There are 2 approaches for lowering the osseocartilaginous nasal dorsum. The most frequently used method includes resection of the osseocartilaginous nasal dorsum. The second method is based on preservation of the osseocartilaginous nasal dorsum. The concept of dorsal preservation surgery is to preserve, not resect, the nasal bones and upper lateral cartilage. Reduction rhinoplasty with preservation of the nasal dorsum is not only possible, but results in a natural appearing postoperative dorsal esthetic line. Thus, the rhetorical question: Why reconstruct the nasal dorsum when you can simply preserve it?
Key points
- •
Dorsal preservation surgery preserves the osseocartilaginous nasal dorsum, allowing reduction rhinoplasty without nasal dorsal (roof) resection; in the Joseph rhinoplasty, the osseocartilaginous nasal dorsum is regularly resected.
- •
Dorsal preservation surgery first appeared in the American literature over 100 years ago, described by Goodale (“push down” 1899) and Lothrop (“let down” 1914).
- •
The French contributed to dorsal preservation surgery with Sebileau and Dufourmentel (”let down” 1926) and Maurel (”push down” 1940).
- •
Fomon (1939) observed that previous surgeons, including Goodale, Lothrop, Eitner, and Dufourmentel were able to “correct the deformity without attacking the hump itself.”
- •
In 2018, Saban, Daniel, Polselli, Trapasso, and Palhazi published a reassessment of the push down technique (320 cases), heralding a reemergence or renaissance (rebirth) of dorsal preservation surgery.
Why bother reading history?
History is a living breathing access laboratory, an expedition into the human experience, delivering knowledge; affording evidence of the thoughts, contributions, and achievements of our predecessors; and providing perspective and insight as to our origins and the consequent contemporaneous state.
Today in corrective rhinoplasty, there are primarily 2 distinctive and disparate approaches for lowering the osseocartilaginous nasal dorsum (“hump”). The most frequently used method, described by Jacques Joseph ( Fig. 1 ) in 1898 and 1904, includes resection of the osseocartilaginous nasal dorsum. The second method is based on preservation of the osseocartilaginous nasal dorsum and was illuminated, advocated, and taught by Maurice Cottle in 1954 ( Fig. 2 ). Cottle labeled the procedure a “push down” operation. His surgical conception was elimination of the dorsal hump, not by resection but rather by downward displacement of the intact osseocartilaginous nasal pyramid with retention (preservation) of the anatomic and physiologic integrity of the nasal roof (vault, or osseocartilaginous nasal dorsum).

What is dorsal preservation surgery?
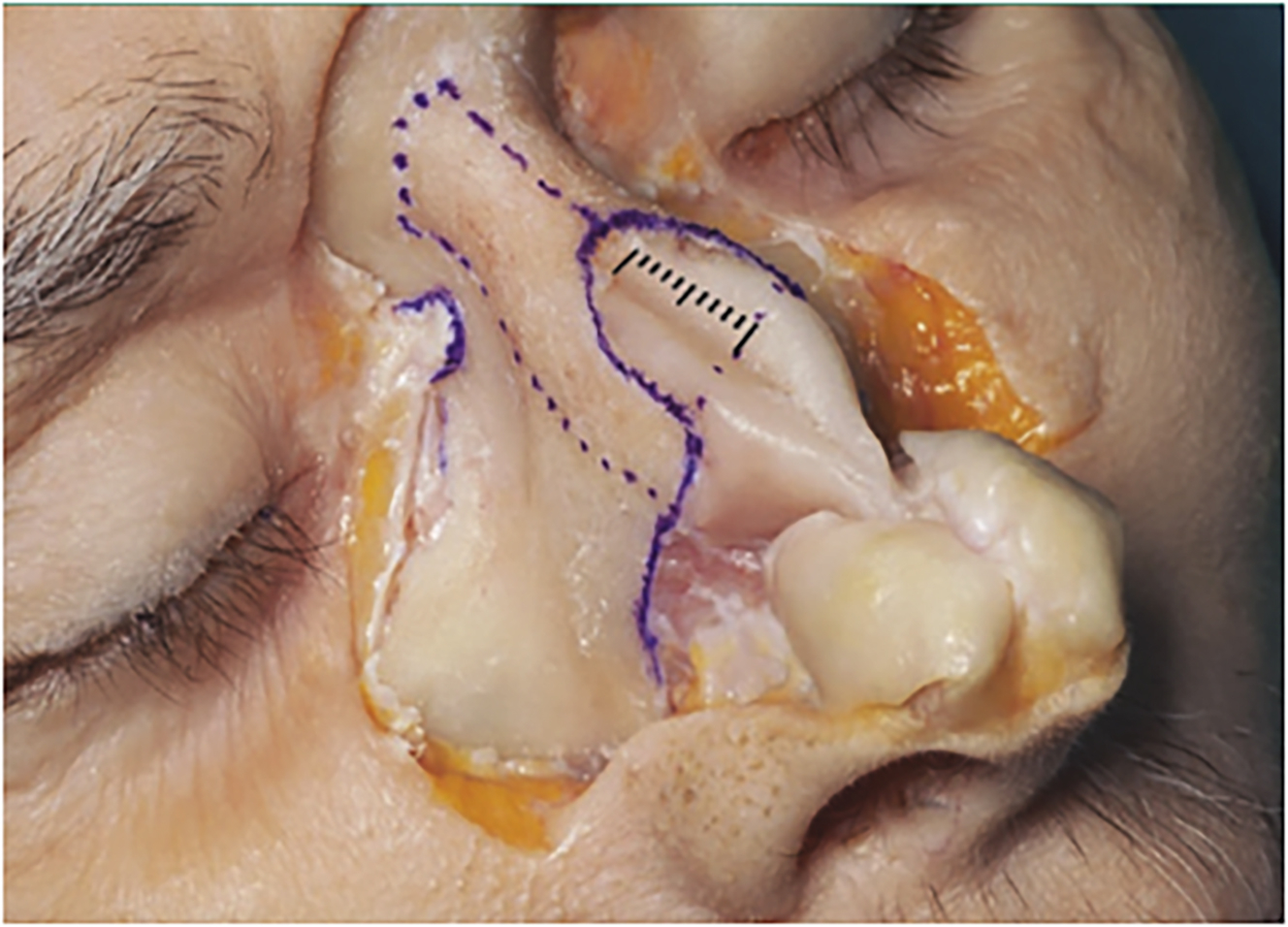
Dorsal preservation surgery preserves both the nasal bones and the upper lateral cartilage, thereby maintaining an intact osseocartilaginous nasal dorsum. Photographs of cadaver dissections in the masterwork text Rhinoplasty: An Anatomic and Clinical Atlas , by Rollin Daniel and Peter Palhazi, captures this anatomy beautifully ( Fig. 3 ).
Why dorsal preservation surgery?
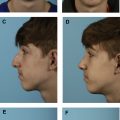
At a 2016 rhinoplasty meeting in Versailles, France, Daniel ( Fig. 4 ) suggested that surgeons reconsider the push down operation, alluding to the undesirable consequences of hump resection as practiced in the Joseph rhinoplasty. The Joseph rhinoplasty embraces the “en bloc” removal (resection) of a portion of the nasal bones, along with portions of the upper lateral cartilage and nasal septum, which can result in the following postoperative consequences:
- 1.
Dorsal esthetic irregularities (the “operated look”).
- 2.
Neurogenic pain syndromes secondary to an “open roof” deformity. a
a The “open roof” deformity is defined as follows: when the nasal dorsum (osseocartilaginous roof) is removed, and remains unclosed (dehiscent) so that the underlying nasal mucosa contacts the under surface of the overlying dorsal nasal skin which may result in pain symptoms.
- 3.
Breathing dysfunction secondary to a narrowed nasal airway, especially in the critical internal nasal valve area.

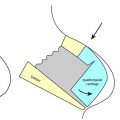
With dorsal preservation surgery, a term coined by Daniel, it is possible to preserve the osseocartilaginous nasal dorsum, including the “K-area.” The K-area refers to the keystone, or bedrock region of the nose, where the distal end of the nasal bones and the cephalic end of the upper lateral cartilage joins the underlying perpendicular plate of the ethmoid and the quadrangular (septal) cartilage.
The result is a more natural postoperative dorsal esthetic line that does not require the obligatory midvault reconstruction with spreader grafts or spreader flaps.
Two methods of dorsal preservation surgery: the push down and let down
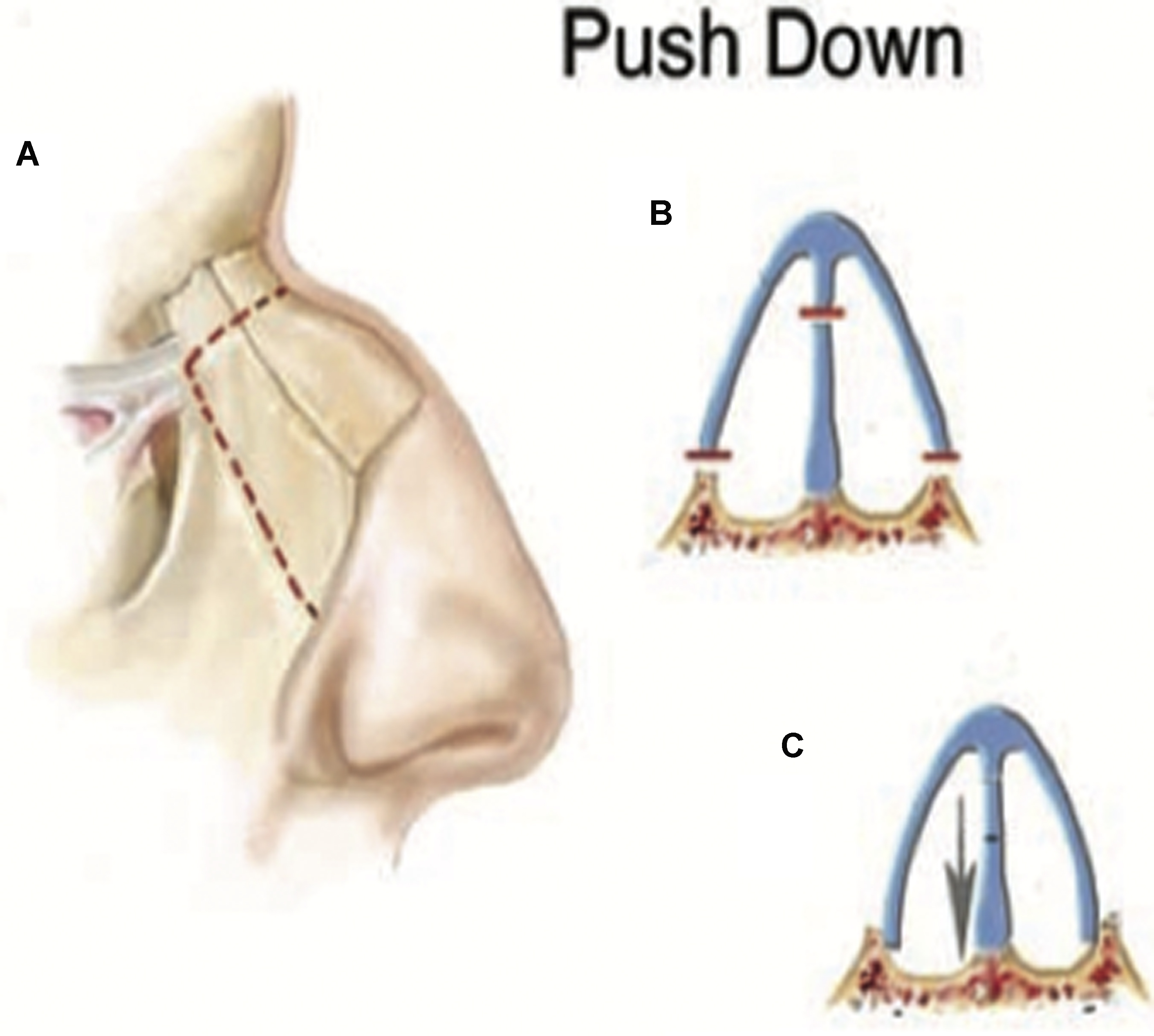
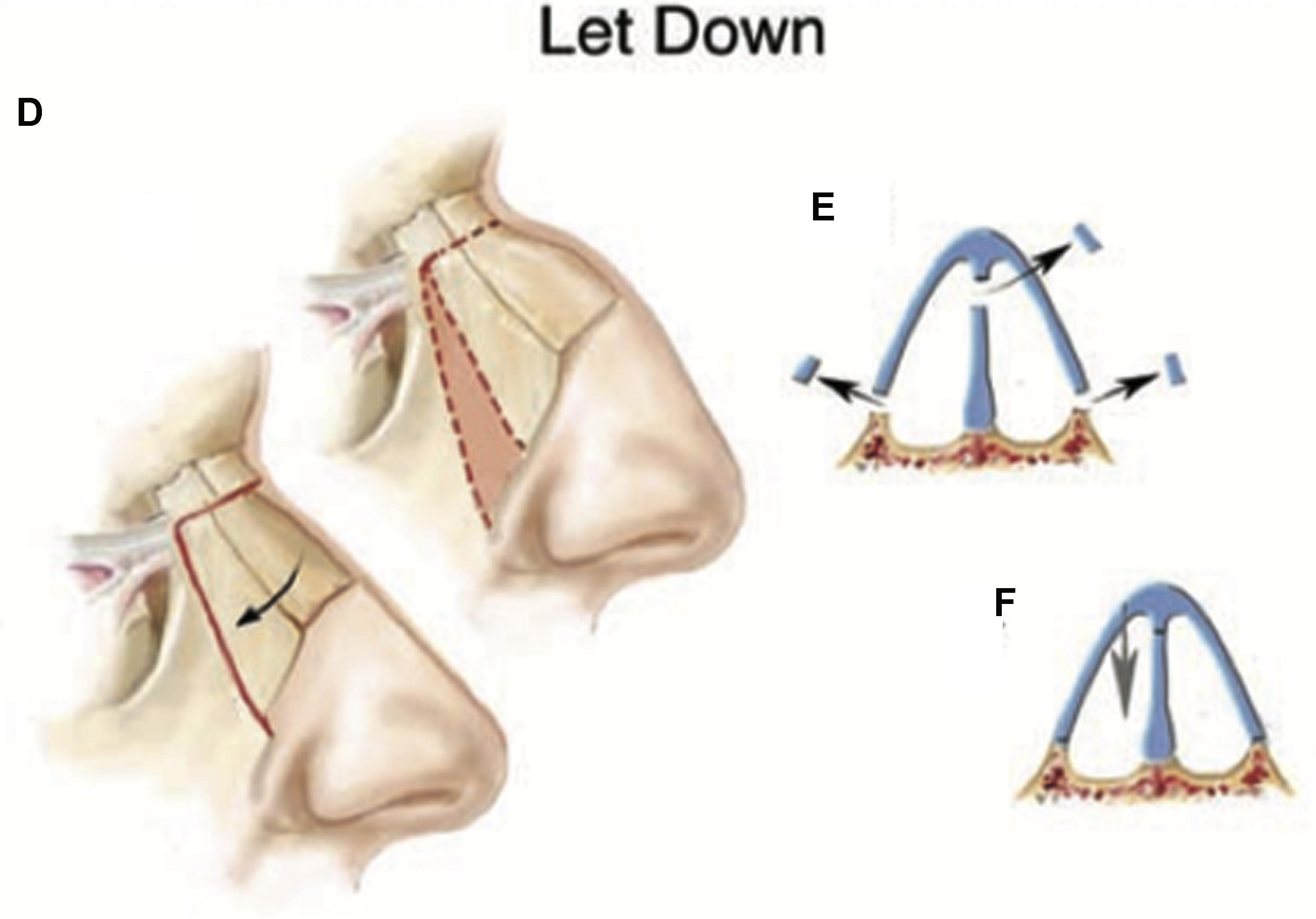
In 2018, Saban and colleagues ( Fig. 5 ) published “Dorsal Preservation: The Push Down Technique Reassessed,” the senior author and surgeon reviewed 740 septo-rhinoplasties performed, over 5 years, in which 320 clinical cases of dorsal preservation surgery occurred. There were 286 females to 34 males. The mean follow-up was 2 years and 5 months (range, 6 months to 5.5 years) amid a revision rate of 3.4% (11/320). Using the endonasal approach, a strip of septal cartilage is removed from the subdorsal region. This step is followed by complete lateral and transverse osteotomies at the radix, thereby achieving a dorsal reduction by either a push down operation or a let down operation. The push down operation consists of downward impaction of the fully mobilized osseocartilaginous nasal dorsum into the pyriform aperture and is used in patients with humps of less than 4 mm ( Fig. 6 ). The “let down” entails resection of a “maxillary wedge” from the ascending (frontal) process of the maxilla, along with some septal resection and is implemented in patients requiring more than 4 mm of dorsal reduction ( Fig. 7 ). Saban and colleagues clearly presented the difference between these operations:
- 1.
” Push down ”
- a.
Septal phase: strip cartilage excision; after Saban and associates, a high subdorsal resection (excision) of septal cartilage; after Cottle, a low septal resection (excision) of septal cartilage; Cottle’s “inferior strip” removal of septal cartilage.
- b.
Bone phase: lateral and transverse osteotomies, then the bony and cartilaginous dorsum is depressed downward (“pushed down”) into the pyriform aperture.
- a.
- 2.
” Let down ”
- a.
Septal phase: strip cartilage excision; after Saban and colleagues, a high subdorsal resection (excision) of septal cartilage; after Cottle, a low septal resection (excision) of septal cartilage; Cottle’s “inferior strip” removal of septal cartilage.
- b.
Bone phase: resection of a portion maxillary wedge of the ascending (frontal) process of the maxilla followed by transverse osteotomies; next the bony and cartilaginous dorsum is depressed downward (let down) onto the ascending (frontal) process of the maxilla.
- a.

Seeking the godfather(s) of dorsal preservation surgery
A godfather is additionally defined as a pioneer, a person who is influential in a specific movement or organization. Because I trained in otorhinolaryngology at the Mayo Clinic Graduate School of Medicine in Rochester, Minnesota, from 1964 to 1968, my teachers included Clifford Lake, MD ( Fig. 8 ) of Mayo Clinic in Rochester, Minnesota, and Pat Barelli, MD ( Fig. 9 ) of Kansas City, Missouri, and both surgeons taught the push down operation; each were professors at the “Cottle Courses” and proficient practitioners of the Cottle push down. My friend and colleague at Mayo Clinic is the accomplished and skillful surgeon George W. Facer, MD ( Fig. 10 ). We both first attended and later taught at the Cottle Courses and cochaired the Mayo Clinic Rhinologic Surgical Courses on alternate years for 30 years; each of us personally trained more than 120 otorhinolaryngology residents at Mayo, from 1970 to 2003, in both the push down and let down operations. Until quite recently, it was believed, by this author (E.B.K.), that dorsal preservation surgery embodied in the push down operation was first presented to the profession by Cottle in 1954. This misapprehension was corrected and clarified while preparing a talk on the history of dorsal preservation surgery for the Preservation Rhinoplasty meeting in Nice, France, in February 2019. Astonishingly, dorsal preservation surgery is an old idea, published more than 100 years ago in the American literature and more than 90 years ago in the French literature.


For the record, in 1887, John Orlando Roe, MD, of Rochester, New York, was undoubtedly the first to publish a cosmetic surgical procedure of the nasal tip. In 1891, he reported a cosmetic correction of an angular deformity of the nasal dorsum using bone scissors for the reduction of a dorsal deformity without septal surgery or osteotomies in 3 patients.
In the mission to accurately discover the godfathers of dorsal preservation surgery, the journey stretched back in time and place to nineteenth-century Boston, Massachusetts.
J.L. Goodale
The contributions of Roe , aside, the first ”push down” operation and the first article on dorsal preservation appeared in the Boston Medical and Surgical Journal 1899 authored by J.L. Goodale, MD ( Fig. 11 ). At that time, neither dorsal preservation surgery nor the ”push down” operation was part of the lexicon. Goodale, an assistant physician for diseases of the throat in the Massachusetts General Hospital and in the Boston Children’s Hospital, described a case of dorsal preservation surgery on June 21, 1898, on a 13-year-old girl, incorporating photographs. The description of the operation was read on October 12, 1898, at the Middlesex South District Medical Society and published in 1899 ( Figs. 12 and 13 ). Goodale’s operation was conceptually a ”push down”. The septal phase used 2 scissor cuts: first a curved scissors convex side uppermost and then a lower cut with a straight scissor. Both cuts were transmucosal as septal flaps were not raised.
A small saw was introduced teeth uppermost into the left nasal passage and the articulation of the nasal and maxillary bones sawn through from below upwards. A similar saw cut was made on the corresponding articulation on the right side. The nasal bones were thus left articulating with the frontal bone and with each other. A few comparatively gentle taps upon the nasal bones sufficed to break the frontal articulation and depress them, still firmly united with each other, until they came into contact with the upper margin of the septum. With the depression of the nasal bones, the bridge of the nose assumed a straight line from tip to forehead, but a ridge at the same time appeared on either side, formed by the maxillary bone along the lines of the nasal articulation. As determined by me previously in experiments on the cadaver, two or three light blows with a protected mallet upon this ridge fractured the maxillary bone, which is here very thin, along a line situated about 1 cm outside the nasal articulation and parallel to it, with the result of depressing the ridge and producing a perfectly smooth and even cutaneous surface. The operation occupied about 40 minutes and was attended by comparatively slight hemorrhage.
Related posts:
 Preservation Rhinoplasty
Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Modified Skoog Method for Hump Reduction
Modified Skoog Method for Hump Reduction
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


