Dorsal preservation rhinoplasty has aesthetic advantages over conventional hump takedown rhinoplasty. In dorsal preservation surgery, the nasal vault is treated en bloc. The internal nasal valve angle is not disrupted and there is no need for midvault reconstruction. Two techniques for management of the bony vault exist in dorsal preservation surgery: the let-down and the push-down techniques. There are a variety of techniques used for management of the septum in dorsal preservation. Available patient-reported outcomes of suggest positive results in nasal breathing. More robust data are needed to clarify the functional results of dorsal preservation and compare breathing outcomes.
Key points
- •
In dorsal preservation surgery, the nasal vault is treated en bloc without disarticulation of the upper lateral cartilages from the septum.
- •
Cadaveric studies imply that the let-down dorsal preservation procedure may be superior to the push-down; however, clinical correlation is necessary.
- •
The techniques used to treat the septum in dorsal preservation surgery differ in location of septal cartilage resection.
- •
Dorsal preservation limits damage to nasal mucosa and nasal ligaments with resulting functional implications.
- •
Robust patient-reported outcomes are needed to elucidate the functional implications of dorsal preservation surgery and compare breathing outcomes between conventional and preservation hump reduction techniques.
Introduction
Dorsal hump reduction with the classic technique of removing dorsal nasal bone and cartilage as championed by Joseph has become a hallmark of rhinoplasty. Variations in techniques for tissue removal (eg, composite vs component hump reduction), for osteotomies to close subsequent open roof deformities, and for midvault reconstruction exist in literature. More recently, there has been renewed interest in techniques that prevent resection of the dorsal hump and rather preserve the overall architecture of the nasal pyramid. Much of the interest in dorsal preservation (DP) is due to the avoidance of the potential negative implications of excisional techniques. The maintenance of the structural integrity at the nasal keystone, dorsal aesthetic lines, and the patency of the internal nasal valve are points of DP. , The anatomic and technical considerations of preservation rhinoplasty have been comprehensively reviewed in a book entitled Preservation Rhinoplasty , written by rhinoplasty experts Daniel, Saban, Palhazi, and Cakir. Several experienced surgeons have also reported exceptional aesthetic results with DP techniques. , However, despite the often stated theoretic benefits of DP on nasal airflow, few studies have explored the effect of these techniques on functional outcomes. , , This article provides a review of the functional considerations in DP surgery and available literature on functional outcomes.
The internal nasal valve
The internal nasal valve contributes to the narrowest portion of the nasal airway and is bounded by the caudal edge of the upper lateral cartilage (ULC) laterally and the nasal septum medially. , This angle of articulation is generally 10° to 15°. Inferiorly it is bounded by the nasal bony floor and posteriorly by the anterior head of the inferior turbinate. The degree of collapsibility of the internal nasal valve wall depends in part on the intrinsic stability of the ULCs, and minor changes in the internal nasal valve size result in large changes in resistance of nasal airflow. Given the attachment of the ULCs to the nasal bones, changes in position of the nasal bones are translated to the upper lateral cartilage and thereby may impact the internal nasal valve.
In the standard Joseph hump takedown, the upper lateral cartilages are disarticulated from the septum and the cartilaginous and bony pyramid are reduced in height. The resection of the cartilaginous middle vault disrupts the important relationship between the upper lateral cartilage and the dorsal septum. The upper lateral cartilage is more prone to medial collapse and careful midvault reconstruction is, therefore required. Moreso, it may decrease the cross-sectional area of the internal nasal valve. Overall, this procedure can result in impaired nasal ventilation. In DP surgery, the nasal vault is treated en bloc without disarticulation of the upper lateral cartilages from the septum. This precludes the disruption of the internal nasal valve angle or the need for midvault reconstruction. Overmobilization and mediatization of the nasal sidewalls can occur with standard lateral and medial osteotomies used to close an open roof deformity. This can lead to a narrower nasal vault and nasal obstruction. Because DP techniques treat the entire nasal pyramid en bloc, there is a decreased risk of overmedialization of the nasal sidewall.
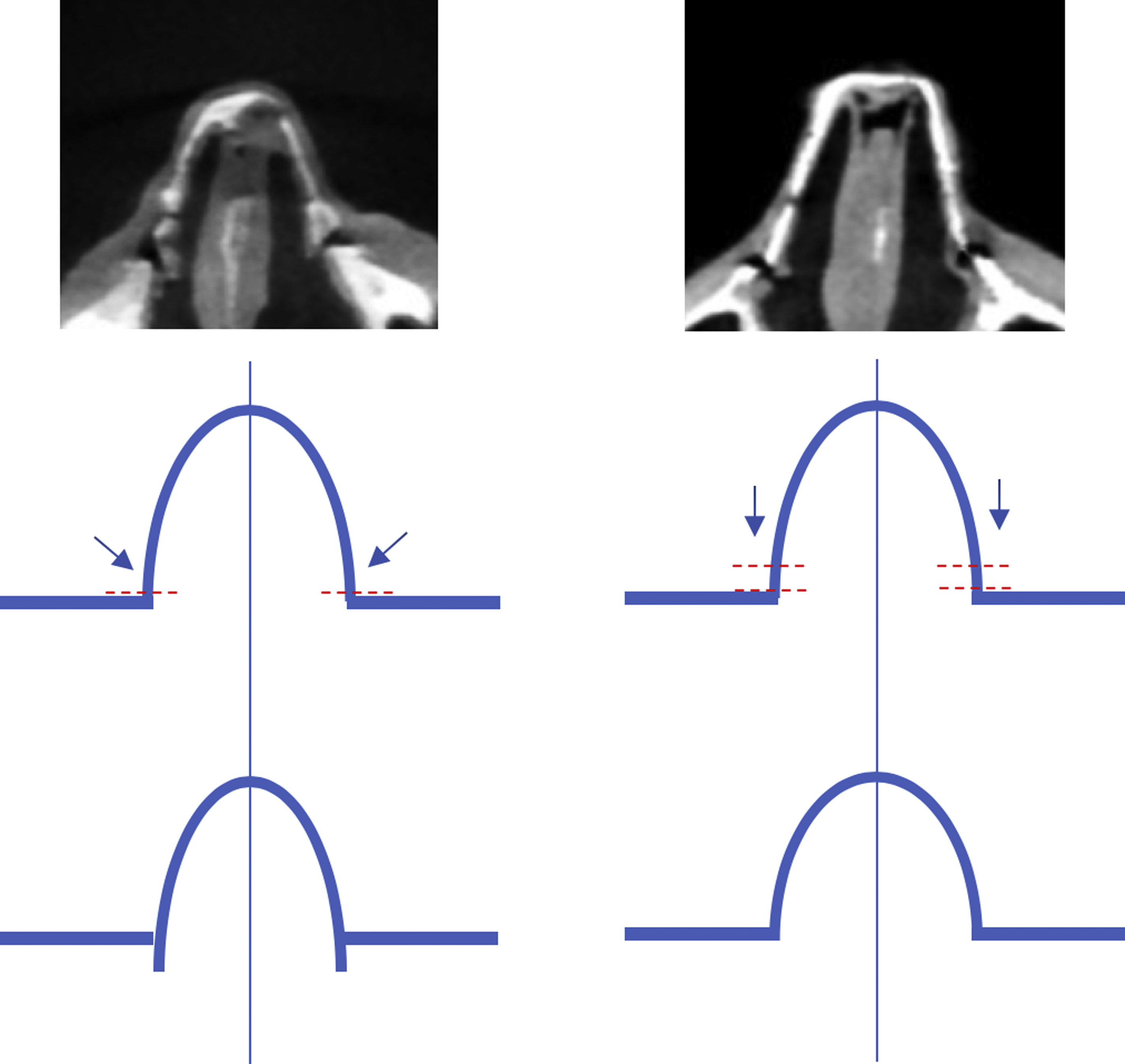
The bony pyramid in DP surgery can be managed using one of two strategies: the push-down (PD) or let-down (LD) operation. , , , In the PD technique, lateral and transverse osteotomies are performed to allow for mobilization of the entire bony vault. In the LD operation, similar osteotomies are performed, but a wedge of bone at the frontal process of the maxilla is also removed. After osteotomies in the PD technique, the lateral aspect of the bony pyramid is advanced into the nasal cavity medial to the frontal process of the maxilla ( Fig. 1 ). Theoretically, although the internal nasal valve angle is not directly disrupted with this technique, the medial movement of the bony vault could narrow the angle. In addition, when combined with the inferior descent of the pyramid into the nose, there may be a reduction in the cross-sectional area of the nose at this site. Alternatively, with the LD technique, because the nasal pyramid is not impacted within the nose and rather lowered to rest on the maxilla, there is a theoretically lower risk of narrowing the area of the internal nasal valve (see Fig. 1 ).
A recent cadaveric radiologic study from our group has examined the impact of DP (both LD and PD) and standard hump take down with autospreader reconstruction of the midvault on internal nasal valve dimensions. In the cadavers with conventional joseph hump take downs, the internal nasal valve angle decreased from a mean of 10.72 preoperatively to 9.98 postoperatively, although this difference only approached significance ( P = .068). The cross-sectional area at the level of the internal nasal valve did not significantly change (1.92–1.87; P = .156). In cadavers undergoing the PD procedure, both the internal nasal valve angle and cross-sectional area decreased (11.36–9.3 [ P = .016] and 1.89–1.59 [ P < .001], respectively). The LD group did not show significant reduction in the internal nasal valve angle or in cross-sectional area ( P = .437 and P = .331, respectively). As such, the LD procedure may be superior to the PD with regard to narrowing of the nasal passage. Whether this difference has clinical relevance for patients is an area of ongoing research and may have implications for the selective use of the LD over the PD technique. Moreover, it remains unclear if there are dynamic differences in narrowing of the internal nasal valve in addition to the static differences between dorsal hump reduction procedures elucidated in this study.
The placement of spreader grafts to widen a narrow internal nasal valve has not been described with DP techniques, although it is theoretically possible to place spreader grafts endonasally without release of the ULCs. Certain methods of DP, including the modified subdorsal strip method described elsewhere in this article, allow access to and release of the caudal upper lateral cartilage attachments. Therefore, the placement of spreader grafts is facilitated. This method allows for unilateral or bilateral widening of the internal nasal valve for functional or aesthetic purposes.
A cartilaginous DP surgery (termed spare roof technique by the authors), has also been described to impart benefits on the internal nasal valve. In this technique, the cartilaginous midvault is preserved with subdorsal resection of septal cartilage. However, an ostectomy of the caudal edge of the nasal bones is performed with subsequent need for lateral osteotomies to close an open roof. As such, this technique differs from DP techniques in which the entirety of the dorsum is preserved. However, in preserving the upper lateral cartilage attachments to the nasal septum, the internal nasal valve is importantly preserved. The authors suggest that this technique has functional benefits secondary to the widening effect on the midvault and internal nasal valve as the dorsum descends.
Nasal septum
In patients who present with a dorsal hump, the presence of a septal deviation may contribute to concomitant obstructive complaints. In addition, the septum provides support to the overlying nasal bone and upper lateral cartilages. Therefore, regardless of whether the LD or PD technique is used, descent of the dorsum requires excision of a portion of the septum. Several techniques to manage the septum have been described in DP surgery, each primarily differentiated by the location of septal cartilage excision. Although these techniques have been described in detail elsewhere, several differences that contribute to functional outcomes are briefly summarized here. ,
A subdorsal resection of cartilage originally described by Goodale and championed by Saban and associates, involves a strip of cartilage removed immediately under the dorsum. , , The resection extends to the anterior septal angle. , , A recently described modified subdorsal strip method performed by the senior author involves resection of a strip of cartilage high on the septum with the preservation of a 3- to 5-mm subdorsal strip of cartilage. Unlike other techniques, the resection terminates posterior to the anterior septal angle, and a 1.0 to 1.5 cm caudal strut of septal cartilage is maintained. A third method, described by Cottle, involves inferior cartilage excision along the maxillary crest. This is combined with a resection of a vertical 4 mm segment at the bony cartilaginous junction (from the keystone to the vomer) and a resection of the ethmoid bone under the nasal bone. Another method, described by Ishida and colleagues, involves excision of a strip of cartilage at the mid aspect of the cartilaginous septum.
Both the subdorsal technique and modified subdorsal strip method would allow for removal of any septal deviation in the mid or posterior aspects of the cartilaginous septum. This is because the excision of cartilage performed for descent of the nasal pyramid is higher up on the septum. As long as a strut of cartilage is maintained superiorly, portions of deviated septum inferiorly can be resected without disrupting nasal support. Alternatively, the Cottle and Loring method relies on resection of inferior cartilage and manipulation of cartilage along the entire bony–cartilaginous junction. This precludes the removal of any further cartilage. Similarly, midseptal resection of cartilage for the purposes of dorsal hump descent limits the amount of cartilage that can be removed inferiorly for the purposes of septal deviations without the risk of loss of nasal support. For these reasons, cartilage grafts for the purposes of providing lower lateral cartilage support can be harvested more easily in the subdorsal and modified subdorsal technique.
Although posterior septal deviations can be managed with standard endonasal septoplasty approaches, deviations of the anterocaudal septum pose unique structural challenges. A variety of repair techniques have been described to address deformities of the caudal septum in nonpreservation rhinoplasty cases, including swinging door, cartilage scoring, septal extension grafts, and septal batten grafts. , , These techniques are aimed at stabilizing or recontouring native cartilage and may be applied to DP rhinoplasty. This technique, however, must be undertaken with caution because the caudal aspect of the septum is already violated during excision of the cartilaginous strip needed for dorsal descent in the majority of techniques, and there is a risk of overweakening of the cartilage to occur (ie, if it is scored). In the Cottle technique, the anterior septum is disarticulated from the maxillary crest and excised inferiorly. As such, this method incorporates elements of the swinging door technique for correcting caudal deviations. The anterior septum can theoretically be positioned into the correct position in both the anterior–posterior and transverse dimensions. The caudal septum is tensioned to the anterior nasal spine and is critical to success of the dorsal reduction. If the caudal septum is severely deviated, weakening and scoring methods will weaken the critical structure of this type of rhinoplasty.
Even in cases of nonpreservation rhinoplasty, these techniques addressing septal caudal deviations can be variably effective because most depend on an inherently misshapen cartilage structure. Conventional extracorporeal septoplasty techniques that are used for extensive caudal septal deviations are difficult to perform with DP techniques given both the septal excisions performed for dorsal lowering and the need to maintain the keystone and the stability of septum to support the overlying nasal vault.
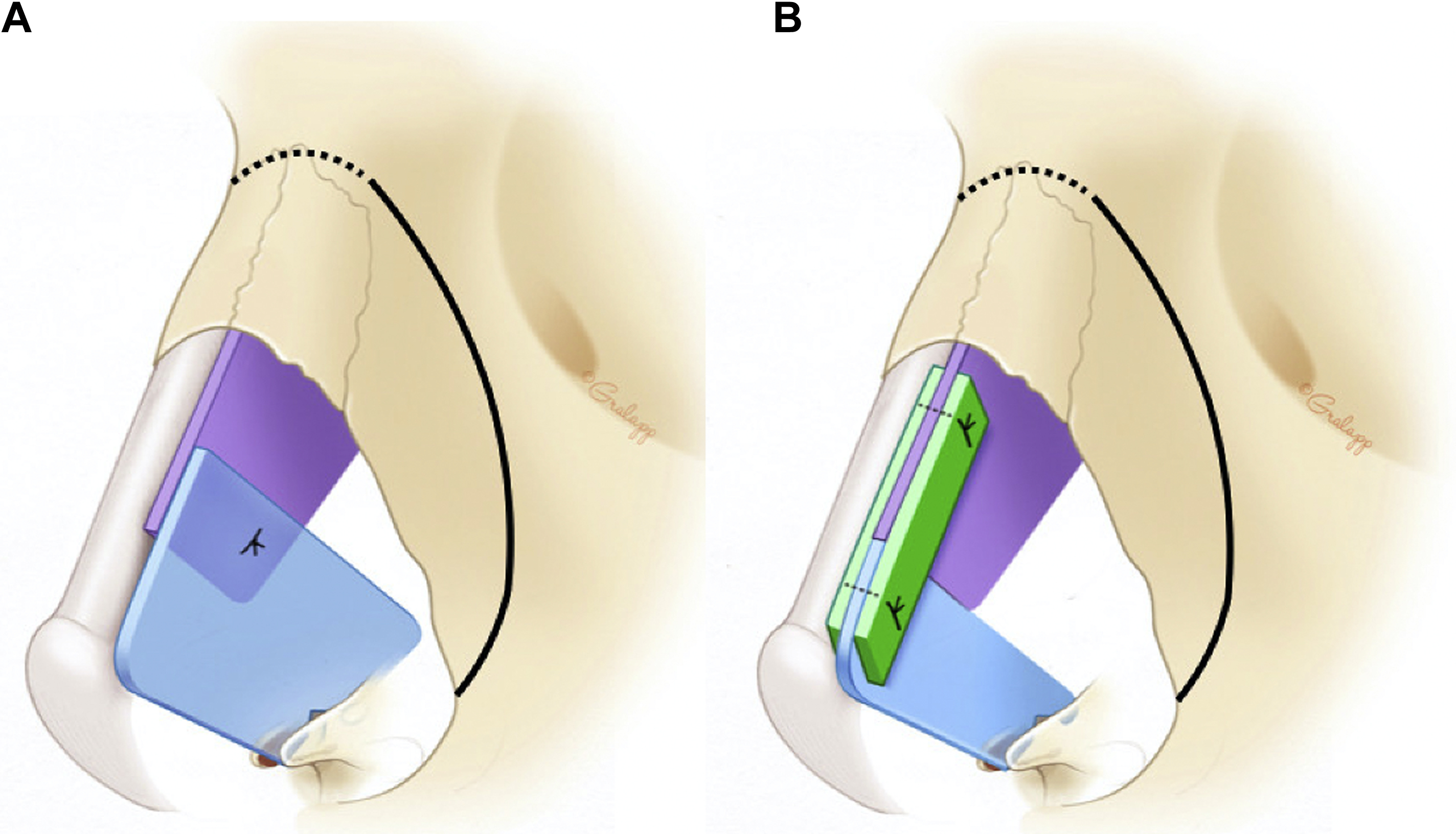
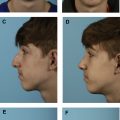
Subtotal septal reconstruction and the anterior septal reconstruction (ASR) techniques, both modifications of extracorporeal septoplasty, preserve the dorsal septum and thereby maintain the integrity of the keystone area. In the ASR method, the anterocaudal septal deviation is removed and a new caudal strut is reconstructed from either rib or septal cartilage. This strut is anchored to the remaining dorsal strut and placed into a groove in the nasal spine. The modified subdorsal strip method, by maintaining a strut of subdorsal cartilage, allows for the use of ASR in this particular DP method ( Fig. 2 ). In this technique, the ASR graft can be directly sutured to the dorsal strut in a side-to-side configuration (see Fig. 2 A) or it can be sutured in an end-to-end configuration (see Fig. 2 B). In the latter configuration, bilateral extended spreader grafts are used to stabilize the ASR graft. Notably, these spreader grafts differ from traditional spreader grafts because they do not sit between the native dorsal septum and the upper lateral cartilages (as the upper lateral cartilage attachment to the dorsal septum is preserved), but instead sit high along the remaining dorsal strut, just beneath the upper lateral cartilage. Fig. 3 demonstrates representative photographs of a patient undergoing an LD procedure with the modified subdorsal strip method technique combined with an ASR.
Related posts:
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 History of Dorsal Preservation Surgery
History of Dorsal Preservation Surgery
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


