Preservation rhinoplasty is making a resurgence as a reliable method of performing primary rhinoplasty. Dorsal preservation is an important part of the approach to preserve favorable nasal contours when performing rhinoplasty. Keys to success require proper patient selection and careful execution. There are potential sequelae, such saddle nose deformity, recurrence of the dorsal convexity, cerebrospinal fluid leak, and radix step-off. This article discusses methods and adjustments in technique to help minimize these potential problems when performing dorsal preservation.
Key points
- •
Preservation rhinoplasty is making a resurgence as a reliable method of performing primary rhinoplasty.
- •
Various septal approaches exist.
- •
Patient selection and careful execution are paramount.
Introduction
Preservation rhinoplasty has reemerged as a popular option for managing the dorsum and is changing the manner in which rhinoplasty is performed. It is apparent that the trend is toward preservation of structure to provide a natural and long-lasting outcome. There are many components of preservation rhinoplasty, including dorsal preservation and subperichondrial dissection with preservation of the ligaments in the nose. The primary concept of dorsal preservation is to avoid creating the open-roof deformity that is seen with classic hump reduction and to preserve favorable dorsal contours. , By using the push-down or let-down technique, there is no need to reconstruct the middle nasal vault with spreader grafts or spreader flaps and potentially create irregularity with dorsal hump reduction. Clinicians who argue in favor of dorsal preservation point to the complications, extra time, or additional effort required to reconstruct or the additional cartilage needed to reconstruct the middle vault. These points are all valid but the significance of these issues varies from surgeon to surgeon. Less experienced surgeons may have difficulty taking down a dorsal hump with a Rubin osteotome. In addition, the same less experienced surgeons may have difficulty reconstructing the middle nasal vault with spreader grafts. In contrast, experienced surgeons are very comfortable taking down a dorsal hump with a rasp or osteotome or reconstructing the middle nasal vault with spreader grafts or spreader flaps. The less experienced surgeons who perform the push-down or let-down can have complications such as saddle nose, asymmetries of the bony pyramid, cerebrospinal fluid (CSF) leak, radix step-off, or hump recurrence. Dorsal preservation is not free of potential complications. This article discusses measures that can be taken to try to avoid some of the potential complications associated with dorsal preservation techniques.
Preoperative analysis
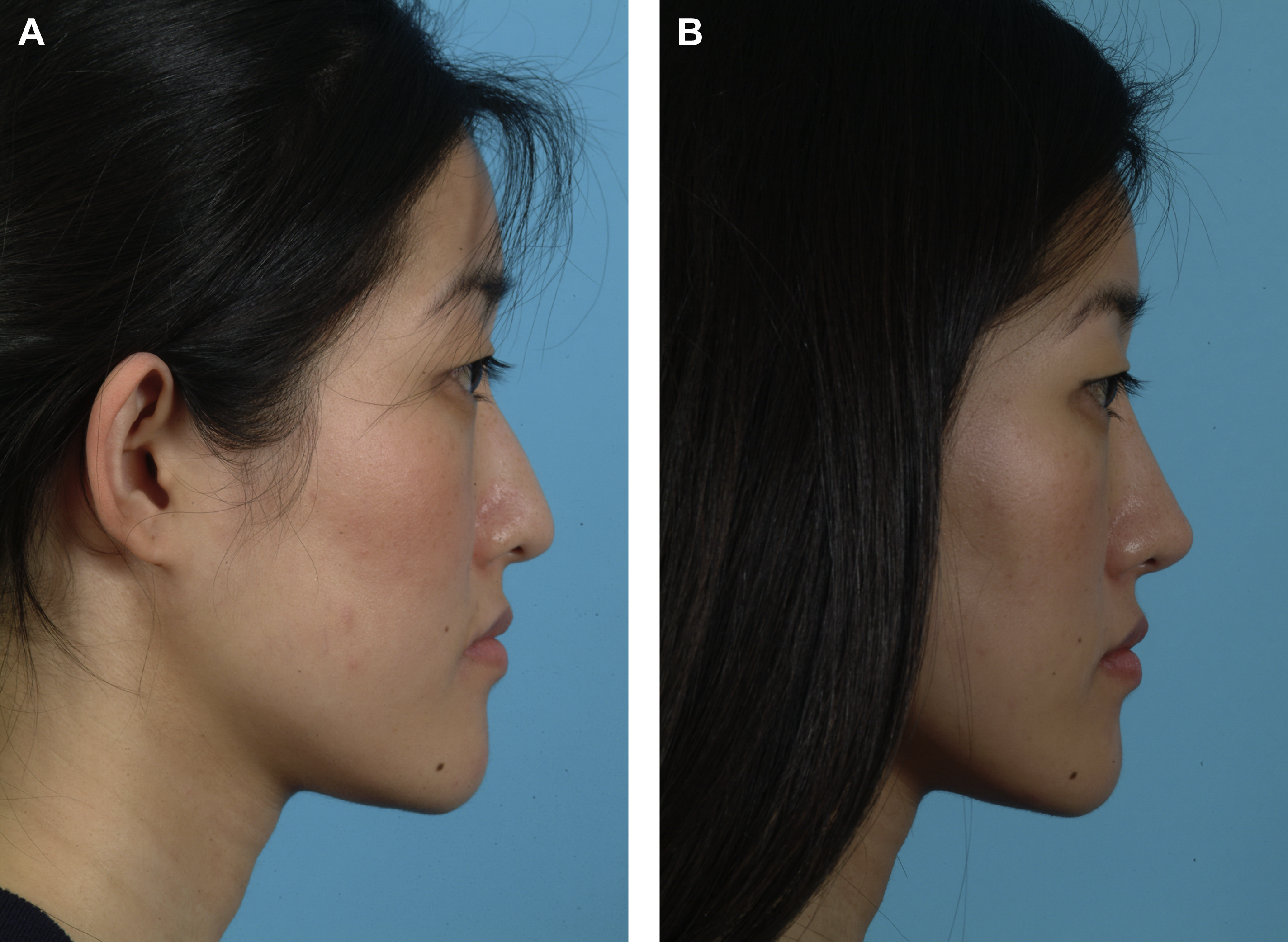
Analysis of whether dorsal hump reduction is even necessary is the first step in treating the profile. If the patient has a low radix and underprojected nasal tip (pseudohump), it is more beneficial to raise the radix, increase tip projection, and limit the amount of dorsal hump reduction ( Fig. 1 ). This approach is particularly helpful in patients who have thicker skin or are wide on frontal view. By leaving the nose more projected with a higher dorsum, the nose will look narrower on frontal view. If this approach is taken, the surgeon must be able to reliably increase tip projection. In order to increase projection, it may be necessary to stabilize the nasal base with a caudal septal extension graft. This approach can be helpful in ethic patients who tend to lack good tip support (see Fig. 1 ). In many of these patients, the authors limit hump reduction to the bony cap. This anatomic structure has been described by Daniel and Palhazi. By simply removing the bony cap, there is no need to perform a reconstruction of the bony or cartilaginous middle nasal vault. In some cases, when the bony cap is removed, the horns of the upper lateral cartilages can pop up, leaving a dorsal convexity requiring some minor reduction. In many ethnic patients, the surgery is augmenting the dorsum and not reducing it. By augmenting the dorsum, the upper two-thirds of the nose can be made narrower without manipulating the bony vault with osteotomies.
Patient selection
If profile alignment requires reduction of the height of the dorsum, the surgeon can consider dorsal preservation. Ideal patients have a normal radix and smaller, cartilaginous, or V-shaped hump. A V-shaped hump has only 1 curvature, which can be more readily flattened, whereas an S-shaped hump has 2 curvature points and is more difficult to flatten. Patients with a narrow bony and cartilaginous dorsum that is straight and favorable in appearance on frontal view also have favorable characteristics. If the patient can benefit from slight widening of the middle nasal vault or preservation of the existing dorsal aesthetic lines, the authors strongly consider a push-down or let-down technique. Other important parameters include shorter nasal bones, and a primarily cartilaginous dorsal hump. In such patients, we consider removing a subdorsal strip of cartilage to allow the cartilaginous hump to be pushed down and sutured into proper position. We may perform a bony cap removal or some rasping to contour the bone with release of the upper lateral cartilages from the lateral keystone as described by Jankowski and Ferreira. , This technique avoids the need for a bony push-down, limiting the push-down to the cartilaginous vault and eliminating the need for more extensive osteotomies. Care must be taken to prevent visibility after the bone is removed and recognize if the cartilaginous vault pops up or deforms.
Potential sequelae
One of the most common complications of the dorsal preservation technique is the radix step, which occurs if a larger strip of bone and cartilage is resected below the radix and the cut below the dorsum is very deep into the ethmoid ( Fig. 2 A). In this case, the entire pyramid can drop excessively, creating a visible step that cannot be hidden by the thicker skin over the radix. This situation occurs if the surgeon tries to use dorsal preservation techniques on noses with a very depressed kyphotic hump, without considering the option of longitudinal stretching of the pyramid. One method to minimize the step-off is to make an oblique transverse osteotomy that allows the bone to slide instead of drop vertically.
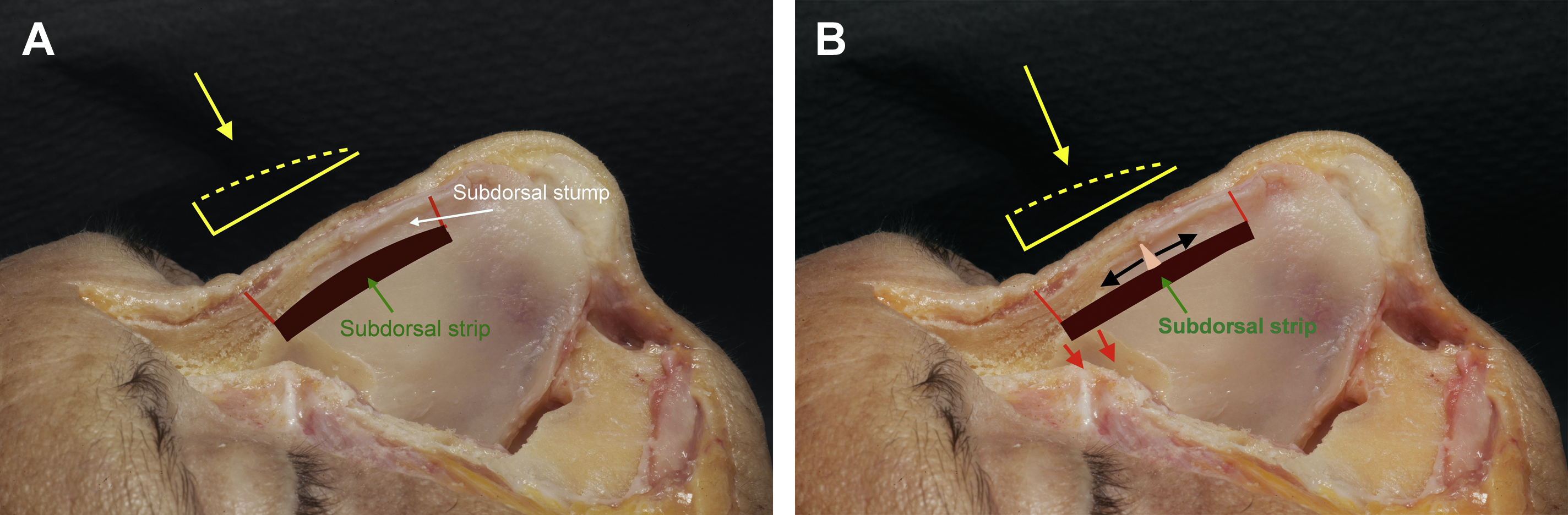
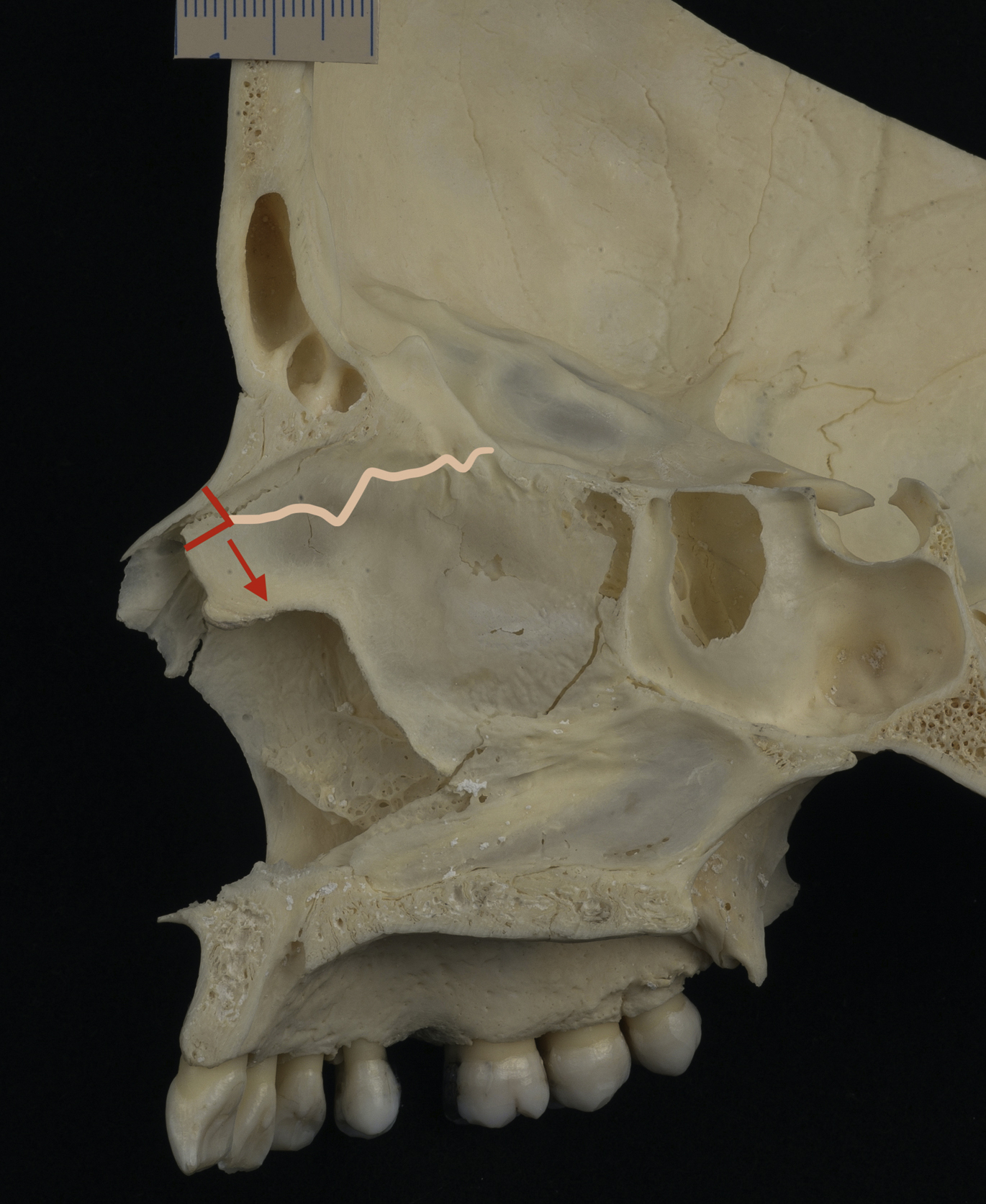
When performing a push-down, there are several potential complications that must be considered. One of the most consequential, but rare, complications is a CSF leak. CSF leak can occur when excessive force is applied to the ethmoid bone, which then can disrupt or fracture the cribriform plate, resulting in a skull base defect that can leak CSF. This complication must be avoided at all cost because the consequences, such as intracranial spread of infection, can be life threatening. Surgical repair can be difficult and fraught with its own complications. The problem lies in the transfer of energy to the ethmoid plate and skull base. When performing a push-down or let-down, a subdorsal strip is removed that may extend into the ethmoid bone, creating a subdorsal space (see Fig. 2 A). It is recommended that a subdorsal stump be left attached to the undersurface of the cartilaginous dorsum for stability purposes (see Fig. 2 A). The subdorsal stump should be approximately 2 mm to 3 mm in vertical height. If necessary, some vertical cuts are made in the subdorsal stump to allow flexion of the dorsum and allow straightening when the push-down is completed ( Fig. 2 B). In most methods of the push-down, the subdorsal stump is rectangular (see Fig. 2 ). The problem occurs when the cuts are made in the bony dorsum and the nasal bones are pushed down excessively. With the complete release of the bony vault through the lateral and transverse osteotomies, impaction onto the underlying ethmoid bone can result in excessive force on the skull base or if the osteotomy below the dorsum is executed with too much force and the fracture extends superiorly ( Fig. 3 ).
Adjustments to minimize suboptimal outcomes
Kovacevic describes a modification of the subdorsal strip and bone cuts to help minimize force on the ethmoid/skull base complex and limit the radix step. His modification involves making a triangular instead of a rectangular subdorsal stump ( Fig. 4 ). In this modification, the first step is to perform the left-sided lateral osteotomy. A subperiosteal tunnel is created around the proposed osteotomy site to allow proper mobilization of the nasal bone. In the absence of piezo, a 3-mm straight osteotome can be used to complete the lateral osteotomy. In some cases, a 3-mm bony wedge resection is performed at the site of the lateral osteotomy to allow the bony pyramid to slide down without any resistance ( Fig. 5 ). In many patients with smaller dorsal humps, the bony vault moves readily without the 3-mm wedge excision. Then a convex radix saw (Marina Medical, Davie, FL) is used to complete the transverse and radix osteotomies (see Fig. 5 ). The transverse osteotomy can also be made using a 2-mm transcutaneous bone cut. This bone cut is made just above the dorsal convexity and extends through the bone and then about 4 mm into the ethmoid bone. If made obliquely, the bone tends to hinge or slide, decreasing the chance of a step-off. The bone cut is extended to the left lateral osteotomy. This cut can be accomplished without dissecting the entire bony dorsum down to the lateral osteotomy. If using piezo, the entire bony dorsum is exposed and the bone cuts are connected under direct visualization. The bone cuts can be made using conventional osteotomes; however, the convex radix saw is helpful to make the transverse and radix osteotomies. The reason for not completing the right lateral osteotomy is to preserve the position of the bony vault until the septal work is completed and to avoid any septal disruption close to the skull base. In addition, extending the radix osteotomy 4 mm into the ethmoid avoids transfer of energy to the subdorsal osteotomy cranially.
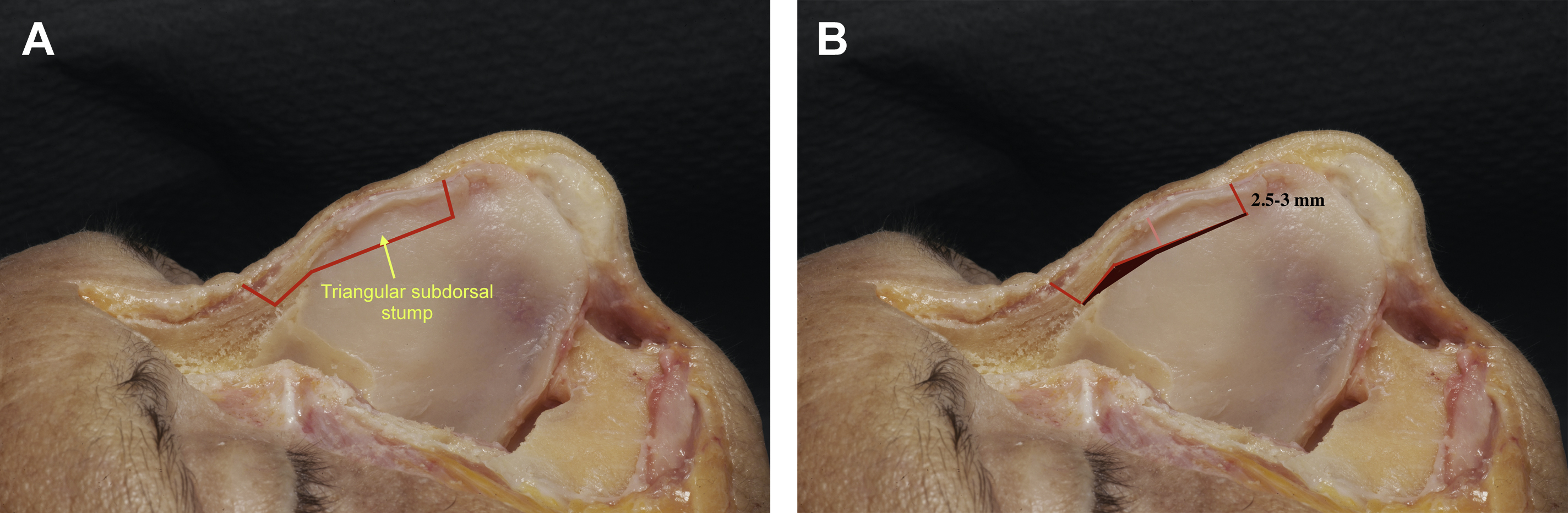
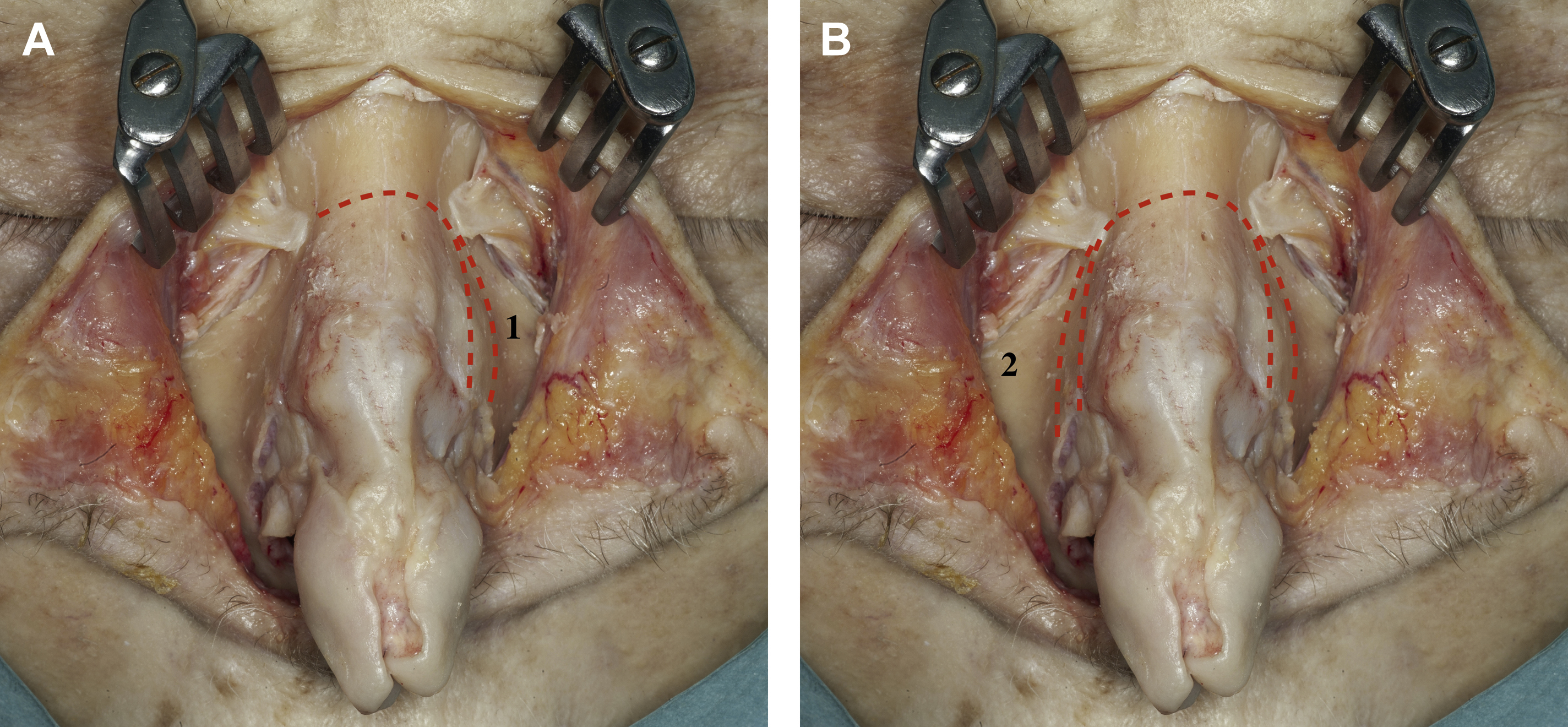
Then the septal work is completed. The first step is make the septal incision cut 3.5 mm to 4 mm cephalad to the W area (where the upper lateral cartilages meet the dorsal septum) and about 2.5 to 3 mm deep to the roof of the middle vault. This cartilaginous cut extends to the height of the dorsal hump and close to where the cartilaginous septum meets the ethmoid plate creating a subdorsal triangle ( Fig. 6 ). This cut creates a triangular cartilage stump under the roof of the middle vault. The next step is to score the bone directly under the bony hump inferior to the transverse bone cut. This step can be accomplished with a sharp osteotome or knife blade. Then a 3-mm osteotome is used to carefully cut the ethmoid bone directly under the hump and extending to the transverse osteotomy. This step can be completed with gentle force applied through the osteotome. Because the transverse bone cut extends 4 mm through the ethmoid bone, the cut made directly under the bony dorsum is isolated from the cranial segment of ethmoid bone and there is no transfer of force to the skull base (see Fig. 6 ). This bone cut can be made easily and can be visualized with an endoscope, or the mucosa can be dissected from the undersurface of the hump and the subdorsal osteotomy can be performed under direct visualization. It may also be possible to gently lift the bony dorsum to gain direct visualization. Once the subdorsal cuts are completed, a small strip (1–2 mm) of ethmoid bone can be resected to provide room for the bony dorsum to be pushed down. A bone scissor, narrow rongeur, or piezo rasp can be used, but this should not be done blindly. Avoid taking out too much bone to avoid excessive lowering of the bony dorsum and creating a radix step.

Related posts:
 Preservation Rhinoplasty
Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Modified Skoog Method for Hump Reduction
Modified Skoog Method for Hump Reduction
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


