There has been particular recent interest in dorsal preservation rhinoplasty techniques because of claims of superior functional and aesthetic results relative to conventional hump reductions. The septum in dorsal preservation rhinoplasty is managed in a variety of ways with differences largely based on the location of septal excision (subdorsal resection, midseptal resection, and inferior septal resection). The technical considerations of a modified subdorsal strip method using a structural preservation technique are described. This technique maintains a subdorsal and caudal strut of cartilage. Patient-reported measures demonstrate significantly improved functional and aesthetic outcomes postoperatively with this procedure.
Key points
- •
Dorsal preservation rhinoplasty is divided into two related components: approaches to the bony nasal pyramid and management of the septum.
- •
Several approaches to the septum have been described in dorsal preservation surgery, each differentiated primarily by the location of septal cartilage excision: subdorsal, midseptal, and inferior septal.
- •
The modified subdorsal strip method (MSSM) allows for a segment of subdorsal cartilage and the entire caudal aspect of the cartilage to be maintained, thereby allowing a structural approach to external preservation rhinoplasty.
- •
Patient-reported measures suggest improved postoperative cosmetic and functional outcomes in those undergoing the MSSM dorsal preservation technique.
Introduction
There has been particular recent interest in dorsal preservation rhinoplasty techniques because of claims of superior functional and aesthetic results relative to conventional hump reductions. , Studies have suggested that rhinoplasty procedures manipulating the nasal dorsum, more so than the nasal tip, have a greater impact on social perception of the nose. Therefore, although the classic Joseph technique of removing dorsal nasal bone and cartilage is a hallmark of rhinoplasty, alternative techniques that avoid dorsal resection have been more recently advocated because of potentially improved functional and cosmetic outcomes. , The concept of preserving the dorsal nasal architecture was introduced in 1899 by the otolaryngologist Goodale and subsequent technical modifications have since been introduced. International rhinoplasty experts published a book in 2018 entitled “Preservation Rhinoplasty” based on this philosophy. This comprehensive text highlights many of the anatomic and technical considerations of preservation rhinoplasty. Fundamentally, dorsal preservation techniques have two related components: approaches to the bony nasal pyramid and management of the septum. This article reviews the approaches and technical considerations as they pertain to the septal work in dorsal preservation surgery, and incorporation of a modified method for dorsal preservation into structural rhinoplasty practices. In particular, the nuances and outcomes of the modified subdorsal strip method (MSSM), as described by the senior author, are discussed.
The bony nasal vault in dorsal preservation
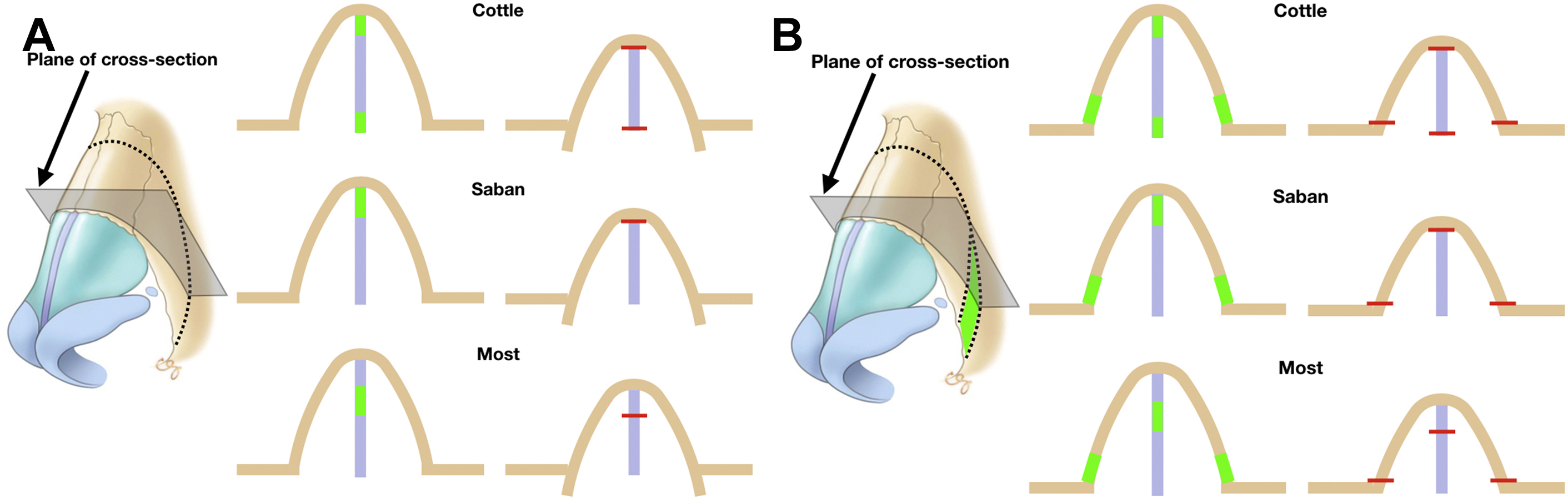
Fundamental to the premise of dorsal preservation surgery is the maintenance of the bony nasal vault and ultimately the dorsal aesthetic lines. An understanding of septal techniques used in dorsal preservation surgery first requires an appreciation for how the bony pyramid is addressed. Although lateral and transverse osteotomies of the bony nasal vault are necessary to allow for lowering of the dorsum, two variations of this approach exist ( Fig. 1 ).
The first, which was initially described by Goodale, , involves single bilateral lateral and transverse osteotomies (without any bone removal), subsequent disarticulation of the nasal-frontal junction, and lowering of the pyramid into the nasal cavity. This technique was further advocated by Cottle and Loring and has become known as the push-down (PD) technique. In comparison, the let-down (LD) technique, first described by Lothrop in 1914, involves similar osteotomies but with the additional resection of bilateral bony wedges along the nasal side wall. The nasal pyramid is lowered and rests on the maxilla as opposed to being advanced into the nasal cavity as in the PD technique. Descent of the nasal bones with the PD technique is limited by the bony attachment of the inferior turbinate to the lateral wall of the nose, and therefore the LD technique has been advocated for humps that are greater than 4 mm in size. The LD procedure can also allow for correction of nasal deviations because an asymmetric wedge of bone is removed between sides. A recent cadaveric study from our group suggests that the PD can cause internal valve narrowing as the bone is forced medially, whereas the LD preserves the nasal valve.
Approaches to the septum in dorsal preservation
Both the bony and cartilaginous septum provide support and attachments to the overlying nasal bone and lateral cartilage. Therefore, regardless of whether the LD or PD technique is used, lowering of the dorsum requires some form of excision and further manipulation of the septum. Two anatomic considerations are important in understanding the movement of the septum in reduction of a dorsal hump using preservation techniques. First, the perichondrium of the cartilaginous vault fuses with the periosteum of the nasal bones over the dorsum, and this junction is flexible. Second, septal cartilage extends subdorsally under the nasal bones such that the bony cap sits above cartilage and not septal bone. Therefore, when a portion of the cartilaginous septum is removed, the dorsum, extending from a point cephalic to the nasal bone–cartilaginous vault junction to the anterior septal angle, descends. Also, the flexibility of the dorsum allows the convexity associated with a hump to be reduced during its decent. Importantly, this process results in not only a lowering effect of the dorsum, but also increased rotation at the anterior aspect of the septum and the nasal tip.
Several approaches to the septum have been described in dorsal preservation surgery, each differentiated primarily by the location of septal cartilage excision (see Fig. 1 ; Fig. 2 ). These include a subdorsal excision, midseptal excision, inferior septal excision, and an MSSM developed by the senior author.
Subdorsal Septal Excision
In Goodale’s , original description of his dorsal preservation technique, he accomplished lowering of the septum by removing a segment of cartilage immediately under the dorsum in a PD procedure (see Figs. 1 and 2A ). Similarly, Lothrop described using subdorsal cartilage resection in an LD procedure. In this approach, which has been championed by several dorsal preservation experts including first Gola and then Saban, an incision is first made along the contour of the dorsal hump immediately under the dorsum and extends to the anterior septal angle. , , Minimal to no septal cartilage remains superior to this incision. A more inferior linear cut is made at a location several millimeters below the dorsal cut. The segment of cartilage between these two incisions is removed and represents the amount of desired dorsal reduction. , As such, the lower incision represents the new dorsal height and corresponds to the intended contour of the nasal profile. Proponents of this technique highlight the control in the design of the lower incision and thereby the ultimate shape of the dorsum. To allow for successful descent of the dorsum, a portion of the subdorsal ethmoid bone parallel to the excised cartilage is also resected. Although a minimal amount of cartilage should remain on the undersurface of the dorsum with this technique, any remaining septum under the osseocartilaginous vault is scored to release tension that may prevent dorsal flattening. Ultimately, the dorsum is sutured to the underlying septum in its lowered position.
Midseptal Excision
An excision in the midaspect of the cartilaginous septum has been advocated for by Ishida and colleagues and Neves and coworkers. With this technique, the subdorsal cartilage is not disrupted and no part of the osseous aspect of the septum is resected. The excision starts from the bony cartilaginous junction and extends anteriorly into the caudal aspect of the septum inferior to the anterior septal angle. In the description by Ishida and colleagues, whereas the septal excision allows for lowering of the cartilaginous nasal vault, the nasal bones are reduced using an osteotome or rasp in a more classic fashion. As such, this is distinct from true dorsal preservation techniques that maintain the dorsal keystone area and where the nasal bones and midvault are treated as a single entity. Nonetheless, a midseptal excision of cartilage, and possibly some bone, could be used to eliminate a dorsal hump while keeping the nasal bones and osseous midvault intact similar to the subdorsal techniques described previously.
Inferior Septal Excision
In 1946, Cottle and Loring described the excision of septal cartilage at the premaxilla in the setting of nasal fractures to allow for adequate mobilization after down-fracture of the nasal bones (see Figs. 1 and 2B ). When applied to rhinoplasty, they found that a similar resection of a strip of cartilage at the maxillary spine allowed for descent of the dorsum. The amount of cartilage removed corresponds to the amount of desired dorsal reduction. To allow for complete removal of a dorsal hump, this inferior cartilage excision is combined with a resection of a vertical 4-mm segment at the bony cartilaginous junction (from the keystone to the vomer) and a resection of the ethmoid bone under the nasal bone. Similar to other techniques, the remaining septal cartilage and thereby the dorsum is stabilized into position via sutures. The complex cuts within the septum and difficulty with anchoring the septal cartilage to the maxillary spine leading to increased operative times have been cited as challenges with this technique.
Modified subdorsal strip method
Technical Considerations
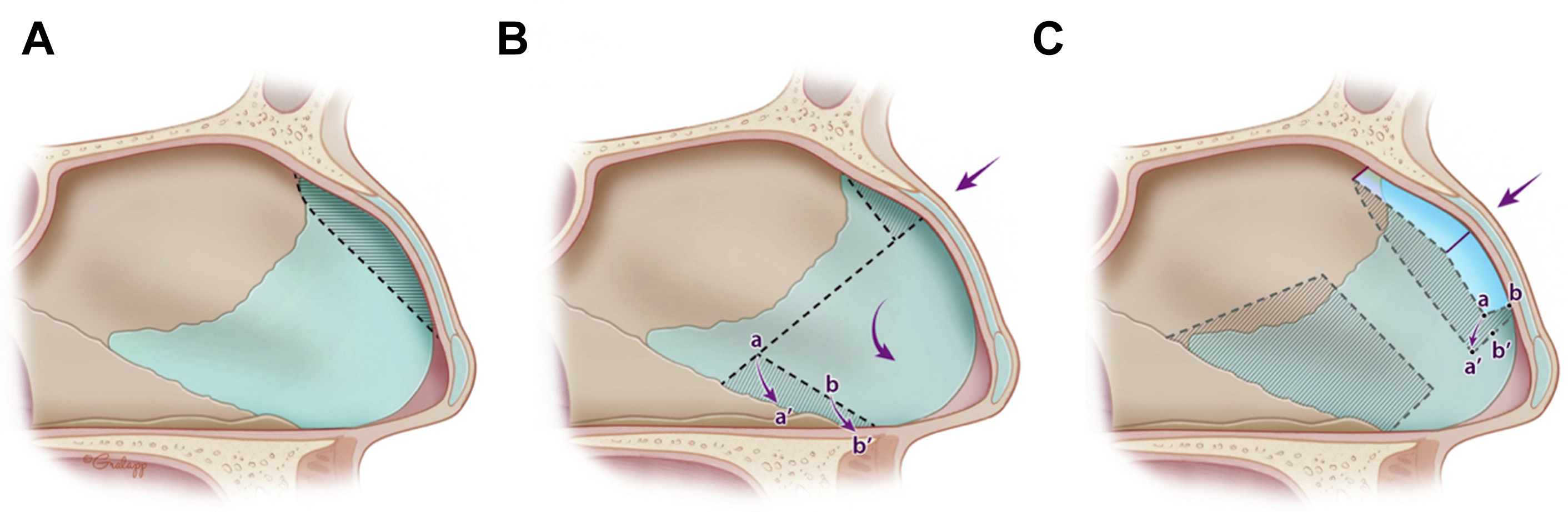
The senior author (SPM) has developed a septal approach to dorsal preservation surgery, termed herein as an MSSM (see Figs. 1 and 2C ). This structural approach is considered an intermediate between the classic subdorsal and inferior septal resections. This concept has been similarly described by Neves and colleagues as a “split preservation method” and modified into the “Tetris concept.” Rather than an immediate subdorsal resection, a 3- to 5-mm subdorsal strip of cartilage is maintained. A cut parallel to the dorsum is made extending from the bony cartilaginous junction toward the caudal septum, but unlike other techniques, this cut terminates posterior to the anterior septal angle. As such, a 1- to 1.5-cm caudal strut of septal cartilage is maintained. The paraseptal cleft, consisting of fibrous attachments between the upper lateral cartilages at the anterior septum, is released to allow for improved visualization of the septum. Importantly, this also allows for unimpacted descent of the dorsum despite the presence of a caudal strut in place. Because the entire caudal aspect of the septum remains intact, it can be used to attach the tripod complex in any desired projected or rotated position. It can also be trimmed secondarily if needed. Although the other aforementioned dorsal preservation septal techniques have been largely performed in a closed or endonasal fashion (with or without endoscopic assistance), an external approach has been implemented at our center for the modified subdorsal septal excision. , , This has allowed for the needed exposure to modify the tip with previously used strategies, such as suture modification of the domes, alar spanning sutures, and cephalic turn-ins. Thus, this method fits the category of “structural preservation” rhinoplasty (a combination of dorsal osseocartilaginous preservation and structural external approach techniques to the tip/tripod complex).
Although a triangular segment of ethmoid bone is classically removed in other techniques, the senior author prefers creating a longitudinal cut into the bony septum such that there is slight side-to-side overlap between bone once there is descent of the dorsum. This can only be performed when the bone is thin, or else axis deviation of the bony vault may occur. This method helps limit overdisplacement of the disarticulated nasal vault into the nose with the open approach in which overlying periosteal attachments have been released. If overmobilization of the nasal bones posteriorly occurs, a radix graft using soft tissue or morselized cartilage may be needed.
Eliminating a dorsal hump, much like in the classic subdorsal resection technique, involves a combination of descent and flexion of the dorsum. This corresponds to lowering and anterior rotation of the septum. To allow for this, several strategies are used. First, one or two vertical incisions are made in the remaining subdorsal cartilage at the apex of the dorsal hump to allow for flexion of the dorsum. In addition, a vertical segment of cartilage anterior to the subdorsal segment is resected to allow for unhindered rotation of the posterior septum. Flexion of the midvault is made easier by cephalically disarticulating the upper lateral cartilages from the ascending process of the maxilla (without violating the lateral keystone area). When done in combination, these maneuvers allow for the subdorsal cartilage to be flexed and ultimately anchored to the remaining inferior cartilage.
A particular benefit of this method, as compared with the Cottle method, is that it allows for resection of the lower and posterior septum. As such, septal deviations are corrected, and cartilage is harvested for grafting purposes. Also, because a caudal strut is maintained without disarticulating it from the maxillary spine, there is no need to stabilize the septum to bone. The stable strut, as previously mentioned, allows repositioning of the nasal tip to the desired position. In addition, if the caudal strut has to be removed because of significant anterior septal deviation, it is replaced and stabilized to the subdorsal strut of cartilage that remains attached to the overlying dorsum and keystone region. For example, anterior septal reconstruction (ASR), a modified extracorporeal septoplasty technique, has been used with success at our center in conjunction with the modified subdorsal resection. , In this technique, an ASR graft is fashioned from septal or rib cartilage and anchored to the subdorsal strut with three 5–0 nonabsorbable monofilament sutures and positioned to sit in a groove created in the maxillary spine. If no suitable groove can be created, the ASR graft is stabilized to the premaxilla using a miniplate.
Surgical Outcomes
To evaluate outcomes with the MSSM, after institutional review board approval, retrospective chart review was performed on patients undergoing septorhinoplasty with this structural dorsal preservation technique. Patients undergoing surgery between June and December 2019 for dorsal hump reduction were included. The Standardized Cosmesis and Health Nasal Outcomes Survey (SCHNOS), a validated patient-reported outcome measure, was recorded preoperatively and postoperatively. , The SCHNOS survey consists of obstructive (SCHNOS-O) and cosmetic (SCHNOS-C) domains (scores ranging from 0 to 100, with 0 being no obstruction or no aesthetic concerns). Descriptive statistics were calculated for the patient population and preoperative and postoperative SCHNOS scores at most recent postoperative follow-up. A paired Student t test was used to compare the mean postoperative SCHNOS-O and SCHNOS-C scores with mean preoperative scores. Similar comparisons were made in patient visual analog scale (VAS) results including a functional scale (VAS-F; 0–10, with 0 being no nasal obstruction) and a cosmetic scale (VAS-C; 0–10, with 0 being no satisfaction with nasal appearance).
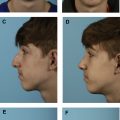
During this period, 22 patients underwent MSSM dorsal preservation rhinoplasty at our center and completed the SCHNOS and VAS surveys during the study period; 19 were female and three were males. Mean ± standard deviation (SD) age was 32.1 ± 11.2. No patient had undergone prior nasal surgery. Ten patients had functional breathing complaints with anatomic obstruction noted on preoperative examination. Of these patients, nine underwent turbinate reduction, nine underwent septoplasty (including three patients who underwent resection of the caudal septum with ASR), and two underwent placement of lateral crural strut grafts. Twelve patients underwent cosmetic surgery alone without any functional elements. Eight patients underwent a PD procedure and 14 underwent an LD operation. Mean ± SD follow-up was 108 ± 56 days. Fig. 3 demonstrates a preoperative, 1-week, and 4-month postoperative example of a patient who underwent a structural dorsal preservation surgery with MSSM. Of note, a structural approach was used for stabilizing and shaping the nasal tip. Namely, tongue-in-groove was used to set tip rotation and projection, and a small cap graft. Bilateral minilateral crural strut grafts, as described by the senior author, were also used.

Related posts:
 Combined Functional and Preservation Rhinoplasty
Combined Functional and Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


