11 Orthognathic Correction of Jaw Deformities
Summary
Orthognathic correction of jaw deformities in the pediatric population aims to correct the dental occlusion, along with addressing an equally important goal to improve facial aesthetics. A comprehensive presurgical workup and evaluation must include intra- and extraoral examinations, facial photographs, diagnostic radiographs, mounted dental models, occlusion records, and a facebow transfer. In skeletally immature patients, the nature of the deformity, the operations necessary for correction, and the psychosocial impact of surgery must all be considered when determining the appropriate timing for an operation. Recognition of common facial patterns can be helpful in determining appropriate corrective operations. The most common operations used in orthognathic surgery are the Le Fort I (LFI) osteotomy for repositioning of the maxilla and the bilateral sagittal split ramus osteotomies for movement of the mandible.
11.1 Introduction
As many as 5% of adolescents in the United States have a dentofacial deformity that cannot be corrected with orthodontic treatment alone. Advances in operative and anesthetic techniques since von Langenbeck’s original description of a maxillary osteotomy in 1895 have allowed maxillary and mandibular osteotomies to become safe and predictable. In the last decade, the combination of three-dimensional treatment planning with low-profile rigid fixation has ushered in a new era of precision in orthognathic surgery.
11.2 Diagnosis and Treatment Planning
Evaluation begins with comprehensive facial and oral examinations, photographs, radiographs, mounted dental models, registration of the occlusion, and a facebow transfer.
The facial examination is performed in natural head position, which is achieved by asking the patient to focus on a distant point at eye level. The shape of the face is characterized, such as square or round, and the facial index (ratio of height to width) is calculated. Normal facial indices are 1.35:1 for men and 1.3:1 for women. The face is evaluated for symmetry at all levels. Vertical facial proportions are assessed by measuring the distances from trichion to glabella, glabella to subnasale, and subnasale to menton; each section should comprise approximately one-third of the total facial height. The lower facial third can be further divided from subnasale to stomion and from stomion to menton, which should account for the one-third and two-thirds, respectively, of the entire lower facial one-third. Transverse proportions are evaluated by partitioning the face vertically into five equal sections that are each the width of the eye from the medial canthus to the lateral canthus. Shape and symmetry of the nose are determined. Lip morphology and posture are evaluated both in repose and in function. During repose, 2 to 4 mm of the maxillary incisor teeth should be visible. In full smile, the canine tips should be seen without excessive gingival show or dark buccal corridors. Presence and depth of the labiomental sulcus are evaluated.
On intraoral examination, the presence and health of the complete adult dentition, the dental midlines in relation to the midsagittal plane, the angle classification of occlusion, overjet, and overbite are determined. The occlusal plane is evaluated from both the frontal and the lateral positions. Study casts are used to analyze the intra-arch and interarch relationships.
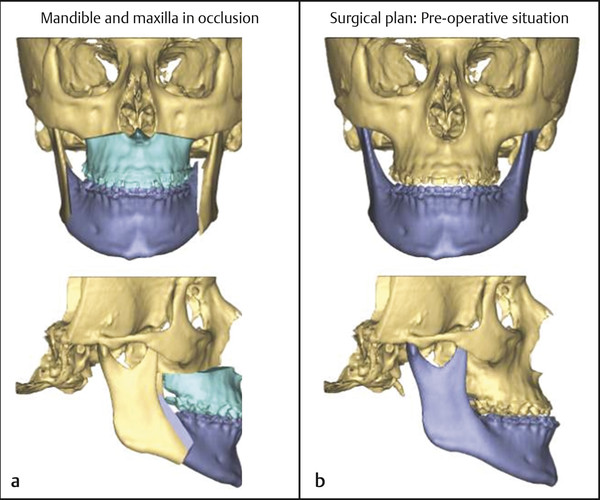
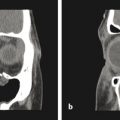
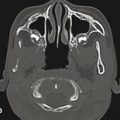
The radiographic evaluation has historically consisted of a series of plain X-rays, including panoramic, lateral cephalometric, and posterior–anterior cephalometric images. This two-dimensional series has largely been replaced by computed tomography (CT) or cone-beam CT, from which two- and three-dimensional images can be extracted. Three-dimensional imaging has improved accuracy in the planning and simulation of surgical movements (Fig. 11‑1) and in evaluation of relevant anatomic structures, including the airway space, temporomandibular joints, and inferior alveolar nerve canals.
The preoperative assessment also includes an analysis of the patient’s level of skeletal maturity. The chronological, skeletal, and dental ages; the nature of the deformity and required corrective operations; and the effect of the deformity on psychosocial development are all considered when determining the appropriate time for an operation. Growth of the maxilla is completed before that of the mandible, with the mandible closely following the skeletal growth pattern. Girls typically reach skeletal maturity between 15 and 16 years of age; boys continue to grow until 16 to 18 years of age or longer. Menarche is a useful marker for the growth cycle for girls, as skeletal growth is usually completed by 2.5 to 3 years thereafter. Evaluation of vertical height, use of hand-wrist radiographs, and overlays of tracings of serial lateral cephalograms can be used to assess the timing of facial growth. An operation involving only advancement of the mandible in the direction of growth can be pursued before skeletal maturity, with low risk for postoperative mandibular growth leading to a new malocclusion. Movements that are not in the direction of growth and bimaxillary surgery should be delayed until after the cessation of growth, unless psychosocial indications dictate earlier operation.
Recognition of common facial patterns can be helpful in determining appropriate corrective operations. Examples include the following:
Class III skeletal pattern: This is most commonly caused by maxillary hypoplasia but can be due to mandibular hyperplasia or a combination of these. It is corrected by maxillary advancement mandibular setback or both (Fig. 11‑2).
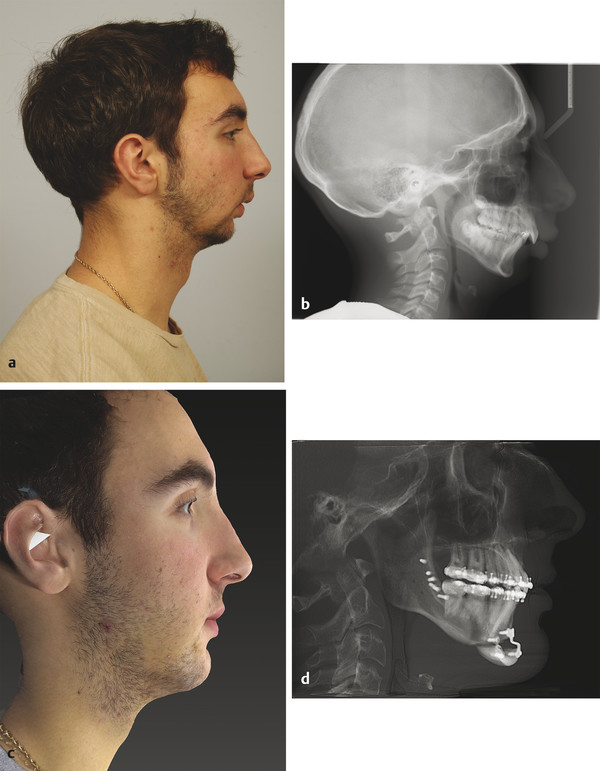
Class II skeletal pattern: This pattern is typically caused by mandibular hypoplasia and is corrected by mandibular advancement (Fig. 11‑3).
Vertical maxillary excess (VME): It is characterized by excess gingival show, a steep mandibular plane angle, increased total anterior facial height, and decreased contribution of the upper facial height to the total facial height. An anterior open bite is often present. It is corrected by superior repositioning of the maxilla, often with flattening of the occlusal plane. Bimaxillary surgery is often required.
Facial asymmetry: It presents with various etiologies, including asymmetric mandibular growth, condylar hyperplasia or resorption, trauma, and malformations such as hemifacial microsomia. It is corrected by bimaxillary surgery. The ideal vertical position of the maxilla must be determined in order to identify the proper fulcrum of rotation for the correction.

Fig. 11.2 A 20-year-old woman with a class III skeletal pattern and a lower facial asymmetry. (a,b) Preoperative photographs demonstrating a thin and poorly supported upper lip. (c–e) Preoperative dental occlusion. (f–h) Preoperative radiographs showing maxillary sagittal hypoplasia and mandibular asymmetry. 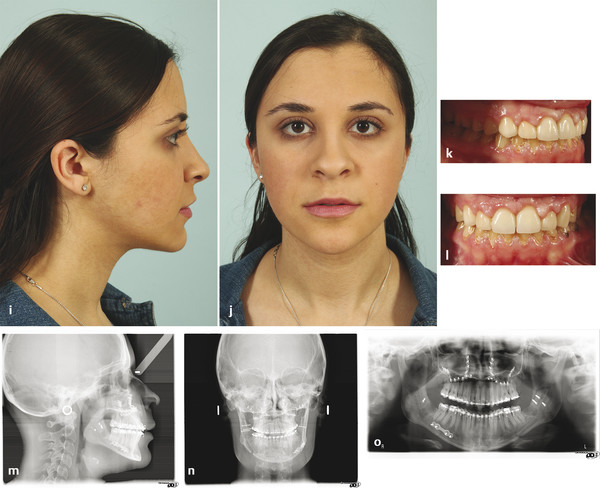
(i–l) Postoperative facial and intraoral photographs after Le Fort I osteotomy, with advancement and anterior disimpaction, and bilateral sagittal split osteotomies, with mandibular rotation. (m–o) Postoperative radiographs demonstrating the planned osteotomies, skeletal movements, and internal fixation.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


