Preservation rhinoplasty may refer to preserving several anatomic components including: the nasal bones, upper lateral cartilages, the keystone area and/or ligaments of the nose. Preserving the osseocartilaginous framework or “dorsal preservation” minimizes or completely avoids violation of the dorsal aesthetic lines’ architecture. Conventional hump reduction in open rhinoplasty disrupts these lines; however, it also provides versatility to reshape the entire dorsum. Surgical success with either technique requires a thorough understanding of the underlying nasal anatomy.
Key points
- •
Preservation and conventional rhinoplasty techniques require a thorough understanding of the surface and soft tissue nasal anatomy, and its integration with the underlying osseocartilaginous framework.
- •
Preservation of the keystone area (divided into a dorsal and lateral components) contributes to the continuity of the dorsal aesthetic lines.
- •
For more in-depth description, the reader is referred to the primary literature referenced herein.
Introduction
A hallmark of rhinoplasty is the maintenance of anatomic and structural components of the nose, while still allowing for changes in the external contour. Although preservation rhinoplasty has been advocated and performed by expert surgeons around the world, open structural approaches with Joseph or conventional hump reduction techniques have predominated rhinoplasty teaching and practice. Recently, there has been increased interest in the preservation rhinoplasty concept, particularly as the anatomic knowledge of the nasal skeleton and soft tissue envelope (STE) has been explained further by anatomists and experts such as Palhazi, Daniel, and Saban. , Preservation rhinoplasty may refer to several elements including (1) elevation of the STE in a subperichondrial–subperiosteal plane, (2) preservation of alar cartilages while minimizing excision. and (3) maintaining the bony/cartilaginous dorsum without violation of the osseocartilaginous interface. , The latter of these, or dorsal preservation rhinoplasty (DPR), can be performed with or without the other. Although conventional hump resection (CHR) or the traditional method described by Joseph disrupt the dorsal aesthetic lines (DALs), these methods provide versatility to reshape the entire dorsal architecture. Surgical success with either DPR or CHR techniques requires a thorough understanding of external and underlying nasal anatomy, particularly the dorsal hump. In this article, essential elements of nasal anatomy as they pertain to DPR and CHR are discussed.
Surface and soft tissue anatomy
An initial assessment of the nose involves an analysis of its relationship with other facial landmarks on different views ( Fig. 1 ). On the frontal view, the ratio of the length of the nose to the middle third of the face is 0.9:1.0. The width of the nasal root to the alar width is 0.5:1.0. The ratio of nasal projection on profile view to nasal length is 0.4:1.0, and the tip length is nearly 45% of the projection. , When a line is drawn from the deepest aspect of the nasal root at the nasion, to the appropriately projected nasal tip, the dorsum should lie at or just posterior and parallel to this line.
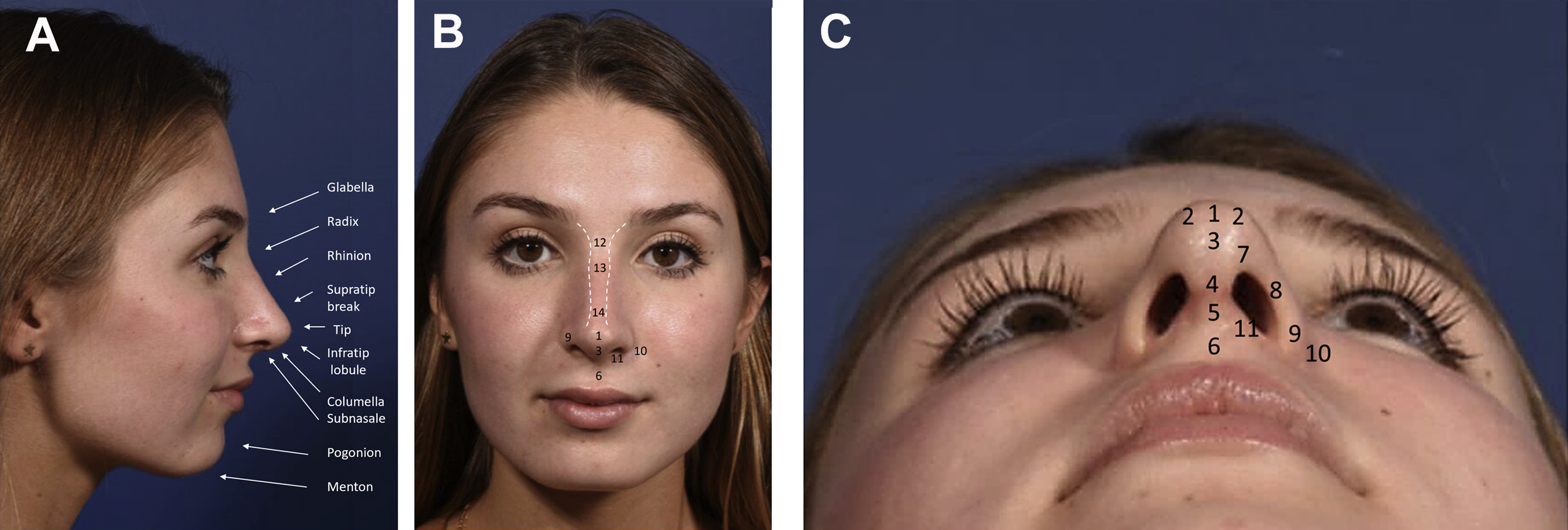
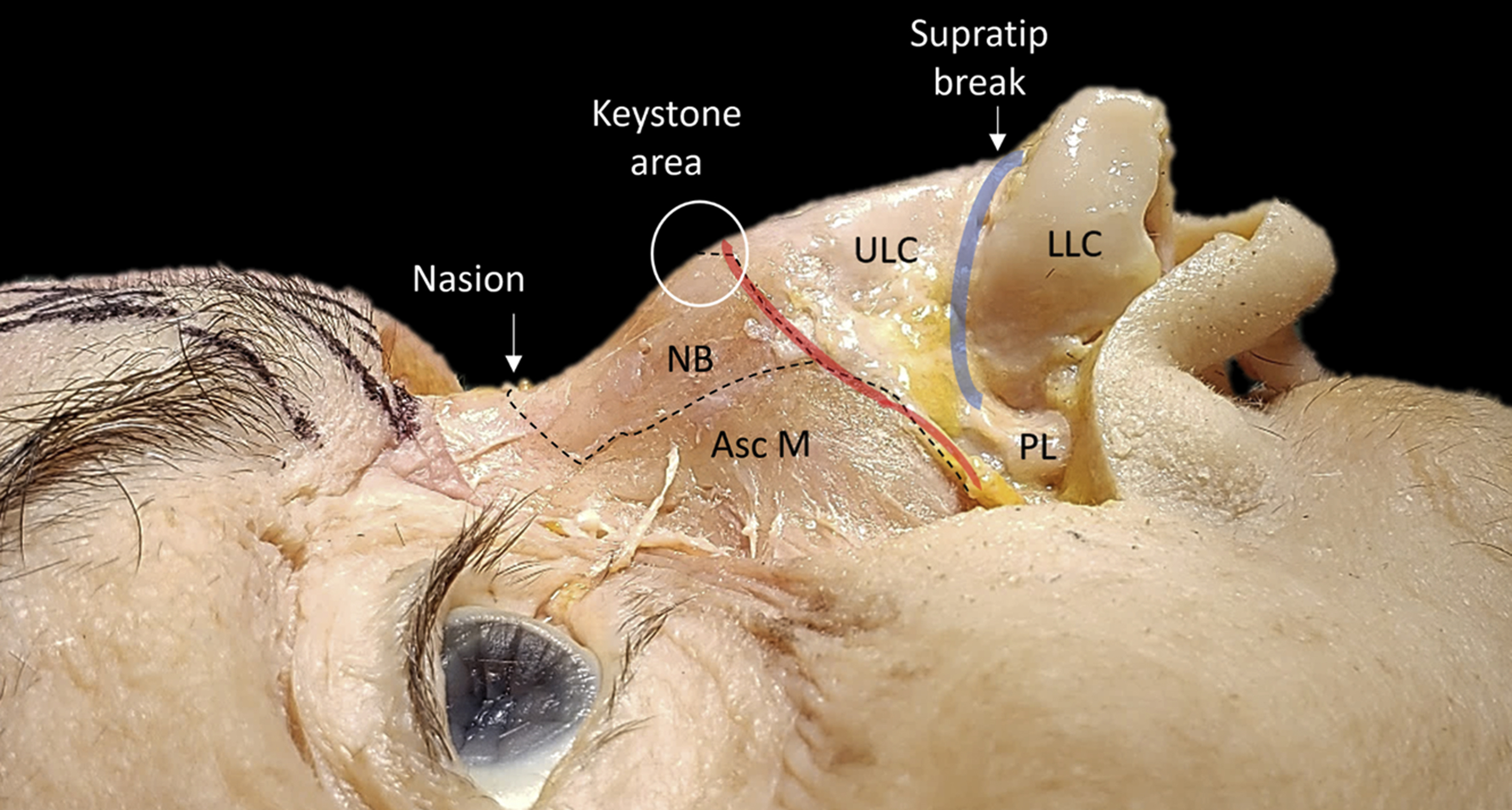
The nasal pyramid can be subdivided topographically into surgical thirds ( Figs. 2 and 3 ). The upper third is composed of a pair of nasal bones and the middle third is formed by the paired upper lateral cartilages (ULCs) that are responsible for forming the midvault and the internal nasal valves (INV). The nasal keystone area refers to the underlying junction between the upper and middle thirds of the nose , ; thus, a dorsal hump has contribution from both bone and cartilage (see Fig. 3 ). The lower third of the nose consists of the tip, soft tissue triangles, alar lobule, and columella, all of which are related to the shape and orientation of the lower lateral cartilages (LLCs).
Anatomic description of the STE mirrors layers of the face: dermis, superficial areolar (fatty) layer, superficial muscular aponeurotic system (SMAS) layer, deep areolar layer, and perichondrium/periosteum. Dissection in rhinoplasty can be performed in a subcutaneous, sub-SMAS, or subperichondral plane. , , In DPR, subperichondral dissection has been advocated. In open structural approaches or CHR techniques, a similar dissection can also be performed although many surgeons ultimately dissect in the sub-SMAS plane. It remains unclear if dissection in the sub-SMAS plane is aesthetically or functionally inferior to a subperichondrial plane of dissection, although there is theoretically less disruption of ligamentous nasal structures that are discussed elsewhere in this article and potentially less soft tissue edema.
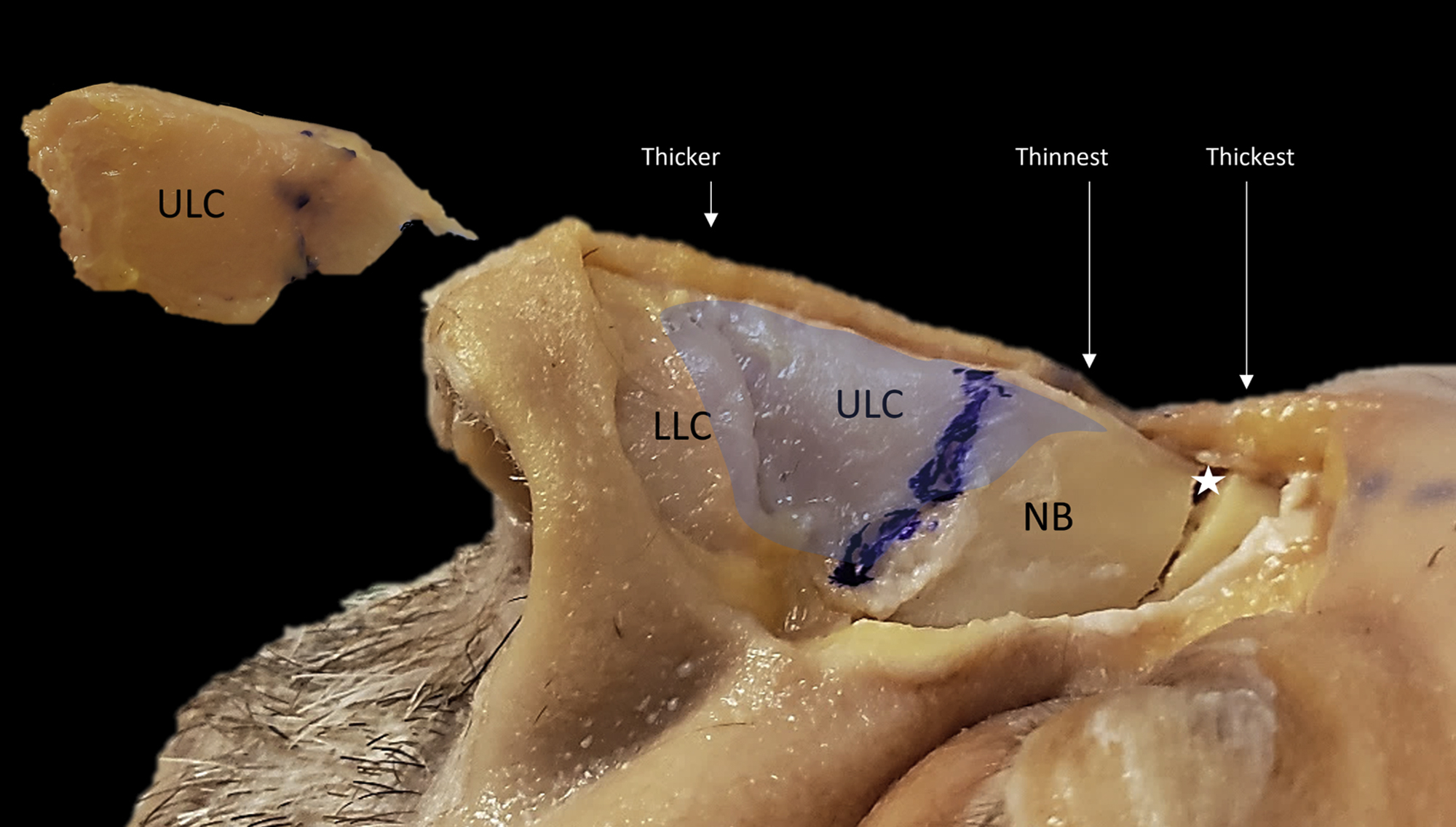
The STE varies in thickness among ethnicities and along the length of the dorsum (see Fig. 2 ), with an average of 1.25 mm at the radix and thinnest at the rhinion at 0.6 mm. There is greater mobility of the STE over the upper two-thirds than the lower third of the nose because of less adherence of the SMAS to the perichondrium, and more abundance in sebaceous and sweat glands in the lower third. In DPR, the thickness of the STE at the radix allows for the camouflage of any underlying stop-off after a transverse osteotomy (see Fig. 2 ). Because the STE is thinnest at the rhinion, irregularities can appear with the CHR, whereas the DPR has the benefit of minimal disruption to the dorsum at this site. In addition, in CHR techniques, as discussed elsewhere in this article, leaving the rhinion slightly more pronounced needs to be considered to compensate for differential skin thickness.
Dorsal aesthetic lines
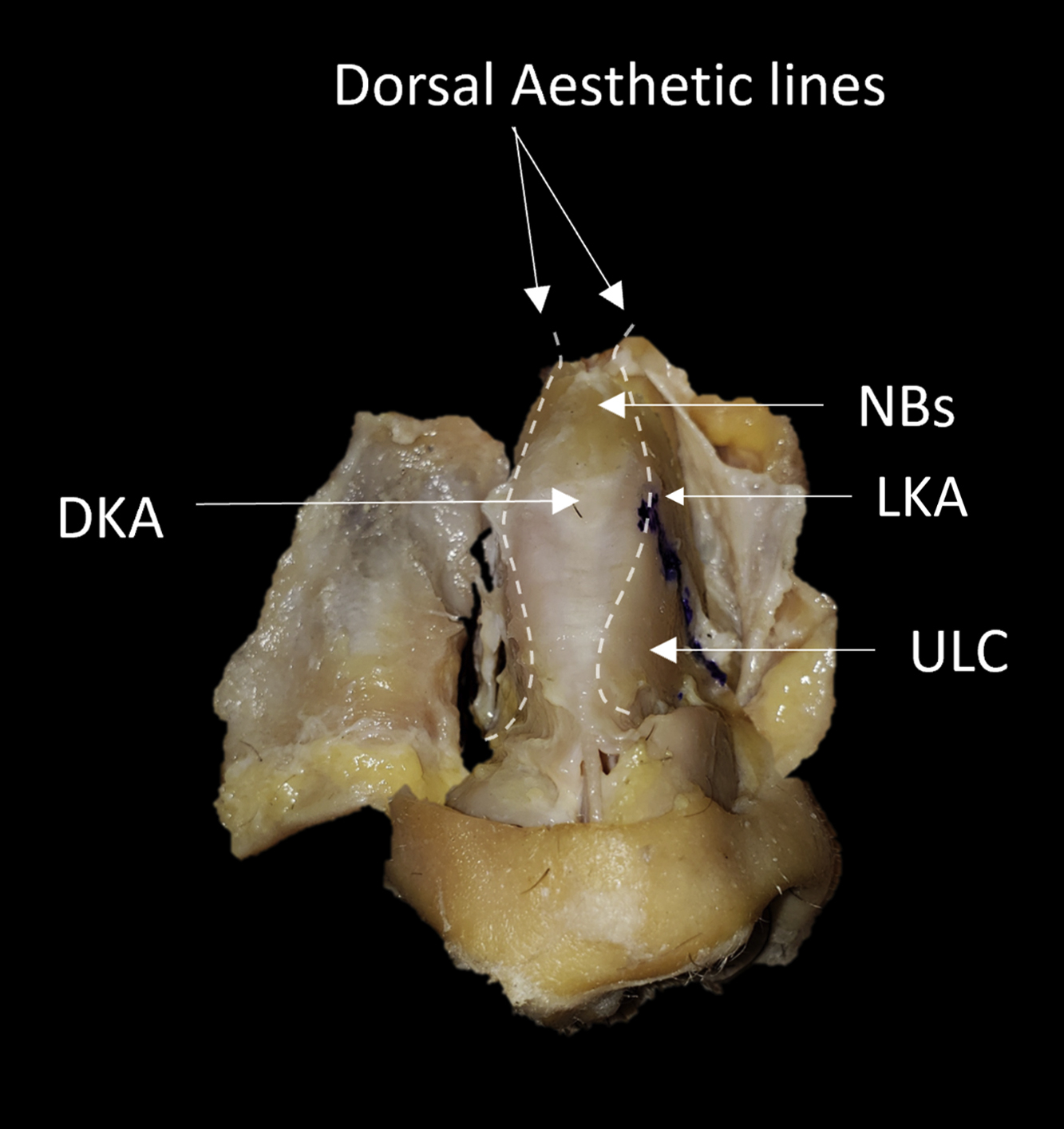
On the frontal view, 2 concave divergent reflection lines are seen extending from the orbital rim to the tip where they become slightly divergent again (see Fig. 1 C). These reflections are formed as a result of the contours of the underlying nasal osseocartilaginous structures. Conventionally, these lines were thought to be narrowest at the keystone area. However, it has been proposed that these lines are instead fusiform, being narrowest at the radix, wider at the keystone, and again narrow at the supratip. This widening at the keystone area corresponds with the caudal flare of the nasal bones and is relatively higher in males. The anatomic contributions to the DALs include the curvature at the junction between the dorsal and lateral aspects of the nasal bones in addition to the architecture of the underlying ULCs ( Fig. 4 ). In CHR, DALs are violated, requiring meticulous care restoring their continuity and symmetry; however, it provides the surgeon with freedom to reshape these lines when asymmetric or broken as in severe or S-shaped deviations. In DPR, these lines are preserved providing a natural dorsal architecture, provided they are desirable.
Nasal bones
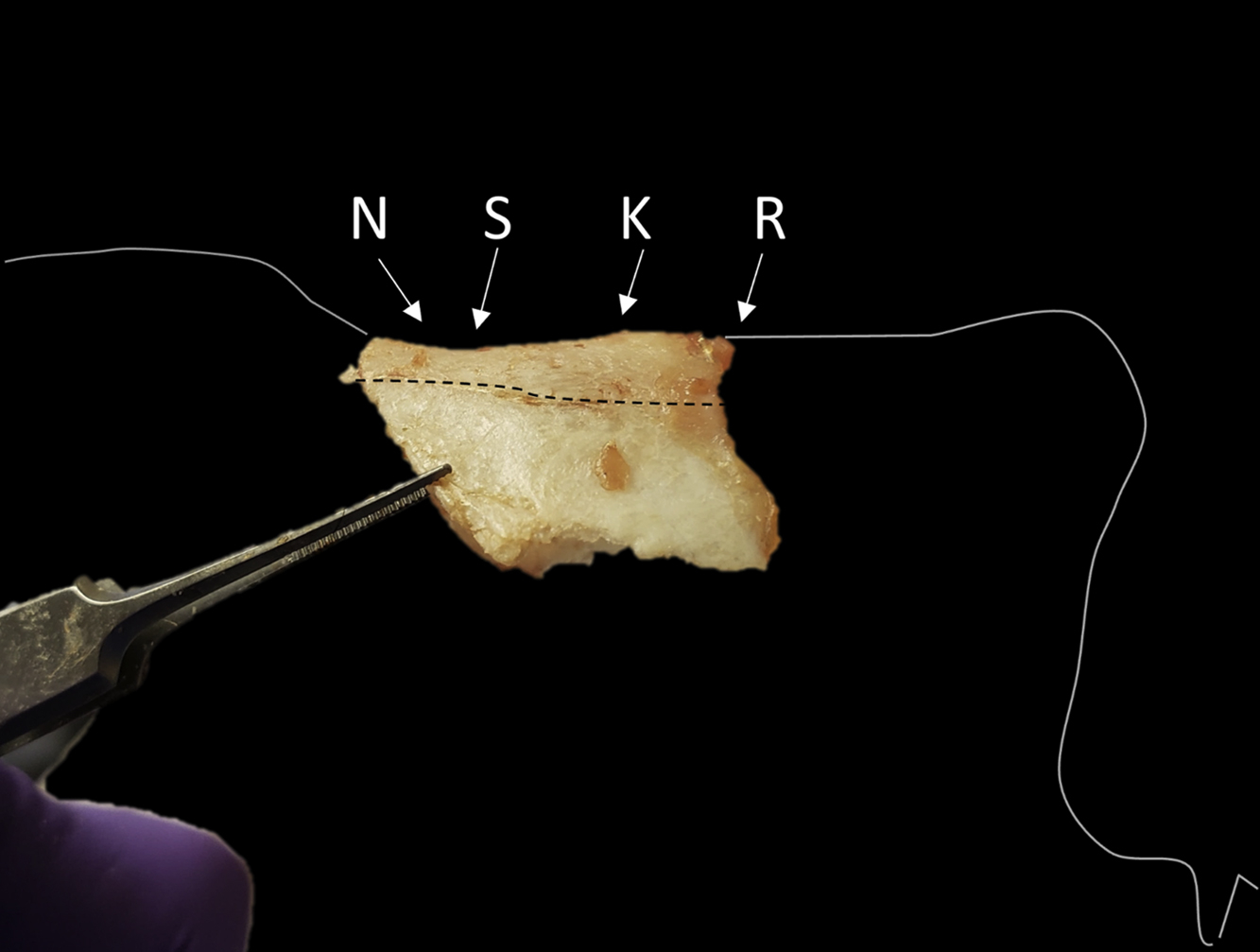
The nasal bones’ cephalic attachment to the frontal bones corresponds topographically with the radix or nasal root, forming the upper limit of the nasal height. The radix angle is obtuse with variations in values and position with gender; in males it tends to lie at the level of the superior tarsal crease and is less obtuse, whereas in females it is at the level of the upper lashes. The nasal bones on a profile view demonstrate 4 main points ( Fig. 5 ):
- 1.
The nasion: midpoint of the nasofrontal suture line.
- 2.
The sellion: deepest depression of the nasal bones and is used in pretreatment plans.
- 3.
The kyphion: most prominent point of the bony dorsum.
- 4.
The rhinion: most caudal point of the nasal bones and marks the midpoint of the osseocartilaginous vault.
These points have led to dividing the bony dorsum into 2 configurations:
- 1.
S-shaped nasal bones have a curve which begins at the sellion, with an apex at the kyphion, and plateaus at the rhinion (see Fig. 5 ).
- 2.
V-shaped nasal bones have a nearly straight configuration from the sellion through the rhinion and thus one locus of angulation at the sellion ( Fig. 6 ).
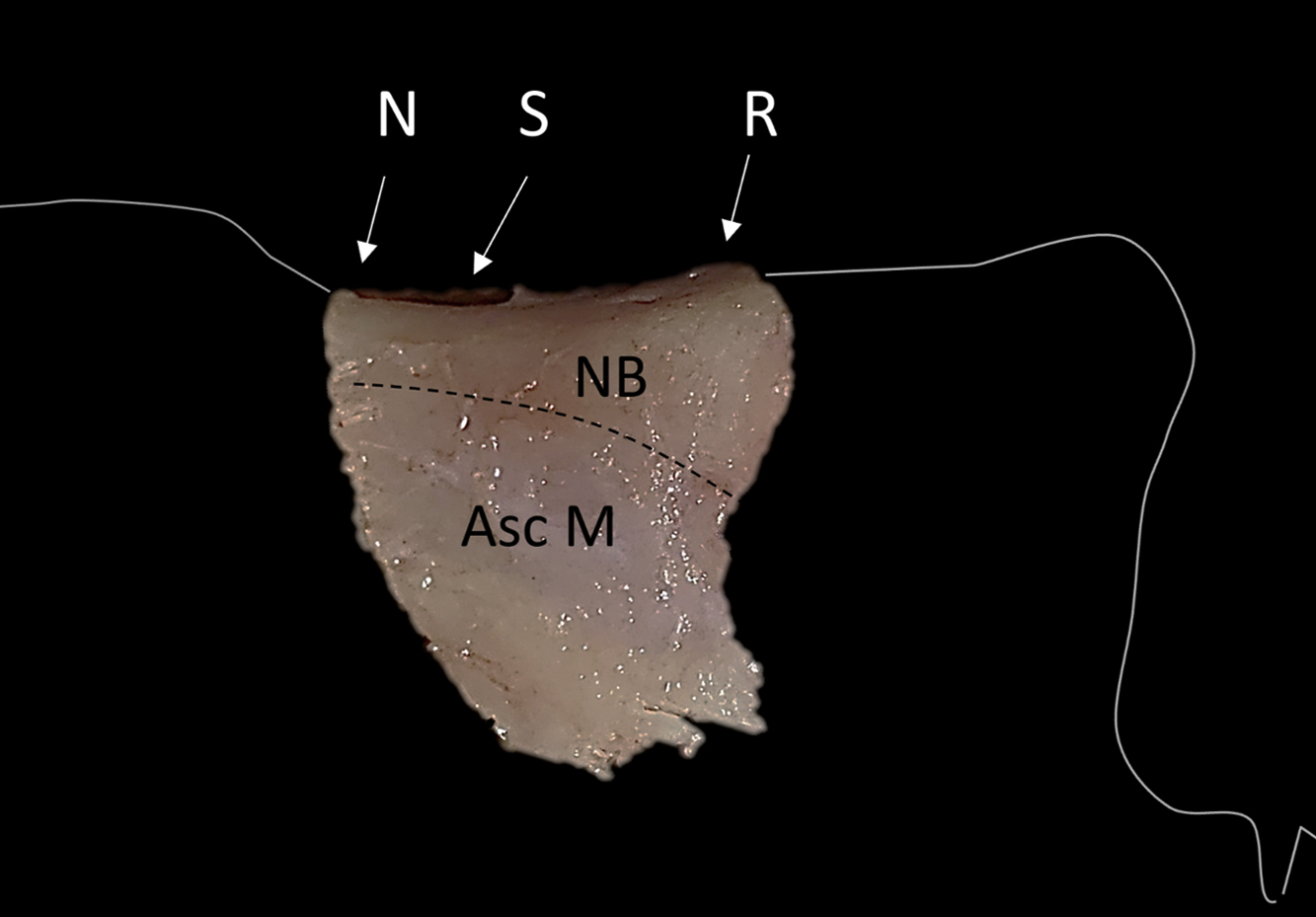
Fig. 6
Example of V-shaped bony hump. This type lacks kyphion prominence. Asc M, ascending process of the maxilla; N, nasion; NB, nasal bones; R, rhinion; S, syllion.
In DPR, as the nasal vault is pushed inferiorly, the kyphion is not resected, and therefore patients with S-shaped nasal bones may be at higher risk of a residual hump. In CHR, the kyphion is removed, thereby minimizing this risk. In nonpreservation hump removal, dorsal reduction can be performed in either a component or composite (en bloc) resection. The original description by Joseph was a composite resection, yet with evolution toward more conservative techniques, component resection has gained popularity. Although the latter procedure is time consuming, it allows more gradual reduction and thereby precise control over the bony dorsum reduced. Importantly, it allows for preservation of structures when possible and decreases chances of an open roof deformity with every dorsal reduction. With the thinning of the bone at the rhinion, and extension of ULCs under the nasal bones, when the bony cap is removed, it is possible to preserve the underlying cartilage if dorsal reduction is done gradually in a component rather than in a composite fashion.
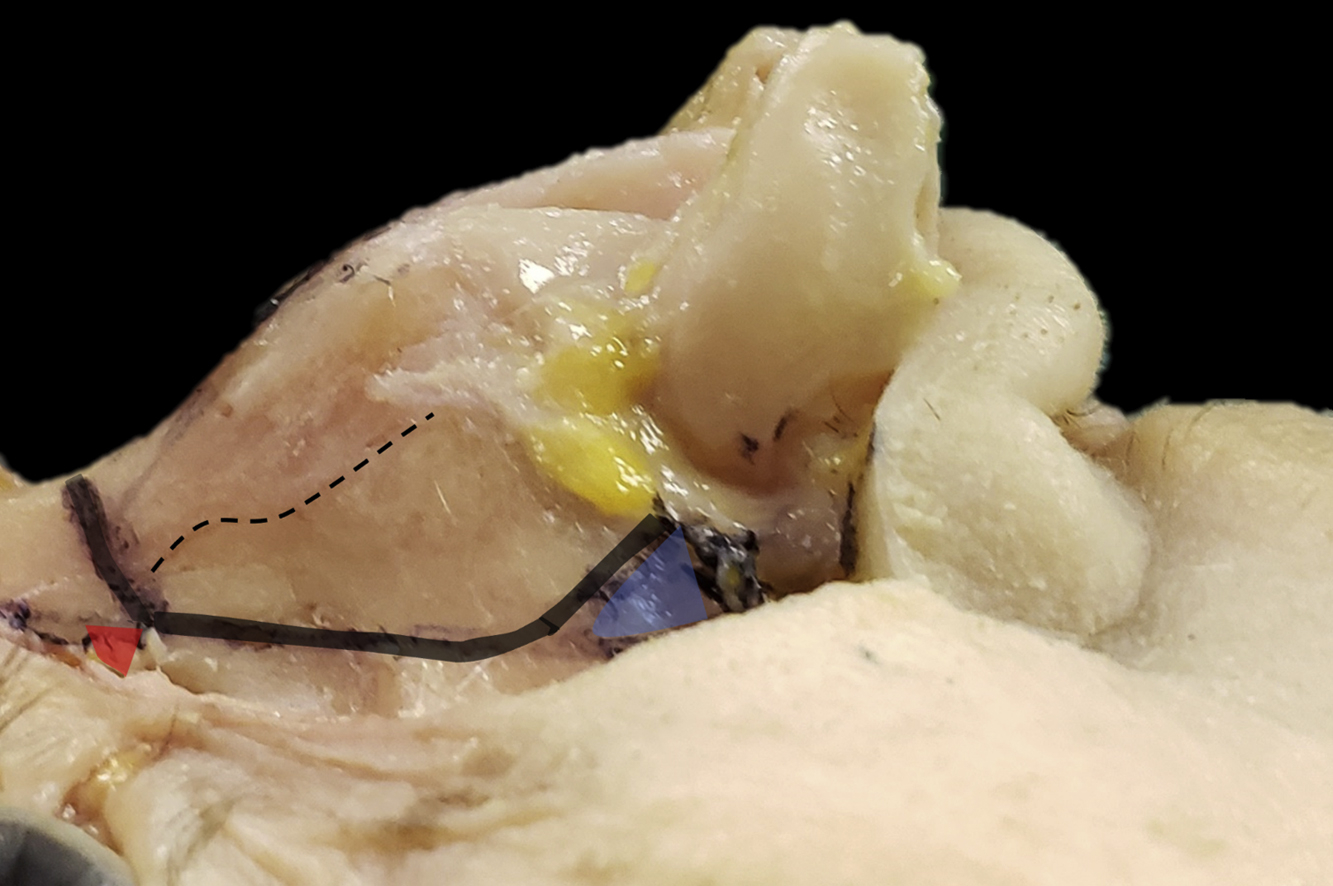
Nasal bones attach to the ascending maxillary processes that hosts the attachment of the medial canthal ligament. Lateral osteotomies in (push-down or CHR) or lateral wedge resection (in let-down procedures) should be placed such that the medial canthal ligament is preserved ( Fig. 7 ). In DPR, a transverse osteotomy across the dorsum connects the 2 lateral osteotomies. The level of the transverse osteotomy determines the starting cephalic point for the hump reduction. In CHR, the starting point of the nose is determined directly by where the reduction terminates. In subjects with convexity at the nasofrontal junction (shallow radix), the use of a curved radix rasp can help to reduce the nasal bone at this site, determining the start point of hump reduction.
The keystone area (dorsal keystone area and lateral keystone area)
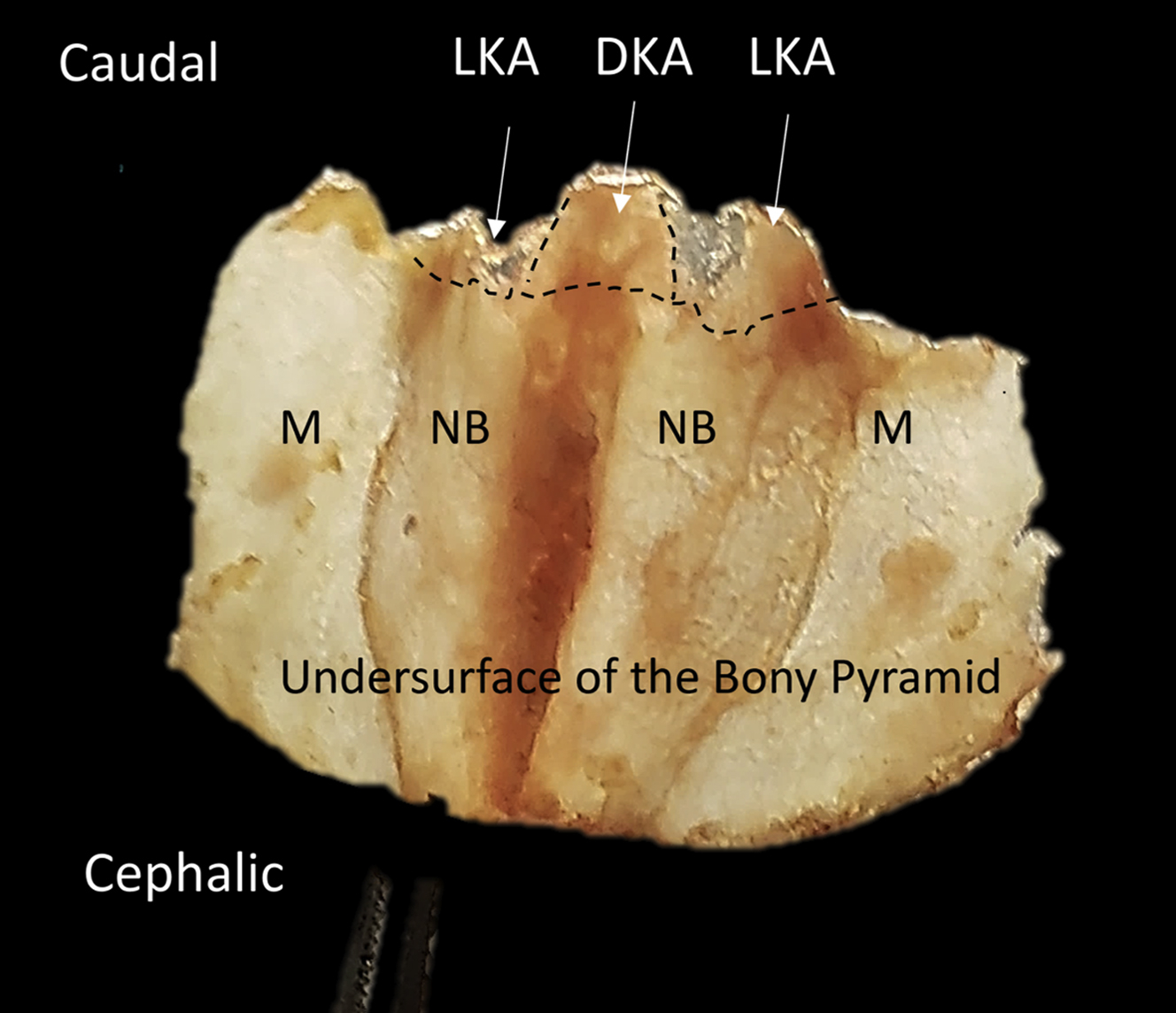
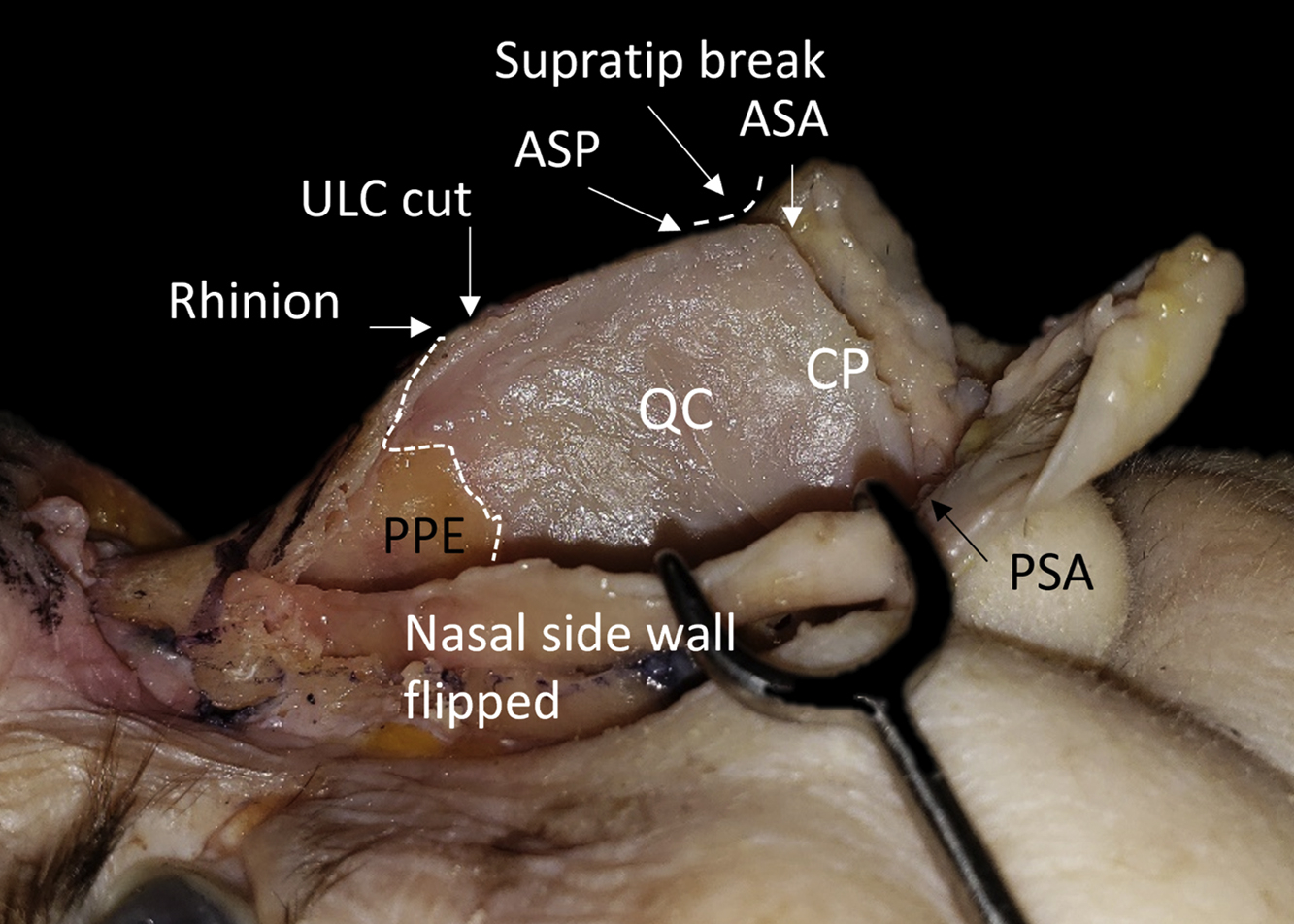
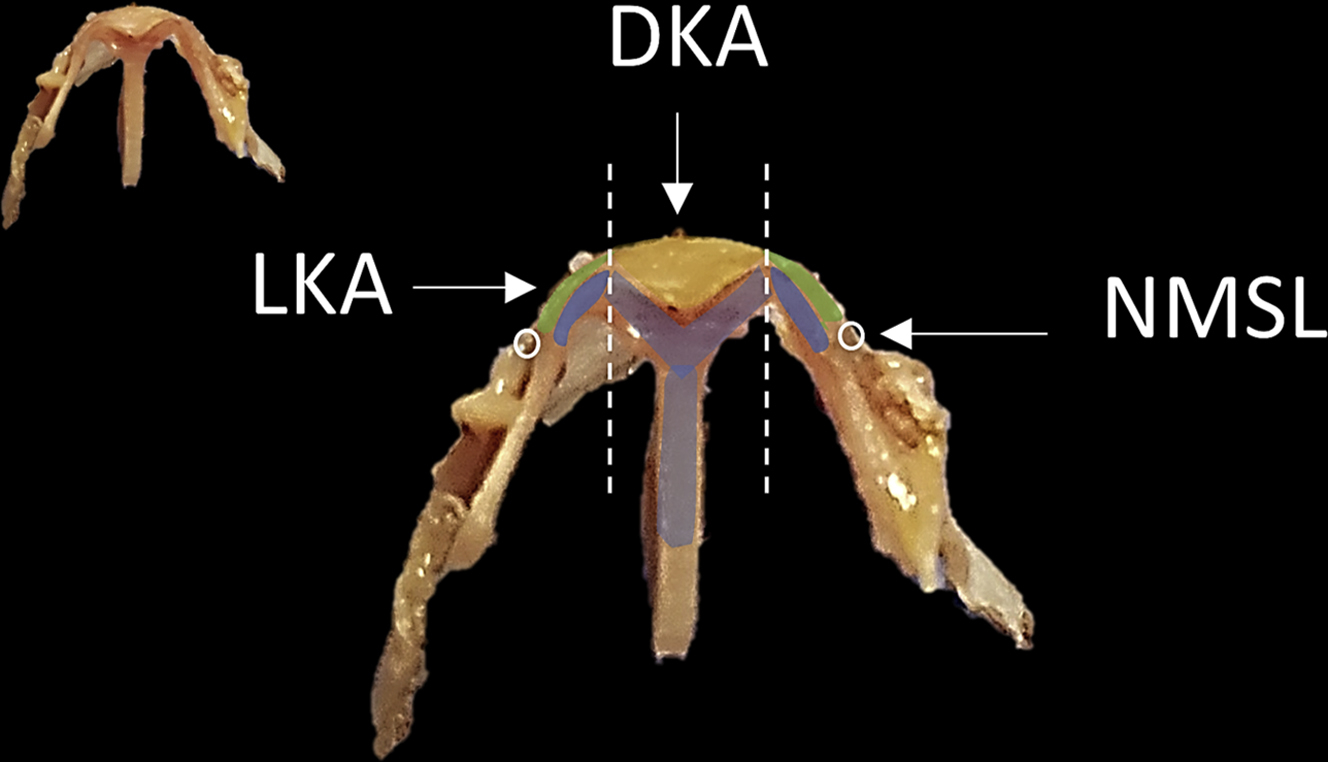
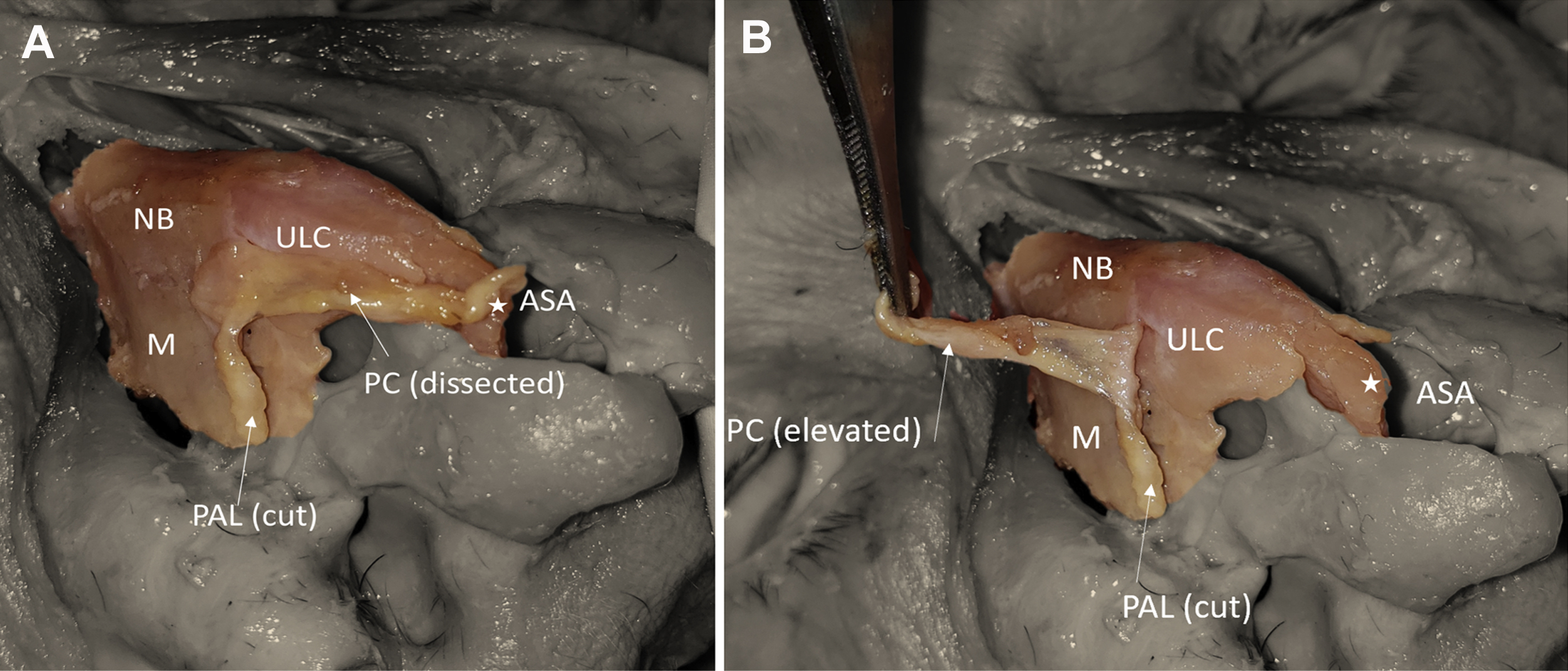
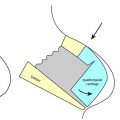
There are 2 surfaces of the nasal bones: dorsal and lateral. Thinner bone exists at the junction between these surfaces bilaterally, that hosts the convex curvature of the ULCs ( Fig. 8 ). This junction, along with the ULCs, contributes to the DALs and is considered a portion of the lateral keystone area (LKA; see Fig. 8 ). The attachment of the ULC to both the undersurface of the nasal bone and the cartilaginous septum at the midline is known as the dorsal keystone area (DKA; Figs. 9 and 10 ). , This complex also involves the fusion between the periosteum of the nasal bones and the perichondrium of the ULC ( Figs. 11 and 12 ). The overlap between the ULCs and nasal bones is variable in length (average 9 mm; Fig. 13 ). , This overlap extends both under the dorsal surface of the nasal bones, thereby contributing to the DKA, and under the lateral aspect of the nasal bones. This lateral overlap makes up the LKA. Fig. 10 shows a coronal section at the level of the keystone area, showing the overlap of the bony and cartilaginous components of both the DKA and LKA (see Figs. 8 and 10 ). Laterally, the transition of the cartilaginous component from the DKA to the LKA has been reported to be either continuous, rounded stepped, sharp-edged stepped, or a minimal joint.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


