Neonatal Skin
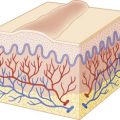
The skin of the infant differs from that of an adult in that it is thinner (40% to 60%), is less hairy, and has a weaker attachment between the epidermis and dermis. In addition, the body surface area-to-weight ratio of an infant is up to five times that of an adult. The infant is therefore at a significantly increased risk for skin injury, percutaneous absorption, and skin-associated infection. Premature infants born before 32 to 34 weeks’ estimated gestational age may have problems associated with an immature stratum corneum (the most superficial cell layer in the epidermis), including an increase in transepidermal water loss (TEWL). This increased TEWL may result in morbidity because of dehydration, electrolyte imbalance, and thermal instability. Interestingly, in the majority of premature infants an acceleration of skin maturation occurs after birth such that most develop intact barrier function by 2 to 3 weeks of life. However, in extremely low-birthweight infants, this process may take up to 4 to 8 weeks. In light of the elevated TEWL levels seen in premature infants, a variety of studies have evaluated the use of occlusive dressings or topical emollients in an effort to improve compromised barrier function.
The risk of percutaneous toxicity from topically applied substances is increased in infants, especially those born prematurely. Percutaneous absorption is known to occur through two major pathways: (1) through the cells of the stratum corneum and the epidermal malpighian layer (the transepidermal route) and (2) through the hair follicle–sebaceous gland component (the transappendageal route). Increased neonatal percutaneous absorption may be the result of the increased skin surface area-to-weight ratio as well as the stratum corneum immaturity seen in premature neonates. Although transdermal delivery methods may be distinctly advantageous in certain settings, extreme caution must be exercised in the application of topical substances to the skin of infants, given the risk of systemic absorption and potential toxicity. Table 2-1 lists some compounds reported in association with percutaneous toxicity in infants and children.
| Compound | Product | Toxicity |
|---|---|---|
| Alcohols | Skin antiseptic | Cutaneous hemorrhagic necrosis, elevated blood alcohol levels |
| Aniline | Dye used as laundry marker | Methemoglobinemia, death |
| Adhesive remover solvents | Skin preparations to aid in adhesive removal | Epidermal injury, hemorrhage, and necrosis |
| Benzocaine | Mucosal anesthetic (teething products) | Methemoglobinemia |
| Boric acid | Baby powder, diaper paste | Vomiting, diarrhea, erythroderma, seizures, death |
| Calcipotriol | Topical vitamin D 3 analog | Hypercalcemia, hypercalcemic crisis |
| Chlorhexidine | Topical antiseptic | Systemic absorption but no toxic effects |
| Corticosteroids | Topical anti-inflammatory | Skin atrophy, striae, adrenal suppression |
| Diphenhydramine | Topical antipruritic | Central anticholinergic syndrome |
| Lidocaine | Topical anesthetic | Petechiae, seizures |
| Lindane | Scabicide | Neurotoxicity |
| Mercuric chloride | Diaper rinses; teething powders | Acrodynia, hypotonia |
| Methylene blue | Amniotic fluid leak | Methemoglobinemia |
| N, N-dimethyl- m -toluamide (DEET) | Insect repellent | Neurotoxicity |
| Neomycin | Topical antibiotic | Neural deafness |
| Phenolic compounds (pentachlorophenol, hexachlorophene, resorcinol) | Laundry disinfectant, topical antiseptic | Neurotoxicity, tachycardia, metabolic acidosis, methemoglobinemia, death |
| Phenylephrine | Ophthalmic drops | Vasoconstriction, periorbital pallor |
| Povidone-iodine | Topical antiseptic | Hypothyroidism |
| Prilocaine | Topical anesthetic | Methemoglobinemia |
| Salicylic acid | Keratolytic emollient | Metabolic acidosis, salicylism |
| Silver sulfadiazine | Topical antibiotic | Kernicterus (sulfa component), agranulocytosis, argyria (silver component) |
| Tacrolimus | Topical immunomodulator | Elevated blood levels of immunosuppressive medication |
| Triple dye (brilliant green, gentian violet, proflavine hemisulfate) | Topical antiseptic for umbilical cord | Ulceration of mucous membranes, skin necrosis, vomiting, diarrhea |
| Urea | Keratolytic emollient | Uremia |
Skin Care of the Newborn
The skin of the newborn is covered with a grayish-white, greasy material termed vernix caseosa . The vernix represents a physiologic protective covering derived partially from secretions of the sebaceous glands and in part as a decomposition product of the infant’s epidermis. Vernix contains protein, lipids, and water and provides water-binding free amino acids that facilitate the adaptation from amniotic fluid immersion in utero to the dry ambient postnatal state. Although its function is not completely understood, it may act as a natural protectant cream to “waterproof” the fetus in utero , where it is submerged in the amniotic fluid. Some studies suggest that vernix be left on as a protective coating for the newborn skin and that it be allowed to come off by itself with successive changes of clothing (generally within the first few weeks of life). It has been suggested that vernix-based topical creams may be effective in augmenting stratum corneum repair and maturation in infants and could play a role in the treatment of epidermal wounds.
The skin acts as a protective organ. Any break in its integrity therefore affords an opportunity for initiation of infection. The importance of skin care in the newborn is compounded by several factors:
- 1.
The infant does not have protective skin flora at birth.
- 2.
The infant has at least one and possibly two open surgical wounds (the umbilicus and circumcision site).
- 3.
The infant is exposed to fomites and personnel that potentially harbor a variety of infectious agents.
Skin care should involve gentle cleansing with a nontoxic, nonabrasive neutral material. During the 1950s, the use of hexachlorophene-containing compounds became routine for the skin care of newborns as prophylaxis against Staphylococcus aureus infection. In 1971 and 1972, however, the use of hexachlorophene preparations as skin cleansers for newborns was restricted because of studies demonstrating vacuolization in the central nervous system (CNS) of infants and laboratory animals after prolonged application of these preparations. At the minimum, neonatal skin care should include gentle removal of blood from the face and head, and meconium from the perianal area, by gentle rinsing with water. Ideally, vernix caseosa should be removed from the face only, allowing the remaining vernix to come off by itself. However, the common standard of care is for gentle drying and wiping of the newborn’s entire skin surface, which is most desirable from a thermoregulatory standpoint. For the remainder of the infant’s stay in the hospital nursery, the buttocks and perianal regions should be cleansed with water and cotton or a gentle cloth. A mild soap with water rinsing may also be used at diaper changes if desired.
There is no single method of umbilical-cord care that has been proven to limit colonization and disease. Several methods include local application of isopropyl alcohol, triple dye (an aqueous solution of brilliant green, proflavine, and gentian violet), and antimicrobial agents such as bacitracin or silver-sulfadiazine cream. The routine use of povidone-iodine should be discouraged, given the risk of iodine absorption and transient hypothyroxinemia or hypothyroidism. A safer alternative is a chlorhexidine-containing product.
Physiologic Phenomena of the Newborn
Neonatal dermatology, by definition, encompasses the spectrum of cutaneous disorders that arise during the first 4 weeks of life. Many such conditions are transient, appearing in the first few days to weeks of life only to disappear shortly thereafter. The appreciation of normal phenomena and their differentiation from the more significant cutaneous disorders of the newborn is critical for the general physician, obstetrician, and pediatrician, as well as for the pediatric dermatologist.
At birth, the skin of the full-term infant is normally soft, smooth, and velvety. Desquamation of neonatal skin generally takes place 24 to 36 hours after delivery and may not be complete until the third week of life. Desquamation at birth is an abnormal phenomenon and is indicative of postmaturity, intrauterine anoxia, or congenital ichthyosis.
The skin at birth has a purplish-red color that is most pronounced over the extremities. Except for the hands, feet, and lips, where the transition is gradual, this quickly changes to a pink hue. In many infants, a purplish discoloration of the hands, feet, and lips occurs during periods of crying, breath holding, or chilling. This normal phenomenon, termed acrocyanosis , appears to be associated with an increased tone of peripheral arterioles, which in turn creates vasospasm, secondary dilation, and pooling of blood in the venous plexuses, resulting in a cyanotic appearance to the involved areas of the skin. The intensity of cyanosis depends on the degree of oxygen loss and the depth, size, and fullness of the involved venous plexus. Acrocyanosis, a normal physiologic phenomenon, should not be confused with true cyanosis.
Cutis Marmorata
Cutis marmorata is a normal reticulated bluish mottling of the skin seen on the trunk and extremities of infants and young children ( Fig. 2-1 ). This phenomenon, a physiologic response to chilling with resultant dilation of capillaries and small venules, usually disappears as the infant is rewarmed. Although a tendency for cutis marmorata may persist for several weeks or months, this disorder bears no medical significance and treatment generally is unnecessary. In some children cutis marmorata may tend to recur until early childhood, and in patients with Down syndrome, trisomy 18, and the Cornelia de Lange syndrome, this reticulated marbling pattern may be persistent. When the changes are persistent (even with rewarming) and are deep violaceous in color, cutis marmorata telangiectatica congenita ( Fig. 2-2 ; see also Chapter 12 ) should be considered. In some infants a white negative pattern of cutis marmorata (cutis marmorata alba) may be created by a transient hypertonia of the deep vasculature. Cutis marmorata alba is also a transitory disorder and appears to have no clinical significance.


Harlequin Color Change
Harlequin color change, not to be confused with harlequin ichthyosis (see Chapter 5 ), is occasionally observed in full-term infants but usually occurs in premature infants. It occurs when the infant is lying on his or her side and consists of reddening of one-half of the body with simultaneous blanching of the other half. Attacks develop suddenly and may persist for 30 seconds to 20 minutes. The side that lies uppermost is paler, and a clear line of demarcation runs along the midline of the body. At times, this line of demarcation may be incomplete; when attacks are mild, areas of the face and genitalia may not be involved.
This phenomenon appears to be related to immaturity of hypothalamic centers that control the tone of peripheral blood vessels and has been observed in infants with severe intracranial injury as well as in infants who appear to be otherwise perfectly normal. Although the peak frequency of attacks of harlequin color change generally occurs between the second and fifth days of life, attacks may occur anywhere from the first few hours to as late as the second or the third week of life.
Bronze Baby Syndrome
Bronze baby syndrome is a term used to describe infants who develop a grayish-brown discoloration of the skin, serum, and urine while undergoing phototherapy for hyperbilirubinemia. Although the exact source of the pigment causing the discoloration is not clear, the syndrome usually begins 1 to 7 days after the initiation of phototherapy, resolves gradually over a period of several weeks after phototherapy is discontinued, and appears to be related to a combination of photoisomers of bilirubin or biliverdin or a photoproduct of copper-porphyrin metabolism. Infants who develop bronze baby syndrome usually have modified liver function, particularly cholestasis, of various origins. Although not all babies with cholestasis develop bronze baby syndrome during phototherapy, those that do should be investigated for underlying liver disease. The disorder should be differentiated from neonatal jaundice, cyanosis associated with neonatal pulmonary disorders or congenital heart disease, an unusual progressive hyperpigmentation (universal-acquired melanosis, the “carbon baby” syndrome), and chloramphenicol intoxication (the “gray baby” syndrome), which is a disorder in infants with immature liver function who are unable to conjugate chloramphenicol and is characterized by elevated serum chloramphenicol levels, progressive cyanosis, abdominal distention, hypothermia, vomiting, irregular respiration, and vasomotor collapse. A distinctive purpuric eruption on exposed skin has also been described in newborns receiving phototherapy and is possibly related to a transient increase in circulating porphyrins. This condition, however, is unlikely to be confused with bronze baby syndrome.
Cephalohematoma
A cephalohematoma is a subperiosteal hematoma overlying the calvarium. These lesions are more common after prolonged labor, instrument-assisted deliveries, and abnormal presentations. They usually develop over the first hours of life and present as subcutaneous swellings in the scalp. They do not cross the midline ( Fig. 2-3 ), because they are limited to one cranial bone, which helps to distinguish them from caput succedaneum (see the next paragraph). Occasionally, a cephalohematoma may occur over a linear skull fracture. Other potentially associated complications include calcification (that may persist radiographically for years), hyperbilirubinemia, and infection. Although infected lesions (which are rare) may require aspiration, most lesions require no therapy with spontaneous resorption and resolution occurring over several months.

Caput Succedaneum
Caput succedaneum is a localized edema of the newborn scalp related to the mechanical forces involved in parturition. It is probably related to venous congestion and edema secondary to cervical and uterine pressure, and as such is more common with prolonged parturition and seen most often in primigravidas. Caput succedaneum presents as a boggy scalp mass and may result in varying degrees of bruising and necrosis in addition to the edema, at times with tissue loss. In distinction to cephalohematoma, caput succedaneum lesions often cross the midline. These lesions tend to resolve spontaneously over 48 hours, and treatment is generally unnecessary. One possible complication in cases of severe caput succedaneum is permanent alopecia. Halo scalp ring refers to an annular alopecia that presents in a circumferential ring around the scalp in infants with a history of caput. It represents a pressure necrosis phenomenon, and the hair loss may be transient or, occasionally, permanent.
Complications from Fetal and Neonatal Diagnostic Procedures
Fetal complications associated with invasive prenatal diagnostic procedures include cutaneous puncture marks, scars or lacerations, exsanguination, ocular trauma, blindness, subdural hemorrhage, pneumothorax, cardiac tamponade, splenic laceration, porencephalic cysts, arteriovenous or ileocutaneous fistulas, digital loss (in 1.7% of newborns whose mothers had undergone early chorionic villus sampling), musculoskeletal trauma, disruption of tendons or ligaments, and occasionally gangrene. Cutaneous puncture marks, which occur in 1% to 3% of newborns whose mothers have undergone amniocentesis, may be seen as single or multiple 1- to 6-mm pits or dimples on any cutaneous surface of the newborn ( Fig. 2-4 ).

Fetal scalp monitoring can result in infection, bleeding, or fontanel puncture, and prenatal vacuum extraction can produce a localized area of edema, ecchymosis, or localized alopecia. The incidence of scalp electrode infection varies from 0.3% to 5.0%, and although local sterile abscesses account for the majority of adverse sequelae, S. aureus or Gram-negative infections, cellulitis, tissue necrosis, subgaleal abscess, osteomyelitis, necrotizing fasciitis, and neonatal herpes simplex infections may also occur as complications of this procedure ( Fig. 2-5 ). It is not unusual for new parents to be under the false impression that fetal scalp electrodes are the cause of aplasia cutis congenita (ACC; see later in this chapter).

Scalp injuries sustained during the birth process tend to be minor and include lacerations, erosions, and ecchymoses. Injuries of the scalp and face occur in approximately 16% of vacuum-assisted deliveries and in 17% of forceps-assisted deliveries.
Transcutaneous oxygen monitoring (application of heated electrodes to the skin for continuous detection of tissue oxygenation) and pulse oximetry may also result in erythema, tissue necrosis, and first- or second-degree burns. Although lesions associated with transcutaneous oxygen monitoring generally resolve within 48 to 60 hours, persistent atrophic hyperpigmented craters may at times be seen as a complication. Frequent (every 2 to 4 hours) changing of electrode sites and reduction of the temperature of the electrodes to 43° C, however, can lessen the likelihood of this complication.
Anetoderma of prematurity refers to macular depressions or outpouchings of skin associated with loss of dermal elastic tissue seen in premature infants. Reports suggest that these cutaneous lesions may correlate with placement of electrocardiographic or other monitoring electrodes or leads.
Calcinosis cutis may occur on the scalp or chest of infants or children at sites of electroencephalograph or electrocardiograph electrode placement, as a result of diagnostic heel sticks performed during the neonatal period, or after intramuscular or intravenous administration of calcium chloride or calcium gluconate for the treatment of neonatal hypocalcemia. Seen primarily in high-risk infants who receive repeated heel sticks for blood chemistry determinations, calcified nodules usually begin as small depressions on the heels. With time, generally after 4 to 12 months, tiny yellow or white papules appear ( Fig. 2-6 ), gradually enlarge to form nodular deposits, migrate to the cutaneous surface, extrude their contents, and generally disappear spontaneously by the time the child reaches 18 to 30 months of age. Although calcified heel nodules are usually asymptomatic, children may at times show signs of discomfort with standing or wearing shoes. In such instances, gentle cryosurgery and curettage can be both diagnostic and therapeutic. Calcinosis cutis after electroencephalography or electrocardiography is more likely to be seen in infants and young children or individuals where the skin has been abraded and usually disappears spontaneously within 2 to 6 months. It can be avoided by the use of an electrode paste that does not contain calcium chloride, and like calcified heel sticks, they may be treated by gentle cryosurgery and curettage.

Abnormalities of Subcutaneous Tissue
Skin turgor is generally normal during the first few hours of life. As normal physiologic dehydration occurs during the first 3 or 4 days of life (up to 10% of birth weight), the skin generally becomes loose and wrinkled. Subcutaneous fat is normally quite adequate at birth and increases until about 9 months of age, thus accounting for the traditional chubby appearance of the healthy newborn. A decrease or absence of this normal panniculus is abnormal and suggests the possibility of prematurity, postmaturity, or placental insufficiency.
Sclerema neonatorum and subcutaneous fat necrosis (SCFN) are two disorders that affect the subcutaneous fat of the newborn. Although there is considerable diagnostic confusion between these two entities, there are several distinguishing features that enable a clinical differentiation ( Table 2-2 ). Sclerema neonatorum seems to occur significantly less often than SCFN.
| Sclerema Neonatorum | Subcutaneous Fat Necrosis |
|---|---|
| Premature infants | Full-term or postmature infants |
| Serious underlying disease (sepsis, cardiopulmonary disease, diarrhea, or dehydration) | Healthy newborns; may have history of perinatal asphyxia or difficult delivery |
| Wax-like hardening of skin and subcutaneous tissue | Circumscribed, indurated, erythematous nodules and plaques |
| Whole body except palms and soles | Buttocks, thighs, arms, face, shoulders |
| Poor prognosis; high mortality | Excellent prognosis; treat associated hypercalcemia, if present |
Sclerema Neonatorum
Sclerema neonatorum is a diffuse, rapidly spreading, wax-like hardening of the skin and subcutaneous tissue that occurs in premature or debilitated infants during the first few weeks of life. The disorder, usually associated with a serious underlying condition such as sepsis or other infection, congenital heart disease, respiratory distress, diarrhea, or dehydration, is characterized by a diffuse nonpitting woody induration of the involved tissues. The process is symmetrical, usually starting on the legs and buttocks, and may progress to involve all areas except the palms, soles, and genitalia. As the disorder spreads, the skin becomes cold, yellowish-white, mottled, stony hard, and cadaver-like. The limbs become immobile, and the face acquires a fixed mask-like expression. Infants with this disorder become sluggish, feed poorly, show clinical signs of shock, and in a high percentage of cases die.
Although the etiology of this disorder is unknown, it appears to represent a nonspecific sign of severe illness rather than a primary disease. Infants with this disorder are characteristically small or premature, debilitated, weak, cyanotic, and lethargic. In 25% of cases the mothers are ill at the time of delivery. Exposure to cold, hypothermia, peripheral chilling with vascular collapse, and an increase in the ratio of saturated to unsaturated fatty acids in the triglyceride fraction of the subcutaneous tissue (because of a defect in fatty acid mobilization) have been hypothesized as possible causes for this disorder but lack confirmation.
The histopathologic findings of sclerema neonatorum consist of edema and thickening of the connective tissue bands around the fat lobules. Although necrosis and crystallization of the subcutaneous tissue have been described, these findings are more characteristically seen in lesions of SCFN.
The prognosis of sclerema neonatorum is poor, and mortality occurs in 50% to 75% of affected infants. In a series of 51 infants with sclerema neonatorum in a special-care nursery within a Bangladeshi hospital, the fatality rate was 98%. In infants who survive, the cutaneous findings resolve without residual sequelae. There is no specific therapy, although steroids and exchange transfusion have been used.
Subcutaneous Fat Necrosis
Subcutaneous fat necrosis (SCFN) is a benign, self-limited disease that affects apparently healthy, full-term newborns and young infants. It is characterized by sharply circumscribed, indurated, and nodular areas of fat necrosis ( Fig. 2-7 ). The etiology of this disorder remains unknown but appears to be related to perinatal trauma, asphyxia, hypothermia, and in some instances, hypercalcemia. Although the mechanism of hypercalcemia in SCFN is not known, it has been attributed to aberrations in vitamin D or parathyroid homeostasis. Birth asphyxia and meconium aspiration seem to be commonly associated. In one large series, 10 out of 11 infants with SCFN had been delivered via emergency cesarean section for fetal distress, and nine of the 11 had meconium staining of the amniotic fluid. The relationship between SCFN, maternal diabetes, and cesarean section, if any, is unclear. SCFN after ice-bag application for treatment of supraventricular tachycardia has been reported, and it has also been observed after selective head or generalized cooling for hypoxic–ischemic encephalopathy.

The onset of SCFN is generally during the first few days to weeks of life. Lesions appear as single or multiple localized, sharply circumscribed, usually painless areas of induration. Occasionally the affected areas may be tender, and infants may be uncomfortable and cry vigorously when they are handled. Lesions vary from small erythematous, indurated nodules to large plaques, and sites of predilection include the cheeks, back, buttocks, arms, and thighs. Many lesions have an uneven lobulated surface with an elevated margin separating it from the surrounding normal tissue. Histologic examination of SCFN reveals larger-than-usual fat lobules and an extensive inflammatory infiltrate, needle-shaped clefts within fat cells, necrosis, and calcification. Magnetic resonance imaging (MRI) reveals decreased T1 and increased T2 signal intensity in affected areas.
The prognosis for SCFN is excellent. Although lesions may develop extensive deposits of calcium, which may liquefy, drain, and heal with scarring, most areas undergo spontaneous resolution within several weeks to months. Hypercalcemia is a rare association, and infants with this finding may require low calcium intake, restriction of vitamin D, and/or systemic corticosteroid therapy. Etidronate therapy has been reported for treatment of recalcitrant SCFN-associated hypercalcemia. Infants should be monitored for several months after delivery, because the onset of hypercalcemia can be delayed for several months. Other rare systemic complications may include thrombocytopenia, hypoglycemia, and hypertriglyceridemia, all of which tend to be mild and/or self-limited.
Miscellaneous Cutaneous Disorders
Miliaria
Differentiation of the epidermis and its appendages, particularly in the premature infant, is often incomplete at birth. As a result of this immaturity, a high incidence of sweat-retention phenomena may be seen in the newborn. Miliaria, a common neonatal dermatosis caused by sweat retention, is characterized by a vesicular eruption with subsequent maceration and obstruction of the eccrine ducts. The pathophysiologic events that lead to this disorder are keratinous plugging of eccrine ducts and the escape of eccrine sweat into the skin below the level of obstruction (see Chapter 8 ).
Virtually all infants develop miliaria under appropriate conditions. There are two principal forms of this disorder:
- 1.
Miliaria crystallina (sudamina), which consists of clear superficial pinpoint vesicles without an inflammatory areola;
- 2.
Miliaria rubra (prickly heat), representing a deeper level of sweat gland obstruction and characterized by small discrete erythematous papules, vesicles, or papulovesicles ( Fig. 2-8 ).
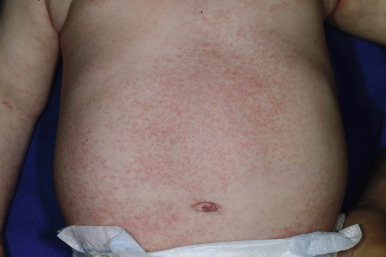
Figure 2-8
Miliaria rubra. Multiple, erythematous, pinpoint macules and papules in an infant with atopic dermatitis who was being treated with overapplication of greasy emollients.
The incidence of miliaria is greatest in the first few weeks of life owing to the relative immaturity of the eccrine ducts, which favors poral closure and sweat retention. A pustular form of miliaria rubra has been observed in association with pseudohypoaldosteronism during salt-losing crises.
Therapy for miliaria is directed toward avoidance of excessive heat and humidity. Light-weight cotton clothing, cool baths, and air conditioning are helpful in the management and prevention of this disorder. Avoidance of emollient overapplication (i.e., in infants with atopic dermatitis) should also be recommended, especially in warm, humid climates or in the winter when infants are bundled under heavy clothing.
Milia
Milia, small retention cysts, commonly occur on the face of newborns. Seen in 40% to 50% of infants, they result from retention of keratin within the dermis. They appear as tiny 1- to 2-mm pearly white or yellow papules. Particularly prominent on the cheeks, nose, chin, and forehead, they may be few or numerous and are often grouped ( Fig. 2-9 ). Lesions may occasionally occur on the upper trunk, limbs, penis, or mucous membranes. Although milia of the newborn may persist into the second or third month, they usually disappear spontaneously during the first 3 or 4 weeks of life and accordingly require no therapy. Persistent milia in an unusual or widespread distribution, particularly when seen in association with other defects, may be a manifestation of hereditary trichodysplasia (Marie-Unna hypotrichosis), dystrophic forms of epidermolysis bullosa, Bazex or Rombo syndromes, or the oral-facial-digital syndrome, type I.

Bohn Nodules and Epstein Pearls
Discrete, 2- to 3-mm round, pearly white or yellow, freely movable elevations at the gum margins or midline of the hard palate (termed Bohn nodules and Epstein pearls , respectively) are seen in up to 85% of newborns. Clinically and histologically the counterpart of facial milia, they disappear spontaneously, usually within a few weeks of life, and require no therapy.
Sebaceous Gland Hyperplasia
Sebaceous gland hyperplasia represents a physiologic phenomenon of the newborn manifested as multiple, yellow to flesh-colored tiny papules that occur on the nose, cheeks, and upper lips of full-term infants ( Fig. 2-10 ). A manifestation of maternal androgen stimulation, these papules represent a temporary disorder that resolves spontaneously, generally within the first few weeks of life.

Acne Neonatorum
Occasionally infants develop a facial eruption that resembles acne vulgaris as seen in adolescents ( Fig. 2-11 ). Although the etiology of this disorder is not clearly defined, it appears to develop as a result of hormonal stimulation of sebaceous glands that have not yet involuted to their childhood state of immaturity. In mild cases of acne neonatorum, therapy is often unnecessary; daily cleansing with soap and water may be all that is required. Occasionally, mild keratolytic agents or topical antibiotics may be helpful (see Chapter 8 ). Unusually severe or recalcitrant cases of acne neonatorum warrant investigation for underlying androgen excess.

A facial acneiform eruption in infants has been associated with the saprophytic Malassezia species and has been termed neonatal cephalic pustulosis (see Chapter 8 ). Lesions consist of pinpoint papules, papulopustules, or larger pustules, and they are located on the cheeks, chin, and forehead ( Fig. 2-12 ). A correlation may exist between the clinical severity of lesions and the colonization with this fungal saprophyte. In these infants, topical antifungal agents may lead to more rapid resolution of lesions.

Erythema Toxicum Neonatorum
Erythema toxicum neonatorum (ETN), also known as toxic erythema of the newborn, is an idiopathic, asymptomatic, benign, self-limiting, cutaneous eruption in full-term newborns. Lesions consist of erythematous macules, papules, and pustules ( Fig. 2-13 ), or a combination of these, and may occur anywhere on the body, especially the forehead, face, trunk, and extremities. The fact that these lesions (which histologically reveal follicular-centered eosinophils) often tend to spare the palms and soles may be explained by the absence of pilosebaceous follicles in these areas.

ETN often initially appears as a blotchy, macular erythema that then develops firm, 1- to 3-mm, pale yellow or white papules and pustules. The erythematous macules are irregular or splotchy in appearance, varying from a few millimeters to several centimeters in diameter. They may be seen in sharp contrast to the surrounding unaffected skin, may blend into a surrounding erythema, or may progress to a confluent eruption.
Although ETN appears most commonly during the first 3 to 4 days of life, it has been seen at birth and may be noted as late as 10 days of age. Exacerbations and remissions may occur during the first 2 weeks of life, and the duration of individual lesions varies from a few hours to several days. The etiology of ETN remains obscure. One study suggested that it represents an immune response to microbial colonization of the skin at the hair follicle. ETN incidence data are variable. Some authors report an incidence as low as 4.5%; others report incidences varying from 31% to 70% of newborns. Two large prospective series of skin findings in newborns (one in the United States and one in Turkey) found incidences of 7% and 13.1%, respectively. The incidence of ETN clearly appears to increase with increasing gestational age of the infant. No sexual or racial predisposition has been noted.
ETN is usually diagnosed clinically. Skin biopsy, which is rarely necessary, reveals a characteristic accumulation of eosinophils within the pilosebaceous apparatus. The diagnosis can be rapidly differentiated from other newborn pustular conditions by cytologic examination of a pustule smear that with Wright or Giemsa staining reveals a predominance of eosinophils. Affected infants may have a peripheral eosinophilia. Although the eosinophilic response has led some observers to attribute the etiology of this disorder to a hypersensitivity reaction, specific allergens have never been implicated or confirmed.
Since erythema toxicum is a benign, self-limiting, asymptomatic disorder, no therapy is indicated. Occasionally, however, it may be confused with other pustular eruptions of the neonatal period, including transient neonatal pustular melanosis (TNPM), milia, miliaria, and congenital infections including candidiasis, herpes simplex, or bacterial processes. Of these, the congenital infections are the most important diagnostic considerations because of the implications for possible systemic involvement. Table 2-3 lists the differential diagnosis of the newborn with vesicles or pustules.
| Clinical Disorder | Comments |
|---|---|
| Acrodermatitis enteropathica | Periorificial erosive dermatitis common |
| Acropustulosis of infancy | Recurrent crops of acral pustules |
| Behçet syndrome | Oral and genital ulcers; may have cutaneous papules, vesicles, and pustules ( Fig. 2-14 ) |
| Eosinophilic folliculitis | Scalp and extremities most common sites |
| Epidermolysis bullosa | Trauma-induced blistering; bullae and erosions |
| Erythema toxicum neonatorum | Blotchy erythema, evanescent |
| Incontinentia pigmenti | XLD; linear and whorled patterns; may be vesicles, as well as warty lesions (hypopigmentation and hyperpigmentation occur later) |
| Infectious | |
| Bacterial | |
| Group A or B streptococci | |
| Staphylococcus aureus | Superficial blisters rupture easily |
| Listeria monocytogenes | |
| Pseudomonas aeruginosa | |
| Other Gram-negatives | |
| Fungal | |
| Candidiasis | Palms and soles involved; nail changes often present |
| Viral | |
| Herpes simplex | 3 types: SEM, CNS, disseminated |
| Varicella zoster | |
| Cytomegalovirus | Blueberry muffin lesions more common |
| Spirochetal | |
| Syphilis | Red macules, papules; palm and sole scaling |
| Langerhans cell histiocytosis | Crusting, erosions, palms and soles, LAD |
| Miliaria | Especially intertriginous, occluded sites; crystallina type presents with clear vesicles without erythema; rubra type presents with red papules and papulopustules |
| Neonatal Behçet syndrome | |
| Neonatal cephalic pustulosis | Acneiform disorder, presenting with numerous pustules on the cheeks, forehead, chin; may respond to topical antifungal agents |
| Pustular psoriasis | |
| Scabies | Crusting, burrows; palms and soles usually involved |
| Transient neonatal pustular melanosis | Mainly affects black skin; peripheral collarettes; pigment persists for months |
| Urticaria pigmentosa | Stroking leads to urtication (Darier sign) |
| Vesiculopustular eruption of transient myeloproliferative disorder | Vesicles and pustules (face > elsewhere); usually in setting of trisomy 21 |

Eosinophilic Pustular Folliculitis
Eosinophilic pustular folliculitis (EPF) is an idiopathic dermatosis that occurs in both adults and infants. When it occurs in neonates or young infants, it may be clinically confused with other vesiculopustular disorders. Lesions consist of follicular pustules, most commonly occurring on the scalp and the extremities ( Fig. 2-15 ). They tend to recur in crops, in a similar fashion to acropustulosis of infancy (see below), and some suggest that these conditions may be related. As opposed to the adult form of EPF, the infancy-associated type does not reveal lesions grouped in an annular arrangement. EPF tends to present before 14 months of age in the majority of patients. Histologic evaluation reveals an eosinophilic, follicular, inflammatory infiltrate, and peripheral eosinophilia may be present. EPF of infancy appears to be distinct from classic (adult) and human immunodeficiency virus (HIV)-associated EPF, although an infant with HIV and EPF has been reported. Importantly, infantile EPF may occasionally be the presenting sign of hyperimmunoglobulinemia E syndrome (HIES) (see Chapter 3 ). Treatment for EPF is symptomatic, including topical corticosteroids and antihistamines, with eventual spontaneous resolution by 3 years of age in the majority of patients. Topical tacrolimus may be useful in patients who are unresponsive to topical corticosteroids.

Impetigo Neonatorum
Impetigo in newborns may occur as early as the second or third day or as late as the second week of life. It usually presents as a superficial vesicular, pustular, or bullous lesion on an erythematous base. Vesicles and bullae are easily denuded, leaving a red, raw, and moist surface, usually without crust formation. Blisters are often wrinkled, contain some fluid, and are easily denuded. Lesions tend to occur on moist or opposing surfaces of the skin, as in the diaper area, groin, axillae, and neck folds. S. aureus pustulosis (or neonatal pustulosis) is a characteristic manifestation of cutaneous S. aureus infection in the neonate or infant. Patients have small pustules on an erythematous base ( Fig. 2-16 ), often distributed in the diaper region. The lesions denude easily upon swabbing, and culture is positive for S. aureus . Streptococci may occasionally be causative. In term or late preterm neonates with localized involvement and without fever or systemic symptoms, evaluation for serious bacterial illness is generally not required, and treatment in the outpatient setting is often sufficient. However, a complete blood cell count and blood culture is advisable given the rare association with bacteremia.

The term pemphigus neonatorum is an archaic misnomer occasionally applied to superficial bullous lesions of severe impetigo widely distributed over the surface of the body. However, a transient neonatal form of pemphigus vulgaris does exist and is caused by transplacental passage of antibodies from a mother with the same disease (see Chapter 13 ).
Sucking Blisters
Sucking blisters, presumed to be induced by vigorous sucking on the affected part in utero , are seen in up to 0.5% of normal newborns as 0.5- to 2-cm oval bullae or erosions on the dorsal aspect of the fingers, thumbs, wrists, lips, or radial aspect of the forearms. These lesions, which must be differentiated from bullous impetigo, epidermolysis bullosa, and herpes neonatorum, resolve rapidly and without sequelae.
Transient Neonatal Pustular Melanosis
Transient neonatal pustular melanosis (TNPM) is a benign self-limiting disorder of unknown etiology characterized by superficial vesiculopustular lesions that rupture easily and evolve into hyperpigmented macules ( Fig. 2-17 ). This disorder is seen in fewer than 1% of newborns and occurs most commonly in infants with black skin. Lesions begin as superficial sterile pustules ( Fig. 2-18 ) that rupture easily to leave a collarette of fine, white scale around a small hyperpigmented macule. Although the distribution may be diffuse, common areas of involvement include the inferior chin, forehead, neck, lower back, and shins. Rarely, vesicles that do not progress to pigmented macules may be detected on the scalp, palms, and soles.


Wright-stained smears of the pustules of TNPM, in contrast to lesions of ETN, demonstrate variable numbers of neutrophils, few or no eosinophils, and cellular debris. Histopathologic evaluation is usually unnecessary.
TNPM is a benign disorder without associated systemic manifestations, and therapy is unnecessary. The pustular lesions usually disappear within 24–48 h, leaving behind hyperpigmented macules that fade gradually, usually over several weeks to months. Occasionally, newborns may have solely the hyperpigmented macules, in which case it is presumed that the pustular phase occurred (and resolved) in utero .
Acropustulosis of Infancy
Acropustulosis of infancy, also known as infantile acropustulosis ( IA ), is an idiopathic pustular disorder with onset usually between birth and 2 years of age. It is characterized by recurrent, pruritic, vesiculopustular lesions that recur every few weeks to months. The lesions begin as pinpoint erythematous papules and enlarge into well-circumscribed discrete pustules. They are concentrated on the palms ( Fig. 2-19 ) and soles ( Fig. 2-20 ) and appear in lesser numbers on the dorsal aspect of the hands, feet, wrists, and ankles. Occasional lesions may occur on the face and scalp.


The differential diagnosis of IA includes scabies, dyshidrotic eczema, pustular psoriasis, ETN, TNPM, impetigo, and subcorneal pustular dermatosis. However, the characteristic presentation and course of IA is usually distinctive enough to render a clinical diagnosis. A smear of pustule contents (or histologic evaluation) reveals large numbers of neutrophils and occasionally eosinophils. Although the etiology of IA remains unclear, several authors have noted a possible association with preceding scabies infestation. IA appears to be common in internationally adopted children.
Patients with IA experience fewer and less intense flares of their lesions with time, and the entire process usually subsides within 2 to 3 years. Pruritus, however, may be severe early in the course, making therapy desirable. Possible associations include irritability, sleeplessness, excoriation, and secondary bacterial infection. Systemic antihistamines, usually in high doses, may relieve pruritus. High-potency topical corticosteroids are quite effective for this condition, and given the limited distribution of lesions, the epidermal thickness at affected (acral) sites, and the periodicity of flares, concerns regarding systemic absorption of these medications should be minimal. Dapsone has long been a recommended therapy for severe cases, but the risk-to-benefit ratio of this agent is not generally justified in patients with IA.
Congenital Erosive and Vesicular Dermatosis
Congenital erosive and vesicular dermatosis healing with reticulated supple scarring is an uncommon disorder characterized by erosive and bullous lesions that, as the name implies, are present at birth and heal with characteristic scarring. Although its cause is unknown, it appears to represent a nonhereditary intrauterine event such as infection or amniotic adhesions, or perhaps an unusual healing defect of immature skin. The disorder generally involves skin of the trunk, extremities, scalp, face, and occasionally the tongue, with sparing of the palms and soles.
Congenital erosive and vesicular dermatosis occurs most often in premature infants and presents with extensive cutaneous ulcerations and intact vesicles that develop crusting and then heal during the first month of life. Occasionally, blistering may continue to occur beyond infancy. Generalized, supple, reticulated scars occur with alternating elevated and depressed areas ( Fig. 2-21 ). Up to 75% of the cutaneous surface may be involved, and the skin lesions have been described as having depressed hypopigmented regions alternating with normal to hyperpigmented zones. Scars on the trunk and head, which often have a cobblestone-like appearance, may be oriented along the cutaneous lines of cleavage; on the limbs they tend to follow the long axes of the extremities. Facial involvement was present in roughly 50% of published cases in one review. Although the eyebrows are usually normal, alopecia may be noted on the scalp. Nails may be absent or hypoplastic, and affected areas on the tongue may manifest scarring and absence of papillae. Dentition is usually normal. Hyperthermia, especially in warm weather or after exertion, is common and although sweating is absent in scarred areas, compensatory hyperhidrosis in normal-appearing skin may be noted. Chronic conjunctivitis is a major continuing problem for these patients, and corneal scarring may occur. Some patients have also been found to have neurologic defects, including mental and motor retardation, hemiparesis, microcephaly, pachygyria, cerebral palsy, and seizures.

Seborrheic Dermatitis
Seborrheic dermatitis is a common, self-limiting condition of the scalp, face, ears, trunk, and intertriginous areas characterized by greasy scaling, redness, fissuring, and occasional weeping. It appears to be related to the sebaceous glands and has a predilection for so-called “seborrheic” areas where the density of these glands is high. It usually presents in infants with a scaly dermatitis of the scalp termed cradle cap ( Fig. 2-22 ) and may spread over the face, including the forehead, ears, eyebrows, and nose. Other areas of involvement include the intertriginous zones, umbilicus, and anogenital region ( Fig. 2-23 ). (For a more detailed discussion of seborrheic dermatitis and its therapy, see Chapter 3 .)


Leiner Disease
The term Leiner disease refers to a shared phenotype for a number of nutritional and immunologic disorders characterized by severe seborrheic dermatitis with exfoliation, failure to thrive, and diarrhea. The disorder may occur during the first week of life but generally starts around 2 to 4 months of age. Patients are particularly prone to recurrent yeast and Gram-negative infections. Among disorders that may show this phenotype are: deficiency or dysfunction of complement, Bruton agammaglobulinemia, severe combined immunodeficiency, and HIES.
Diaper Dermatitis
Diaper dermatitis is perhaps the most common cutaneous disorder of infancy and early childhood. The term is used to describe an acute inflammatory skin reaction in the areas covered by the diaper. The incidence of diaper dermatitis is estimated to be between 7% and 35%, with a peak incidence at 9 to 12 months of age.
The term diaper rash is commonly used as a diagnosis, as though the diverse dermatoses that may affect this region constitute a single clinical entity. In actuality, diaper dermatitis is not a specific diagnosis and is best viewed as a variable-symptom complex initiated by a combination of factors, the most significant being prolonged contact with urine and feces, skin maceration, and, in many cases, secondary infection with bacteria or Candida albicans . Although diaper dermatitis may often be no more than a minor nuisance, eruptions in this area may not only progress to secondary infection and ulceration but may become complicated by other superimposed cutaneous disorders or represent a manifestation of a more serious disease.
The three most common types of diaper dermatitis are chafing dermatitis, irritant contact dermatitis, and diaper candidiasis. However, the differential diagnosis of diaper dermatitis is broad ( Box 2-1 ). In patients in whom a response to therapy is slow or absent, alternative diagnoses should be considered and appropriate diagnostic evaluations performed. The following sections contain a brief discussion of several potential causes of diaper dermatitis. Many of these entities are discussed in more detail in other chapters.
Chafing dermatitis
Irritant contact dermatitis
Diaper candidiasis
Seborrheic dermatitis
Psoriasis
Intertrigo
Jacquet dermatitis
Perianal pseudoverrucous papules and nodules
Miliaria
Folliculitis
Impetigo
Scabies
Nutritional deficiency (i.e., acrodermatitis enteropathica, cystic fibrosis, biotin deficiency)
Allergic contact dermatitis
Atopic dermatitis
Granuloma gluteale infantum
Langerhans cell histiocytosis
Burns
Child abuse
Epidermolysis bullosa
Congenital syphilis
Varicella/herpes
Tinea cruris
Chronic bullous dermatosis of childhood
Bullous mastocytosis
Chafing Dermatitis
The most prevalent form of diaper dermatitis is the chafing or frictional dermatitis that affects most infants at some time. Generally present on areas where friction is the most pronounced (the inner surfaces of the thighs, the genitalia, buttocks, and the abdomen), the eruption presents as mild redness and scaling and tends to wax and wane quickly. This form responds quickly to frequent diaper changes and good diaper hygiene.
Irritant Contact Dermatitis
Irritant contact diaper dermatitis usually involves the convex surfaces of the buttocks, the vulva, the perineal area, the lower abdomen, and the proximal thighs, with sparing of the intertriginous creases ( Fig. 2-24 ). The disorder may be attributable to contact with proteolytic enzymes in stool and irritant chemicals such as soaps, detergents, and topical preparations. Other significant factors appear to be excessive heat, moisture, and sweat retention associated with the warm local environment produced by the diaper.

The etiology of irritant contact diaper dermatitis is multifactorial, and past hypotheses have included potential roles for ammonia, bacteria and bacterial products, and urine pH. In 1921 when Cooke demonstrated that an aerobic Gram-positive bacillus ( Bacillus ammoniagenes ) was capable of liberating ammonia from urea, this organism was pinpointed as the etiologic agent of most diaper dermatoses. More recent studies, however, have refuted the role of urea-splitting bacteria in the etiology of this disorder and incriminate a combination of wetness, frictional damage, impervious diaper coverings, and increase in skin pH. It is suggested that urinary wetness increases the permeability of the skin to irritants as well as the pH of the diaper environment, thus intensifying the activities of the fecal proteases and lipases, the major irritants responsible for this disorder.
Several technological innovations in the design of disposable diapers and other diapering products have aimed to reduce moisture and irritancy in this environment, thus decreasing the risk of irritant dermatitis. The introduction of absorbent gelling materials into diaper technology was one such breakthrough and has been shown to result in less diaper dermatitis than conventional cellulose-core disposable diapers. Other recent innovations include nonirritating disposable diaper wipes and diapers designed to deliver petrolatum-based formulations to the skin.
A blistering, erosive contact dermatitis has been observed after oral ingestion (either intentional or accidental) of senna-containing laxatives. Patients typically have with well-demarcated, diamond-shaped eroded plaques with desquamation that in some cases initially could be mistaken for scalding burns. Prolonged contact with stool (i.e., via overnight wearing of the diaper) is often reported.
Allergic Contact Dermatitis
Although not traditionally considered a common cause for diaper dermatitis, allergic contact dermatitis has received increasing attention in the literature in recent years (see Chapter 3 ). Potential associations to consider include chemical constituents of the diaper (rubber additives, rubber accelerator compounds, adhesive resins), topically applied diaper products such as emollients and “butt balms” (emulsifiers), and baby wipes (fragrances and preservatives). Disperse dyes, which are used to impart color to synthetic fabrics, can also be contact sensitizers and are found in some disposable diapers.
Diaper Candidiasis
Candidal (monilial) diaper dermatitis is a commonly overlooked disorder and should be suspected whenever a diaper rash fails to respond to usual therapeutic measures. Cutaneous candidiasis is a possible sequela of systemic antibiotic therapy and should be considered in any diaper dermatitis that develops during or shortly after antibiotic administration.
Candidal diaper dermatitis presents as a widespread, beefy-red erythema on the buttocks, lower abdomen, and inner aspects of the thighs. Characteristic features include a raised edge, sharp marginalization with white scales at the border, and pinpoint pustulovesicular satellite lesions (the diagnostic hallmark) ( Fig. 2-25 ). Although cutaneous candidiasis commonly occurs in association with oral thrush ( Fig. 2-26 ), the oral mucosa may be uninvolved. Infants harbor C. albicans in the lower intestine, and it is from this focus that infected feces present the primary source for candidal diaper eruptions.


If necessary, the diagnosis of candidal diaper dermatitis may be confirmed by microscopic examination of a potassium hydroxide preparation of skin scrapings, which reveals egg-shaped budding yeasts and hyphae or pseudohyphae. Growth of yeast on Sabouraud medium implanted with skin scrapings can also confirm the diagnosis, usually within 48 to 72 hours.
Seborrheic Dermatitis
Seborrheic dermatitis of the diaper area may be recognized by the characteristic salmon-colored, greasy plaques with a yellowish scale and a predilection for intertriginous areas (see above). Coincident involvement of the scalp, face, neck, and postauricular and flexural areas helps to establish the diagnosis. Seborrheic dermatitis of the diaper region may be difficult to distinguish from psoriasis.
Psoriasis
Psoriasis of the diaper area must also be considered in persistent diaper eruptions that fail to respond to otherwise seemingly adequate therapy ( Fig. 2-27 ). The sharp demarcation of lesions suggests diaper area psoriasis, but the typical scaling of psoriasis may be obscured because of the moisture of the diaper region. The presence of nail changes and red, well-marginated plaques with silvery mica-like scales on the trunk, face, axillae, umbilicus, or scalp may help confirm this diagnosis (see Chapter 4 ), although affected infants may have involvement limited to the diaper area.

Intertrigo
Intertrigo (see Chapter 17 ) is a common skin eruption in the diaper area, particularly in hot weather or when infants are overdressed. It usually involves the inguinal creases, the intergluteal area, and the thigh creases (especially in chubby babies), and presents as bright red erythema often with a mild white-yellow exudate. Nondiapered areas of involvement include the anterior neck fold and the axillae.
Jacquet Dermatitis
The term Jacquet dermatitis is used to describe a severe erosive diaper eruption with ulcerated papules or nodules ( Fig. 2-28 ). In male infants, erosion and crusting of the glans penis and urinary meatus may result in painful or difficult urination.

Perianal Pseudoverrucous Papules and Nodules
This is an eruption composed of verrucous (wart-like) papules has been observed to occur in children with incontinence of stool or urine. These patients have verrucous papules and nodules of the perianal and suprapubic regions, possibly representing a distinct reaction to severe irritant diaper dermatitis. Reported patients had a history of delayed ileoanal anastomosis for Hirschsprung disease, encopresis, or urinary incontinence. The importance of this diagnosis lies in differentiating it from condylomata acuminata or other more serious dermatoses.
Acrodermatitis Enteropathica
Acrodermatitis enteropathica, a disorder of zinc deficiency, may mimic a severe irritant contact dermatitis in the diaper area (see Chapter 24 ). Patients have a periorificial erosive dermatitis that is often most accentuated in the diaper region ( Fig. 2-29 ) but also may involve the perioral face. Erythema and pustules may involve intertriginous or acral sites, and diarrhea, failure to thrive, and alopecia are commonly present.