Dermatologic Parasitology
John C. Hall MD
Dermatologic parasitology is an extensive subject and includes the dermatoses caused by three main groups of organisms: protozoa, helminthes, and arthropods.
▪ The protozoal dermatoses are exemplified by the various forms of trypanosomiases and leishmaniases (see Chapter 45).
▪ Helminthic dermatoses include those due to roundworms (ground itch, creeping eruption, filariasis, and other rare tropical diseases) and those due to flatworms (schistosomiasis, swimmer’s itch, and others) (see Chapter 45).
▪ Arthropod dermatoses are divided into those caused by two classes of organisms: the arachnids (spiders, scorpions, ticks, and mites) and the insects (lice, bugs, flies, moths, beetles, bees, and fleas). Lyme disease is caused by a spirochete that is transmitted by a tick and is discussed in Chapter 22. Rickettsial diseases are also tick borne (see Chapter 21).
In this chapter scabies, pediculosis, and bedbugs are discussed. Scabies are caused by mites, pediculosis is caused by lice, and bedbugs are caused by an insect that is usually found in mattresses and furniture. Fleabites, chigger bites, creeping eruption, swimmer’s itch, and tropical dermatoses are discussed in Chapter 45.
Scabies
Scabies (Figs. 17-1 and 17-2) is usually more prevalent in a populace ravaged by war, famine, or disease when personal hygiene becomes relatively unimportant. However, there are unexplained cyclic epidemics of this parasitic infestation. In the 1970s and 1980s, such a cycle plagued Americans. In normal times, scabies is seen in schoolchildren, elderly patients in nursing care centers, in poorer populations under crowded conditions, and in sexually active patients with multiple sex partners.
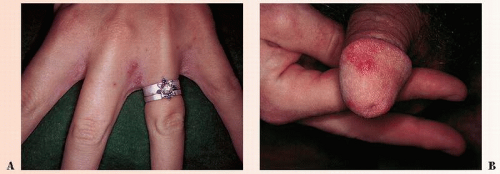 FIGURE 17-1 ▪ (A) Scabies on the hand. (B) Scabies on the penis. (Courtesy of Hoechst-Roussel Pharmaceuticals.) |
Animal scabies can occur in cats, dogs, foxes, cows, pigs, and other mammals. The disease is sarcoptic mange and is caused by Sarcoptes scabiei var canis. Direct contact with an infected animal causes a severe, generalized, polymorphous, pruritic eruption with absence of burrows and a negative wet mount for ova, parasites, or feces. This occurs 24 to 96 hours after exposure, is not associated with human-to-human transmission, and lasts only 14 to 21 days without further exposure. Treatment is accomplished by topical agents such as permethrin, malathion, or lindane for the pet and antipruritic therapy and topical or systemic corticosteroids for the temporary human host.
Presentation and Characteristics
Primary Lesions
A burrow caused by the female of the mite S. scabiei (see Fig. 17-2) measures approximately 2 mm in length and can be hidden by the secondary eruption. Small vesicles may overlie the burrows. Scabies incognito is a form of the disease in which the burrows are not easily identified. It is seen most commonly in patients who are fastidiously clean and
bathe at least once a day. Norwegian, or keratotic, scabies occurs in immunosuppressed patients. Hundreds of organisms create a psoriasiform dermatitis.
bathe at least once a day. Norwegian, or keratotic, scabies occurs in immunosuppressed patients. Hundreds of organisms create a psoriasiform dermatitis.
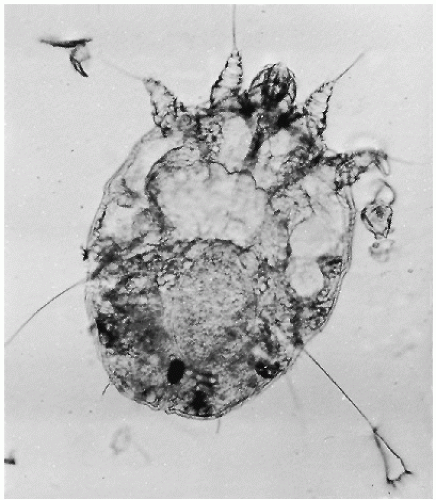 FIGURE 17-2 ▪ The female of the mite Sarcoptes scabiei. The small, oval, black body near the anal opening is a fecal pellet. Proximal to it is a vague, much larger, oval, pale-edged mass (an egg). (Courtesy of Dr. H. Parlette.) |
Secondary Lesions
Excoriations of the burrows may be the only visible pathologic process. These may be difficult to see, and magnification devices may be helpful. In severe, chronic cases, bacterial infection may be extensive and may take the form of impetigo, cellulitis, or furunculosis.
Residual nodular lesions may persist as an allergic reaction for many weeks or months after the organism is eliminated. They are often recalcitrant to therapy and topical, intralesional, and even systemic corticosteroids may be necessary. Excision may even be necessary. Nodular scabies is not contagious.
Distribution
Most commonly, the excoriations are seen on the lower abdomen and the back, with extension to the pubic, genital, and axillary areas, the legs (ankles especially), the arms (flexor wrists especially), and the webs of the fingers.
SAUER’S NOTES
1. Scabies should be ruled out in any generalized, excoriated eruption.
2. The patient should always be asked if other members of the household itch.
Subjective Complaints
Itching is intense, particularly at night when the patient is warm and in bed and the mite is more active. However, many skin diseases itch worse at night, presumably due to a lower itch threshold when relaxation occurs.
Course
The mite can persist for months and years (7-year itch) in untreated persons.
Contagiousness
Other members of the household or intimate contacts may or may not have the disease, depending on exposure and severity of the infestation.
Laboratory Findings
The female scabies mite, ova, and fecal pellets may be seen in skin scrapings that are done with a no. 15 Bard-Parker blade. The scrapings are done at the site of burrows in the skin or in areas where itching is most severe. The scrapings are then examined under the low-power magnification of the microscope (see Fig. 17-2). Potassium hydroxide (KOH) (20% solution) can be used to clear the tissue. Another method of collection is to scrape the burrow through immersion oil and then transfer the scrapings to the microscopic slides. Skill is necessary to uncover the mite by curetting or scraping.
Differential Diagnosis
▪ Pyoderma:Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree