For rhinoplasty surgeons, surgery of the dorsum has never been so dynamic or as easily learned. Reproducible techniques offer excellent results that can be difficult to achieve in certain patients using component reduction. An expanding repertoire of dorsal preservation (DP) techniques is evolving. Each DP operation builds on the others. To understand DP requires a new appreciation of the cartilaginous septum, the perpendicular plate of ethmoid, nasal osteotomies, and anatomy of the nose where surgeons do not operate with traditional component reduction. The result is more beautiful noses where the normal anatomy is preserved.
Key points
- •
Dorsal preservation represents a new frontier in surgery of the nasal dorsum.
- •
Multiple new techniques are evolving allowing for increased applicability of dorsal preservation.
- •
An algorithm is presented for the different forms of dorsal preservation and how to incorporate them into your practice.
Introduction
For rhinoplasty surgeons, surgery of the dorsum is increasingly dynamic and exciting. An expanding repertoire of reproducible techniques offers excellent results that can be difficult to attain in certain patients using conventional methods. Once surgeons understand dorsal preservation (DP), they will look for every opportunity to preserve the dorsum. An enlarging body of techniques is evolving as the most creative and innovative rhinoplasty surgeons push the limits of the philosophy. For beginners, easier techniques should be chosen initially on patients with the most appropriate indications. As the learning curve progresses, it makes sense to advance to the next phase of the preservation journey and to learn the more complicated operations. Each DP operation builds on the others, and, over time, these philosophies make clinicians not only better surgeons of the nasal dorsum but also better surgeons of the septum and the nose in general. To understand DP, surgeons needs to gain a new appreciation of the septum, the perpendicular plate of ethmoid, osteotomies, and anatomy of the nose where they rarely operate with traditional L-strut philosophy. Through this journey, I have evolved as a surgeon, and now I approach rhinoplasty in ways that I did not before. The result is more natural and beautiful noses where the anatomy has been preserved.
Dorsal Preservation
Control of the bony vault, especially the keystone area, is enhanced with the popularity of the full open approach and piezoelectric surgery. However, keystone irregularities, bony spicules, callus formation, asymmetric osteotomies, asymmetries of the middle vault, and long-term contraction can affect dorsal aesthetic lines years after the operation was performed. However, dorsal irregularities (especially in the middle vault) continue to be an issue for rhinoplasty surgeons over the long term. This situation is where DP takes the lead in the rhinoplasty revolution.
Personal experience with dorsal preservation
My introduction to DP came in 2016. The concept was intriguing: preserve the dorsum by lowering the osseocartilaginous vault into the pyriform aperture. Because the keystone would remain intact and the middle vault would not be opened, irregularities/asymmetries/contraction could potentially be avoided. In addition, the prospect of a narrow but stable middle vault was exciting. Up to that point in my career, I learned the hard way that the only way to maintain stability was restructuring, which sometimes widened the middle vault and/or deteriorated over time. After dozens of hours of discussion with Drs Yves Saban and Rollin Daniel, I did my first DP at the end of 2016. Over the next year, other surgeons, including Drs Baris Cakir, Milos Kovacevic, Olivier Gerbault, Charles East, Peter Palhazi, and Abdulkadir Goksel, also began in parallel performing high septal strip DP as advocated by Saban and colleagues. Through hundreds of hours of casual conversations, emails, roundtable discussions, presentations, and meetings, we learned the technical details and were able to understand how to perform the high septal strip push/letdown technique and to achieve stable and predictable results. With 2 years of experience performing the high septal strip DP operation, I found that one-third of my primary rhinoplasty patients were good candidates. What came next was astounding:- the resurgence, development, and modification of techniques that expanded my indications for DP. Throughout 2018 to 2019, several techniques came to the forefront of rhinoplasty surgery, including Valerio Finnochi’s modification of the Cottle technique, as well as the cartilage pushdown techniques championed by Ferreira and colleagues and Ishida and colleagues. More than half of my patients can now successfully undergo DP with excellent results using a variety of techniques, each with its own best indications.
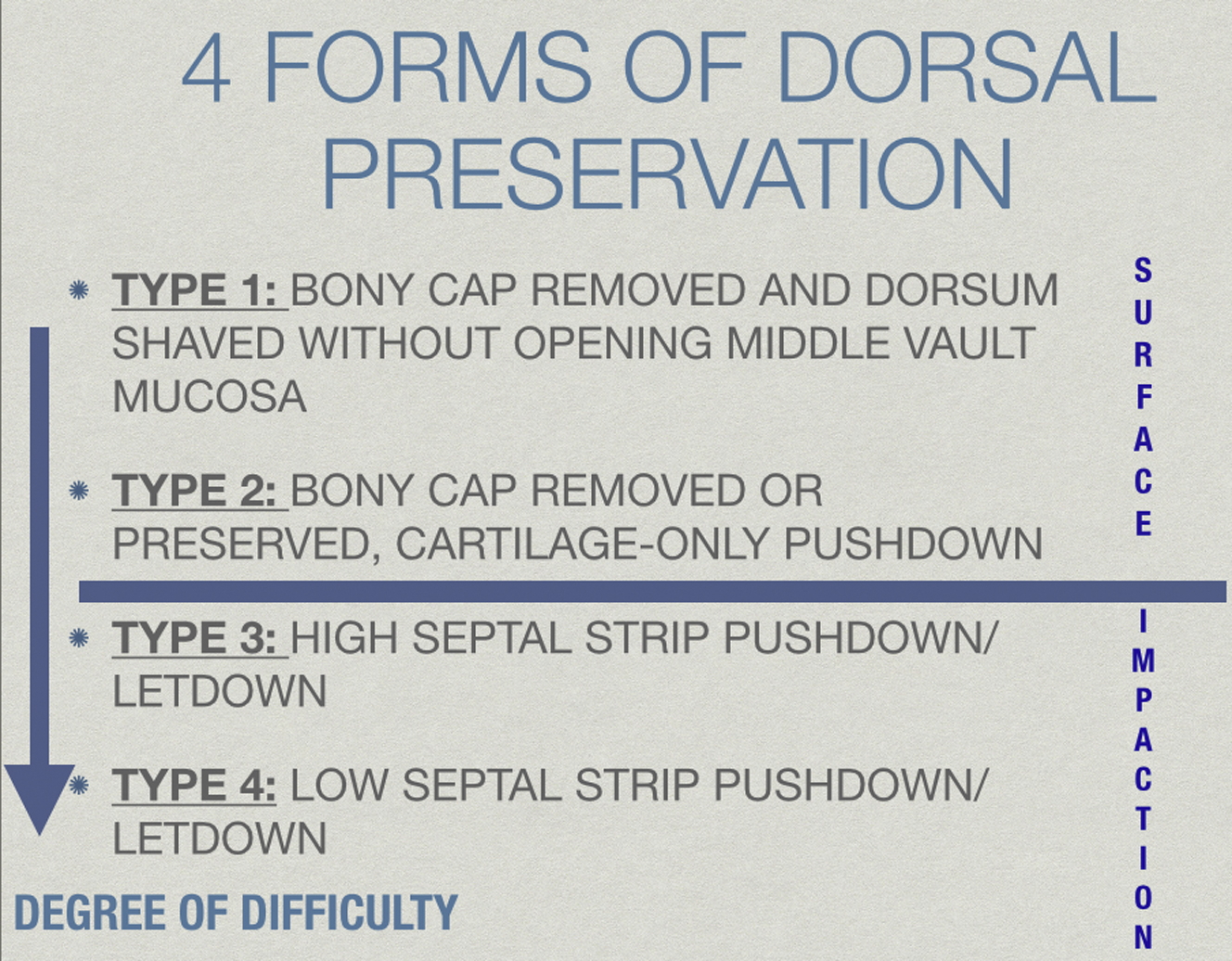
The spectrum of dorsal preservation (types 1–4)
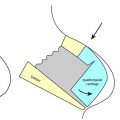
Preservation rhinoplasty is not just DP, and DP is not just a pushdown or letdown impaction procedure. DP is a spectrum of techniques whereby the surgeon preserves all or part of the osseocartilaginous dorsum. More simply, DP can be divided into both impaction techniques as well as surface dorsal modification (DM) techniques. Impaction techniques lower the entire osseocartilaginous vault by (1) first separating the nose from the septum, followed by (2) separating the nose from the face. In contrast, surface or DM techniques lower only the central cartilaginous vault (with or without the bony cap), and the bones are treated separately as in component reduction. Technically, surface techniques are easier to learn and to execute for surgeons beginning DP. In addition, surface techniques widen the applications of the preservation philosophy ( Fig. 1 ).
As surgeons become more experienced with DP, it is preferable to preserve the dorsum and to avoid midvault reconstruction in select patients. Although some surgeons prefer a specific technique for all patients, I prefer to apply the optimal technique for each patient. A summary of my indications for each DP procedure follows, in order of increasing complexity. I have not invented any of these techniques, nor do I prefer 1 technique. I have used all these techniques in hundreds of cases over a 3.5-year period and have become aware of each technique’s inherent advantages and disadvantages in different patients. Each surgeon selects which technique to use based on personal experience and the patient population. The step-by-step technical details of these procedures are summarized elsewhere in this issue, so this article focuses on indications and thought processes.
Type 1 Surface Technique: Dorsal Modification/Cartilage Vault Modification
Cartilage vault modification (CVM) is the simplest technique for DP and an easy entry for beginner surgeons.
CVM modification is a hybrid DP technique that consists of 4 parts:
- 1.
Incremental modification and ostectomy of the bony cap to convert the bony dorsum to cartilage
- 2.
Shaving excess upper lateral cartilage shoulders and/or dorsal septum without opening the mucosa
- 3.
Piezoelectric rhinosculpture and/or osteotomies to narrow and to sculpt the bony pyramid
- 4.
Closing any cartilage defect over the underlying mucosa and shaping the upper lateral cartilages ( Fig. 2 )
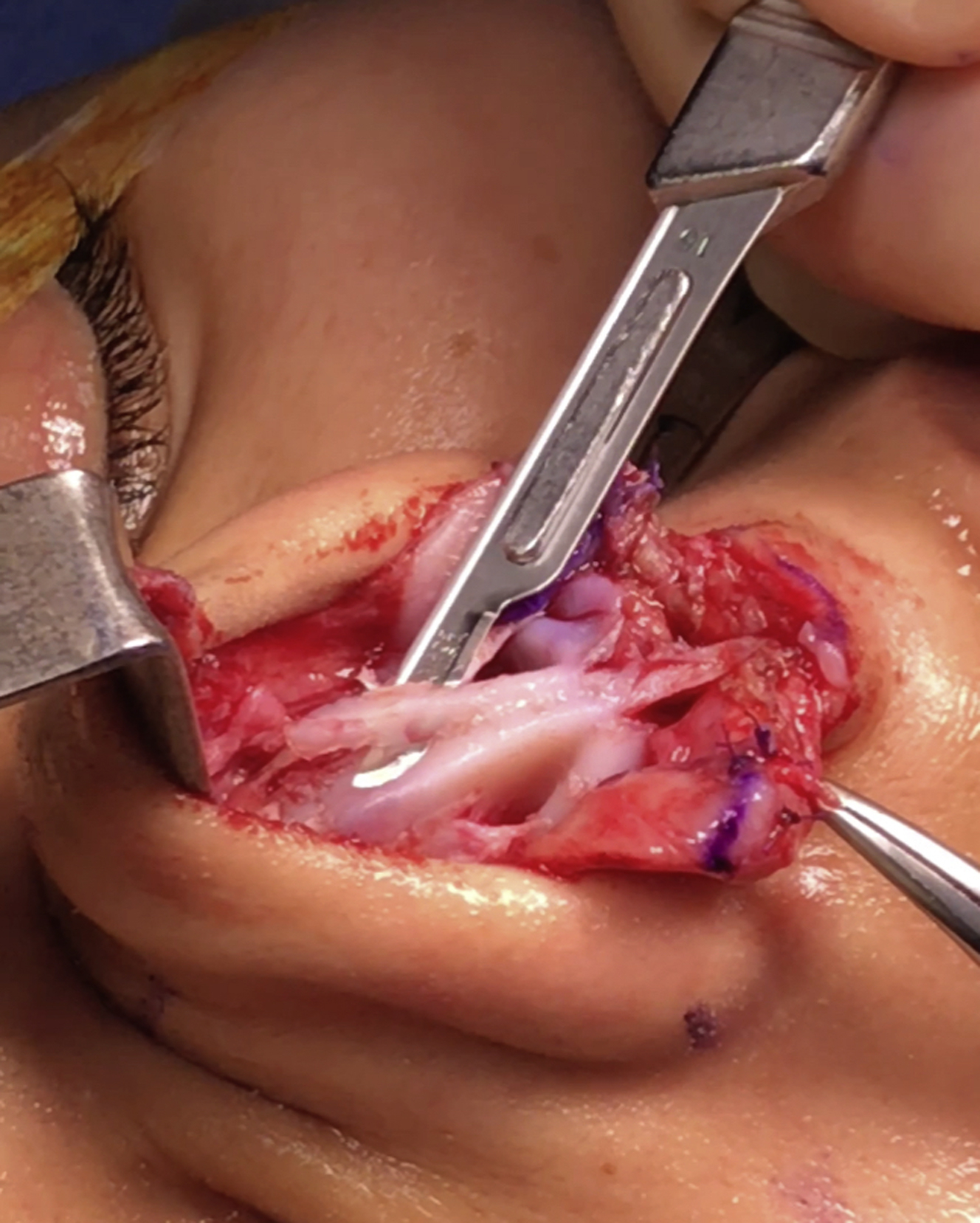
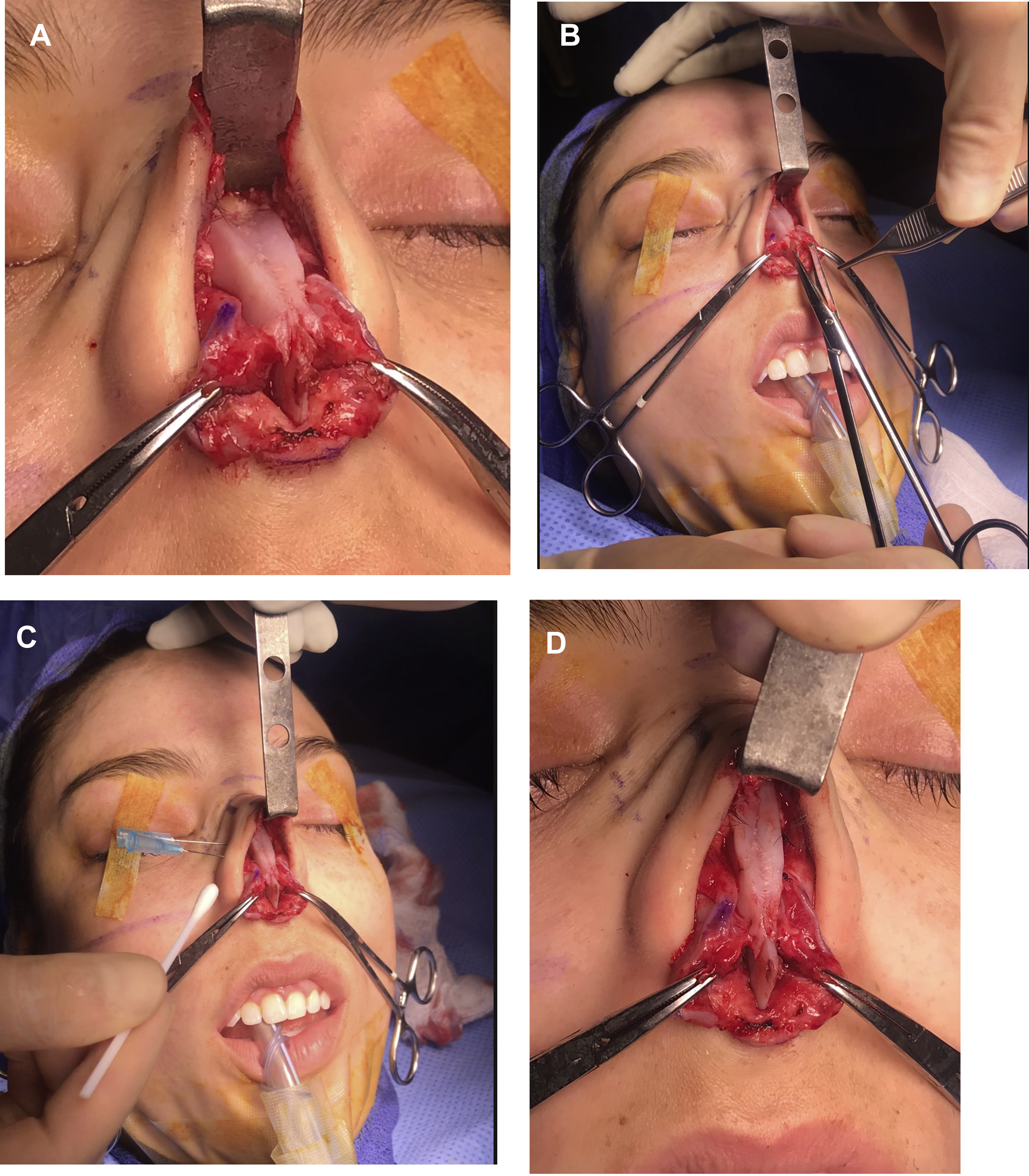
Fig. 2
Piezoelectric removal of the bony cap followed by shaving of the shoulders of the upper lateral cartilage without opening the middle vault. This is DM/CVM.
Thus, CVM is a surface technique whereby only the bony cap is removed, and the cartilaginous vault is modified/lowered. The bones are dealt with separately (as in a component reduction) and no impaction of the osseocartilaginous vault into the pyriform aperture is performed.
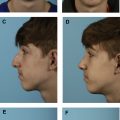
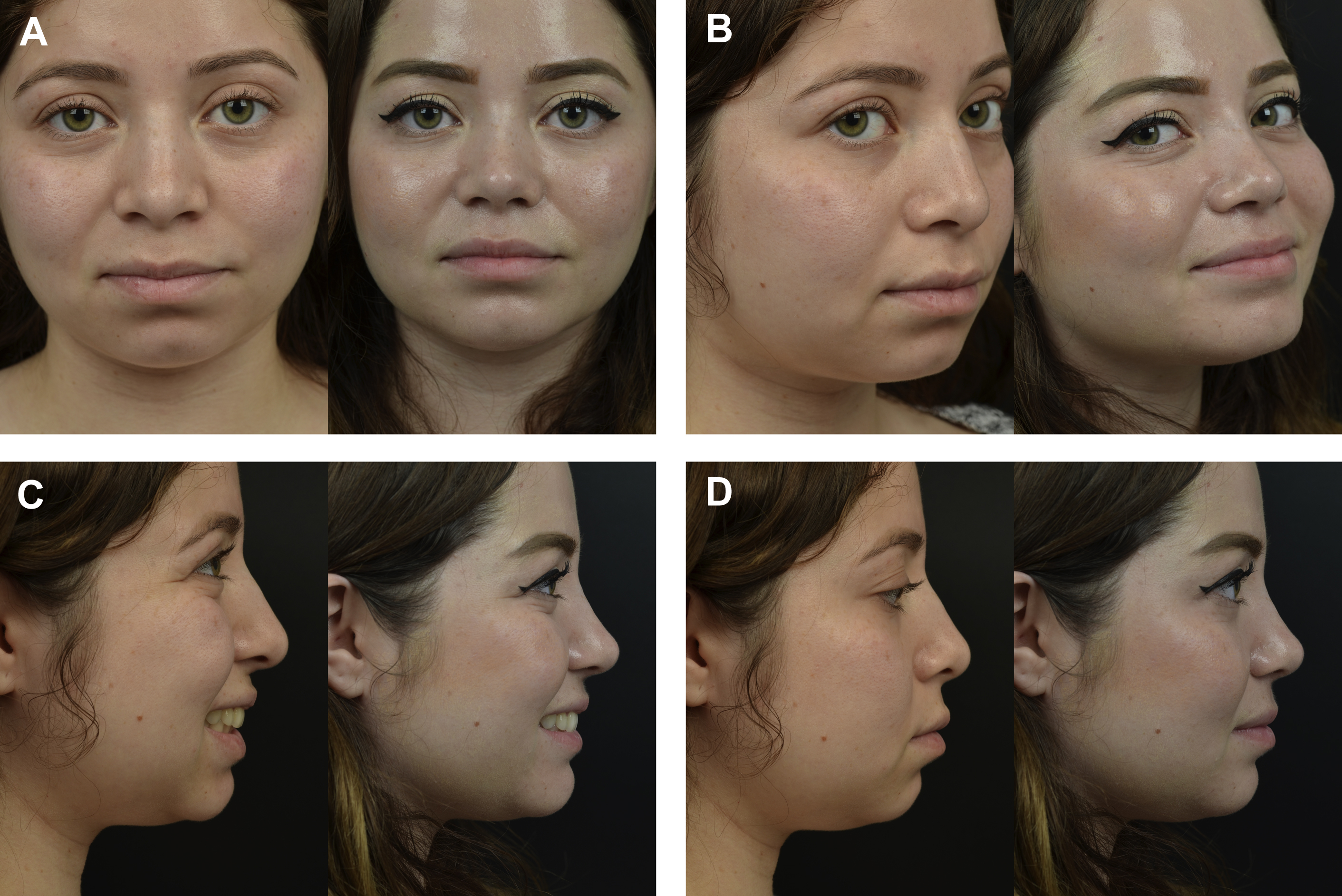
My indications are as follows ( Fig. 3 ):
- •
Small hump/convexity less than 2 mm
- •
Small hump with need for tip projection
- •
Small hump with wide bones and/or need for osteotomies
The main advantage of the CVM technique is simplicity, particularly in an open approach. With a small osseocartilaginous hump, the osseous part is removed up to the desired profile line, and any excess cartilage is shaved. The cartilaginous vault is kept mostly intact, as is the internal valve mucosa. Because the upper lateral cartilages have not been separated from the dorsal septum, there is no need for midvault reconstruction. In addition, endonasal spreader grafts can easily be placed in submucosal pockets to treat asymmetries. The bones are modified as needed with standard osteotomies for narrowing dorsal or base bony width. Of note, the septum remains available for septoplasty and harvesting of graft material, and, if the surgeon gets in trouble, conversion to a standard component reduction is simple.
Type 2 Surface Technique: Dorsal Modification/Cartilage Vault Preservation
Cartilage vault preservation (CVP) is a critical category of techniques in my rhinoplasty practice. It is widely applicable, easy to learn, fast, and has a very low complication rate. CVP can be done using a high or low septal strip.
CVP is a hybrid technique that consists of 4 parts:
- 1.
Preservation or ostectomy of the bony cap to convert the bony dorsum, thereby permitting a cartilage-only pushdown
- 2.
Septal strip resection under the dorsum by removing a high or low septal strip
- 3.
Precise downward fixation of the cartilaginous vault
- 4.
Piezoelectric rhinosculpture and/or osteotomies to narrow and to sculpt the bony pyramid ( Fig. 4 )