include topical compresses and concurrent administration of topical or systemic antibiotics if bacterial infection is also suspected. In general, topical corticosteroids can be continued during the course of systemic acyclovir therapy without impacting clearance of the viral infection if the dermatitis is problematic. Molluscum infections (see Chapter 15 ) can be managed by curettage after application of topical anesthetics, or if available, by cantharidin application. Children with molluscum and AD (but not nonatopical) may show improvement in both their dermatitis and the molluscum lesions by treatment with high doses of oral cimetidine (40 mg/kg per day divided twice daily) for a 3-month course. Imiquimod has not been found beneficial in double-blind, randomized trials.
Other Considerations for Atopic Dermatitis that Fails to Respond: Adherence and Alternative Diagnoses
Moderate to severe AD may be recalcitrant to topical corticosteroid and calcineurin therapy. Although secondary staphylococcal infection is a common reason for recalcitrance, several other factors should be considered before initiating systemic immunosuppressive therapy or phototherapy. Poor adherence is a major reason for failure to respond. In one study with electronic-cap monitoring to detect opening of tubes, mean adherence of patients with mild to moderate atopic dermatitis was 32%, increasing on or near office visit days. Shortening the time between prescription of the medication and the follow-up office visit ; prescribing once-a-day treatment; using sticker charts to engage children ; providing adequate education about the disease, the use of treatment, and why it is needed; and adapting instruction on medication utilization to existing elements of the family routine (e.g., linking to bathing or brushing the teeth) may be helpful.
Chronic, unresponsive dermatitis, especially involving the eyelids, hands, feet, or vulva may result from ACD, and comprehensive patch testing should be undertaken (see Contact Dermatitis section). Several other alternative diagnoses that may require different intervention are described (see Differential Diagnosis section).
Management of Children with Severe Atopic Dermatitis Requiring Systemic Immunosuppressive Therapy
Systemic immunosuppressive therapy or ultraviolet light treatment can be considered for patients with recalcitrant moderate to severe disease. Narrow-band ultraviolet-B light therapy, which avoids intervention with systemic immunosuppressive therapy, has been reported to cause at least moderate improvement in 89% of children and complete clearance in 40% over a median of 3 months. Nevertheless, the requirement for frequent treatments in a medical office (two to three times weekly) and holding still in a hot, enclosed box while wearing protective goggles, as well as the unknown risk of long-term cutaneous damage from ultraviolet light, complicate the use of this form of therapy for most pediatric patients.
Systemic corticosteroid therapy is effective for most patients with AD, but the rapid rebound after discontinuation of therapy and high risk of potential side effects make its use impractical for patients with AD. Systemic administration of nonsteroidal anti-inflammatory medications to children with AD has largely replaced the use of systemic corticosteroids by pediatric dermatologists in the management of more recalcitrant severe AD.
Cyclosporine has the most rapid onset of action and greatest efficacy but also the highest risk of potential side effects. Therapy is initiated with 3 to 5 mg/kg per day (microemulsion for preferred). Response may be seen within 1 to 3 months, but medication should be tapered once significant improvement is achieved; trough levels can be determined in patients without a sufficient response to determine if a higher dosage can be administered. Discontinuation of treatment usually leads to relapse flares, but low-dose continuing treatment or intermittent courses in children can be effective. Several experts now recommend initial treatment with cyclosporine to rapidly suppress the severe AD (for 3 months) followed by continued treatment with ultraviolet light treatment or an alternative, safer immunosuppressant such as mycophenolate mofetil or methotrexate. Renal and hepatic function and blood pressure must be carefully monitored during cyclosporine therapy.
Azathioprine (2.5 to 3.5 mg/kg per day) has effectively suppressed severe, recalcitrant AD in 58% to 92% of children during a 3-month trial. Pretreatment determination of thiopurine methyltransferase level can predict the risk of developing myelosuppression, and hepatic functions should also be monitored. In one study the thiopurine methyltransferase (TPMT) levels changed unpredictably during treatment in 25% of patients, suggesting that periodic assessment of TPMT levels is warranted to optimize clinical response. Azathioprine should be used with caution, given its recent link of hepatosplenic T-cell lymphoma.
Mycophenolate mofetil has been found to cause at least 60% improvement in 91% of treated children with a dosage of 40 to 50 mg/kg per day for children and 30 to 40 mg/kg per day for adolescents with maximal effects at 8 to 12 weeks. Complete blood counts and liver function testing should be performed.
Methotrexate was found to be effective or very effective in 75% of children with severe AD in a recent retrospective analysis. There were no serious adverse events noted, although 14% experienced minor nausea and 14% had slight elevation in hepatic transaminases. Low-dose therapy (0.3 to 0.5 mg/kg per week) is administered with folate supplementation. The need for a small test dose of methotrexate has not been demonstrated. Complete blood counts should be followed weekly, and hepatic transaminases should be monitored at least monthly.
Interferon-γ downregulates Th2 lymphocyte function, and treatment with recombinant interferon-γ (50 μg/m 2 daily or every other day) has led to improvement in some patients, including pediatric patients. Clinical improvement correlates with decreases in peripheral eosinophilia but not IgE levels. Flu-like symptoms are particularly common early in the treatment course. The high price and benefit for only a subset of individuals also limit the use of interferon-γ in children who are severely affected with AD.
Biologics to date have not been used for pediatric AD. However, weekly subcutaneous injection of IL-4 receptor antibody (dupilumab) shows very promising results in adult AD, consistent with the important role of Th2 cytokines in AD inflammation. An alternative biologic approach may be treatment with ustekinumab to combat the impact of elevation of downstream Th22 cytokine activation, as has been shown effective in adults and an adolescent with severe AD.
Use of Experimental or Complementary Treatment Approaches
The impact of vitamin D3 levels and potential value of vitamin D3 supplementation remain controversial. Low levels of vitamin D3, including in cord blood, have been associated with childhood AD, although there is not a relationship with disease severity unless there is allergic sensitization. Vitamin D3 has been shown to upregulate the expression of cathelicidin, including in the skin of individuals with AD, but topically applied vitamin D3 irritates skin affected by AD. Although one small open-label study of oral vitamin D3 supplementation in children who were vitamin-D deficient with AD showed clinical improvement, a small double-blind trial showed improved serum levels of vitamin D3 after 3 weeks but no clinical improvement in AD. At this time there is insufficient evidence to recommend vitamin D3 supplementation for AD.
Probiotics have recently received considerable attention as a means of prevention of AD. Evidence that reduced diversity in the gut microbiota is a risk factor in the development of AD provides further rationale for probiotic use. Although there is some evidence of benefit prenatally in prevention (for reviews, ) there is insufficient evidence to recommend probiotics as part of standard management of infantile AD. Not all lactobacilli are effective, and Lactobacillus rhamnosus GG has shown the greatest efficacy; in fact, early administration of L. acidophilus did not prevent AD development and increased atopic sensitization. Although early studies suggest some benefit of prebiotics (fiber compounds that stimulate the growth of advantageous organisms) and fatty acids (such as the γ-linolenic acid [GLA] alone or in combination with ω-3 fatty acids), there is insufficient evidence to recommend these approaches for either reducing the risk of developing AD or treating AD.
Leukotriene antagonists such as montelukast, which are used extensively in asthma prophylaxis, have largely been ineffective. The benefit from administration of traditional Chinese herbal therapy has been variable. Regardless, the demonstration of hepatic toxicity, cardiac adverse events, and idiosyncratic reactions from this therapy has raised concerns; furthermore, the discovery of glucocorticoid contamination in some preparations warns that these alternative agents be used with caution. Massage therapy has been advocated as a means to improve the clinical signs of atopic dermatitis in young children, in addition to improving the psychological well-being of the patients and family members. Psychological counseling, behavioral modification, hypnotherapy, and biofeedback can also be helpful in decreasing scratching. Psychological intervention for families can also be beneficial, because increased parental stress and depression correlate with higher levels of biological markers of inflammation. A form of alternative medicine, particularly herbal remedies and homeopathy, is used in 42.5% to 63.5% of patients with AD. More than half reported no improvement but tried the therapies based on recommendation from nonphysicians, concern about the potential risks of topical steroids, and dissatisfaction with conventional treatment. Of concern is that these complementary approaches have potential side effects, have not been adequately tested for safety and efficacy, and require time and effort that might otherwise be directed toward use of physician-prescribed treatment.
Pityriasis Alba
Pityriasis alba is a common cutaneous disorder characterized by asymptomatic hypopigmented patches, usually on the face, neck, upper trunk, and proximal extremities. Individual lesions vary from 1 cm or more in diameter and may show a fine scale ( Fig. 3-33 ). This disorder is thought to represent a nonspecific dermatitis with residual postinflammatory hypopigmentation and occurs more often in individuals with darker skin types. Histologic evaluation shows normal numbers of melanocytes but decreased epidermal melanosomes and melanocyte degeneration. Most cases appear after sun exposure because of the contrast that results between areas that can show a pigmentary response to ultraviolet light and the pityriasis alba areas that do not.

The differential diagnosis of the hypopigmented macules of pityriasis alba includes tinea versicolor, vitiligo, the white macules seen in association with tuberous sclerosis; nevus depigmentosus; cutaneous T-cell lymphoma; leprosy; postinflammatory hypopigmentation secondary to atopic dermatitis, psoriasis, tinea corporis, or pityriasis rosea; and in light-skinned individuals, nevus anemicus. Application of mild topical corticosteroids or calcineurin inhibitors for a few weeks followed by frequent emollition and protection of the sites and surrounding area from sun exposure appears to diminish the dry skin and fine scaling, allowing repigmentation of involved areas. Patients and parents should be warned that, as with postinflammatory hypopigmentation, repigmentation may take several months to years. Effective moisturization during drier months may help prevent recurrence of the pityriasis alba in subsequent summers.
Hyperimmunoglobulinemia E Syndrome
HIES is a rare immunodeficiency disorder characterized by very high levels of IgE in association with AD and recurrent cutaneous and sinopulmonary infections. The AD is seen in 100% of patients, usually within the first 6 months, and is of variable severity ( Fig. 3-34 ). Most patients have an autosomal dominant form (also called Job syndrome ), which results from mutations in the gene encoding signal transducer and activator of transcription 3 ( STAT3 ).

Many neonates or infants with autosomal dominant HIES have pruritic papulopustules, especially on the face, which show eosinophilic folliculitis or eosinophilic dermatitis by biopsy of lesional skin. Infections often begin during the first 3 months of life. Cutaneous candidiasis may also be an early clinical feature (83%). Cutaneous S. aureus infections may take the form of excoriated crusted plaques, pustules, furuncles, cellulitis, paronychia, lymphangitis, or abscesses, especially on the neck, scalp, periorbital areas, axillae, and groin ( Fig. 3-35 ). The abscesses are slightly erythematous and tender but not nearly to the degree expected for a normal individual. Although some patients demonstrate cutaneous manifestations only, patients with HIES usually have recurrent bronchitis and pneumonias with resultant empyema, bronchiectasis, and in 77% of patients, pneumatocele formation. The pneumatoceles tend to persist and become the site of further infections with bacteria ( Pseudomonas ) or fungi ( Aspergillus, Scedosporium ). Rarely, massive hemoptysis ensues. Other common sites of infection include the ears, oral mucosae, sinuses, and eyes. Visceral infections other than pneumonia are unusual.

By late childhood and adolescence, patients with HIES begin to develop progressive facial coarseness, perhaps reflecting bony abnormalities and recurrent facial abscesses. Osteopenia is usually detected by adolescence or early adulthood, and patients have an increased risk of bone fractures, often because of unrecognized or minor trauma. Scoliosis occurs in 64% of patients 16 years of age or older, and hyperextensibility of joints has been reported in 70% of patients. Dental abnormalities associated with HIES syndrome include retention of primary teeth, lack of eruption of secondary teeth, and delayed resorption of the roots of primary teeth. Focal brain hyperintensities and an increased incidence of lymphoma are other features. Patients with HIES of intermediate phenotypes that include staphylococcal and mucocutaneous candidal infections may have STAT3 mosaicism.
The abnormalities in STAT3 signaling impair Th17-cell development, leading to insufficient expression of IL-17 and IL-22, which drive expression of antimicrobial peptides, thus promoting S. aureus and candidal infections. The diagnosis of HIES is largely based on clinical findings and the presence of very high levels of IgE. There are no specific tests to confirm the diagnosis other than the finding of HIES-related mutations. Patients have markedly elevated levels of polyclonal IgE. Although levels of more than 2000 IU/mL are needed to consider the diagnosis in older children and adults, the normal levels of IgE in infants (0 to 50 IU/mL) are considerably lower than those in older children. A 10-fold increase in IgE levels above normal levels for age should trigger consideration of HIES, although these levels of IgE are more common in AD without HIES. Affected individuals tend to have IgE antibodies directed against S. aureus and candida. Levels of IgE are not related to clinical course and may decrease to normal in affected adults. Approximately 93% of patients have eosinophilia of the blood and sputum. Abnormal polymorphonuclear leukocyte and monocyte chemotaxis has been noted, but is intermittent and not correlated with infection. Cell-mediated immunity (Th1-driven) is often abnormal as well and may manifest as anergy to skin testing, altered responses in mixed leukocyte culture, and impaired blastogenic responses to specific antigens such as Candida and tetanus. The decrease in memory (CD27+) B cells is markedly decreased in 80% of patients, in contrast to individuals with AD and high levels of IgE.
Autosomal recessive HIES usually results from loss-of-function mutations in DOCK8 (dedicator of cytokinesis), which regulates the actin cytoskeleton and is less common than the dominant form. Although patients share the cardinal features of high levels of IgE, AD, and infections, patients fail to show the bone, dental, and coarse facial features of the dominant form. Cardinal features that are not part of the STAT3 -deficient form include severe viral infections (molluscum, herpes, and life-threatening cytomegalovirus [CMV] infections), early malignancy (cutaneous and mucosal squamous cell carcinomas), neurologic changes (aneurysms and strokes), and an increased risk of autoimmune issues (anemia, thrombocytopenia, and vasculitis). One patient with autosomal recessive HIES and homozygous mutations in TYK2 (which activates STAT3) had nontuberculous mycobacterial infections. The additional clinical features of recessive HIES have been ascribed to additional abnormalities in IL-12 and interferon-α/β-cytokine production.
HIES must be distinguished from a number of other disorders in which IgE levels may be elevated. Most common is AD, which shows similar inflammatory cutaneous features and often very high levels of IgE, especially if severe ; the concurrent presence of abscesses, coarse facies, noncutaneous infections, and dental and bony abnormalities in HIES may enable differentiation. WAS can be distinguished by thrombocytopenia with cutaneous petechiae and hemorrhagic episodes. Eosinophilia and elevations of IgE levels with dermatitis can also be seen in patients with DiGeorge syndrome, the Omenn syndrome type of severe combined immunodeficiency, graft-versus-host disease (GVHD), and selective IgA deficiency.
The mainstay of therapy for HIES is antistaphylococcal antibiotics, and patients are usually treated prophylactically with trimethoprim-sulfamethoxazole. When other bacterial or fungal infections develop, infections must be treated with appropriate alternative antibiotics. Recombinant interferon-γ has shown inconsistent efficacy. The cutaneous and pulmonary abscesses often require incision and drainage. The pneumatoceles should be removed surgically, especially if present for longer than 6 months, to prevent microbial superinfection. Therapy for AD as discussed in previous sections is also useful for HIES; omalizumab has improved the severe dermatitis of a recalcitrant patient with a relatively low level of IgE. Alendronate sodium may alleviate the osteopenia.
Wiskott–Aldrich Syndrome (WAS)
WAS is a rare X-linked recessive disorder, which in its classic form consists of dermatitis that meets criteria for AD, bleeding from microthrombocytopenia and platelet dysfunction, and recurrent severe pyogenic infections. Bleeding is the most common manifestation, but the presence of mild to severe AD distinguishes WAS from X-linked thrombocytopenia and X-linked neutropenia with myelodysplasia, which are both allelic. The majority of patients are male, but full expression has been reported in girls.
The dermatitis usually develops during the first few months of life and fulfils criteria for AD ( Fig. 3-36 ). Excoriated areas commonly have serosanguineous crust and often show petechiae or purpura. IgE-mediated allergic problems such as urticaria, food allergies, and asthma are also seen with increased frequency.

The hemorrhagic diathesis results from both quantitative and qualitative defects in platelets. Platelets from patients with WAS are small and structurally abnormal with a reduced half-life, although megakaryocyte numbers are normal. Epistaxis and bloody diarrhea are often the initial manifestations. Mucocutaneous petechiae and ecchymoses (see Fig. 3-36 ), spontaneous bleeding from the oral cavity, hematemesis, melena, and hematuria are common, but the severity varies.
Recurrent bacterial infections begin in infancy as placentally transmitted maternal antibody levels diminish and include staphylococcal impetigo, furunculosis, otitis externa and media, pneumonia, pansinusitis, conjunctivitis, meningitis, and septicemia. Infections with encapsulated bacteria such as pneumococcus, Haemophilus influenzae , and Neisseria meningitidis predominate. With advancing age, T-cell function progressively deteriorates and patients become increasingly susceptible to infections caused by herpes and other viruses and to Pneumocystis jiroveci .
Additional clinical features may be hepatosplenomegaly, lymphadenopathy, and autoimmune complications. The most common autoimmune complication is hemolytic anemia, occurring in 36% of patients and usually before 5 years of age. Other autoimmune disorders that clearly seem linked to WAS are autoimmune neutropenia (25%), arthritis (29%), IgA nephropathy, and painful cutaneous vasculitis (22%) that can appear as purplish induration of skin and soft tissues.
The clinical course of WAS is progressive, usually resulting in death by adolescence without transplantation. Overall, 40% of patients die of infection, 21% of hemorrhage (usually intracranial), and 25% of malignant neoplasia. Lymphoreticular malignancies occur overall in 13% to 22% of patients, with an average age of onset of 9.5 years. Non-Hodgkin lymphoma is the most common malignancy and is often linked to Epstein–Barr (EBV) infection, and extranodal and brain involvement predominate. Fewer than 5% who develop lymphoma survive more than 2 years.
Individuals with WAS have mutations in the gene that encodes WAS protein (WASp), and the extent of WASp depletion correlates with disease severity. WASp, through complexing with other proteins, activates Arp2/3 and ultimately polymerizes the actin cytoskeleton to enable cell movement, dendrite formation, formation of immune synapses, T-cell activation, and B-cell homeostasis. Platelet abnormalities result from defective migration in proplatelet formation, inherent platelet defects increasing fragility, and autoimmunity against platelets. T-regulatory cell dysfunction has been blamed for the increased risk of autoimmune complications. The mechanism for the AD is not defined but could relate to T-cell activation defects and the abnormal interactions of WAS Langerhans cells with T cells after antigenic stimulation.
Laboratory studies show thrombocytopenia in 100% of patients, with platelets below about 80,000/mm 3 and often below 20,000/mm 3 . Platelets tend to be small, and aggregation is sometimes defective. Eosinophilia is common, but lymphopenia is not usually seen until after 6 to 8 years of age. Total serum γ-globulin is usually normal, but levels of IgM are often low, with variable IgG levels and increased levels of IgA, IgE, and IgD. The number of T lymphocytes and response in vitro to mitogens may be normal in early life but often decreases with advancing age. Delayed hypersensitivity skin-test reactions are usually absent, and antibody responses to polysaccharide antigens are markedly diminished.
Several conditions may be confused with WAS. Many other immunodeficiencies are characterized by dermatitis, increased susceptibility to infections, and the development of malignancy, but do not share the bleeding diathesis. The clinical findings of hemorrhage, petechiae, and recurrent sinopulmonary infections in WAS help to differentiate WAS from AD.
Bone marrow transplantation with human leukocyte antigen (HLA)-identical marrow is the treatment of choice. Full engraftment results in normal platelet numbers and functions, immunological status, and if T lymphocytes engraft, clearance of the dermatitis. Optimal survival occurs with matched sibling donors and allogeneic transplantation below the age of 5 years (87%). Despite the good result of matched unrelated donors in young children (71%), there is a higher risk of acute GVHD after transplant (56%) versus matched siblings (16%). Mixed chimerism (i.e., engraftment of T cells but not myeloid or B cells) increases greatly the risk of chronic GVHD. If a matched donor is unavailable, infusion of autologous stem cells modified ex vivo by gene therapy is an alternative approach.
Appropriate antibiotics and transfusions of platelets and plasma decrease the risk of fatal infections and hemorrhage. Intravenous infusions of γ-globulin are also useful in patients. Topical corticosteroids may improve the dermatitis, and chronic administration of oral acyclovir is appropriate for patients with EH. Splenectomy has been used selectively for patients with severe platelet abnormalities; however, splenectomy increases the risk of infection by encapsulated organisms, markedly increasing the risk of mortality after transplantation. Children with WAS are unable to mount immune responses after administration of vaccines against encapsulated organisms. Rituximab has been used successfully in some children with EBV-induced lymphoma to prolong survival.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


