Dorsal hump reduction is a key component of rhinoplasty. Spreader grafts are the most frequently used technique; however, dorsal irregularities may result. The modified Skoog method involves removal of the osseocartilaginous dorsal hump, its modification, further reduction of the nasal dorsum, replacement of the modified dorsal segment, and suspension of the upper lateral cartilages. The dorsal segment acts as an onlay spreader graft, preserves the middle vault, closes the open roof deformity, and creates a smooth dorsal contour from radix to anterior septal angle. The modified Skoog method produces optimal functional and aesthetic outcomes in appropriately selected patients.
Key points
- •
The evolution of dorsal hump reduction has been toward that of preservation and use of grafts that resist the contractive forces of healing.
- •
The modified Skoog technique uses a modified composite dorsal segment as an onlay spreader graft to maximize aesthetic and functional outcomes.
- •
The modified Skoog technique is ideal for patients with short nasal bones, a predominantly cartilaginous dorsal hump, normal to narrow nasal width, and thin skin.
Introduction
Nasal hump reduction is a key component of rhinoplasty. Western ideals of nasal aesthetics emphasize a straight dorsal profile, thin nasal dorsum, and smooth dorsal lines.
In the past decades, aesthetic surgery has seen great emphasis, by surgeons and patients alike, on minimally invasive procedures that use less tissue resection, anatomic preservation, and tissue repositioning to create a more natural, flattering change with less risk of revision surgery.
There has been a trend toward preservation, reshaping, and realignment rather than reduction and removal. Rather than mere reduction, the importance of adding structural grafts to create definition and resist the contractive forces of healing to preserve normal nasal function while also controlling aesthetic outcomes has gained esteem. In the area of rhinoplasty, this technique has been referred to as preservation rhinoplasty. We embrace these concepts whenever possible and the approach to nasal hump reduction has followed suit. Herein, we discuss the evolution of dorsal modification and focus on a preservation technique, the modified Skoog method.
The evolution of nasal hump reduction
Composite Resection
The classic technique for nasal hump reduction was first introduced by Joseph in 1931. This procedure involves an en bloc resection of the dorsal hump. A scalpel is used to cut through the cartilaginous dorsal septum and upper lateral cartilages, and an osteotome is used to resect the bony dorsum. The resected hump is discarded and lateral osteotomies are used to medialize the bony side walls and close the open roof deformity. Although effective for hump reduction, this method can be wrought with adverse sequelae including uneven resection of the dorsum, inadvertent over-resection, destabilization of the keystone area, creation of dorsal irregularities, excessive dorsal narrowing, and midvault collapse, resulting in both an unnatural appearance and poor nasal function.
Push-Down Technique
In response, Cottle introduced his push down technique in 1954, aimed at reducing the dorsal profile while preserving the nasal dorsum and midvault. In this technique, lateral osteotomies are performed and an inferior strip of the septum is removed, allowing for mobilization of the entire bony and cartilaginous nasal pyramid. The nasal pyramid is then pushed down into the piriform aperture, reducing the dorsal profile. Although this technique did not disturb the native dorsum or midvault, the amount of reduction was limited and it did not gain widespread popularity in the United States.
The Skoog Technique
In 1966, Skoog introduced an alternative method for dorsal hump reduction that similarly aimed to preserve the nasal dorsum and midvault. In this method, an en bloc resection of the cartilaginous and bony dorsum is performed in the same manner as that described by Joseph. The mucosa is then removed from the undersurface of the resected composite dorsum. The lateral walls of the hump are shaped, leaving the dorsum with the desired width. The bony and cartilaginous septum are then removed from the undersurface with a Ronguer, allowing the angle between the bone and cartilage to flatten. The remaining flattened dorsum is then replaced over the dorsum as a free graft. Although this technique minimized dorsal irregularities, the upper lateral cartilages were not resuspended, and nasal function continued to suffer.
Understanding the Internal Nasal Valve
Although first described by Mink in 1903, the importance of maintaining the internal nasal valves for proper nasal function was not fully understood until more recently. This new appreciation further impacted the evolution of dorsal hump reduction and created a greater emphasis on preserving the middle vault to achieve not only excellent aesthetic results but functional outcomes as well.
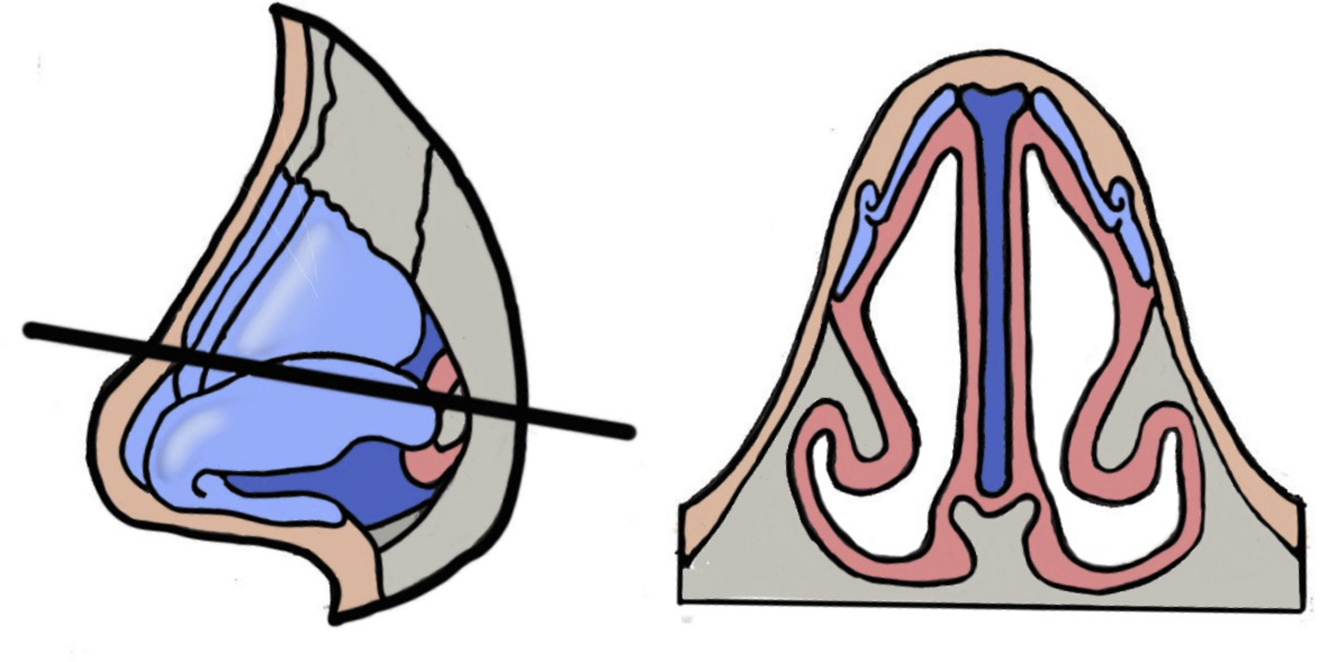
The internal nasal valve, bound by the septum, upper lateral cartilage, head of the inferior turbinate, and nasal floor, is the narrowest portion of the nasal airway ( Fig. 1 ). As such, it regulates upper airway resistance and thus nasal airflow. In accordance with Poiseuille’s law, resistance is inversely proportional to the radius of cross-sectional area to the fourth power. Thus, small changes in internal nasal valve area can have profound changes on resistance. This was confirmed by Roithmann and colleagues through the use of acoustic rhinometry and rhinomanometry. Furthermore, as the cross-sectional area of the valve decreases, a greater negative pressure is generated within the nasal cavity during inspiration owing to the Bernoulli effect. This pressure in turn can result in a dynamic collapse of the nasal sidewall, depending on the strength of the cartilaginous framework and nasal musculature resisting this pressure. Reduction rhinoplasty was found to be the second most common cause of internal nasal valve obstruction, second only to trauma, and a study by Grymer and colleagues demonstrated an average 22% decrease in the cross-sectional area at the internal nasal valve by acoustic rhinometry 6 months after standard reduction rhinoplasty.
Midvault Grafts
With this new understanding in mind, a number of techniques were introduced to reconstruct the middle vault and internal nasal valves after dorsal hump reduction. In 1984, Sheen introduced spreader grafts to reconstruct the middle vault. Spreader grafts have gained widespread popularity and have been shown to improve nasal airflow. In 1999, Alsarraf and Murakami described onlay spreader grafts from septal or conchal cartilage, and more recently, in 2004, the concept of a component dorsal hump resection in which the upper lateral cartilages are released from the septum before hump takedown and then used as autospreader grafts was introduced. These advances have greatly advanced the reconstruction of the middle vault and patency of the internal nasal valves, resulting in improved aesthetic and functional outcomes following dorsal hump reduction; however, they still have the heightened risk of creating dorsal irregularities, particularly in patients with thin skin.
The modified Skoog technique
With both function and aesthetics in mind, the modified Skoog technique was introduced in 2004 as a method of dorsal hump reduction that would allow for the preservation of the middle vault and internal nasal valves while also maintaining a natural, smooth contour of the nasal dorsum, and potentially obviating the need for lateral osteotomies. Ideal candidates for this procedure are patients with an overprojected nasal dorsum, long cartilaginous dorsum, short nasal bones, a normal to narrow bony base, and thin skin.
This technique is performed in the following steps.
- 1.
A standard open septorhinoplasty approach through transcolumellar and marginal incisions is used.
- 2.
The soft tissue envelope is elevated in the standard supraperichondrial, subperiosteal fashion.
- 3.
The anterior septal angle is exposed and bilateral mucoperichondrial flaps are elevated from the septum.
- 4.
The mucosal attachments of the medial aspect of the upper lateral cartilages and nasal bones are released. (Note: this modification was first introduced by Regnault and Alfaro in 1980. )
- 5.
Any necessary nasal tip work is performed
- 6.
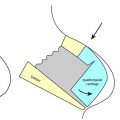
An 11-blade is held in a horizontal plane and used to perform the cartilaginous hump reduction, transecting both the septum and upper lateral cartilages from the anterior septal angle to the nasal bones, ensuring the cartilaginous attachments to the nasal bones are preserved ( Fig. 2 ).

Related posts:
 Preservation Rhinoplasty
Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


