3 Deformational Plagiocephaly, Brachycephaly, and Scaphocephaly
Summary
Deformational plagiocephaly is a common condition that affects infants. Patients have a head preference when supine, usually because of torticollis. As a result, the cranium becomes misshaped over the first few months of life. Treatment includes positioning strategies or cranial molding device.
3.1 Introduction
In 1992, the American Academy of Pediatrics initiated the “Back to Sleep Campaign” in an effort to reduce the incidence of sudden infant death syndrome. This policy advocated a paradigm shift of infant sleep positioning in Western countries from prone to supine. The recommendation was widely implemented and resulted in an estimated 40% reduction in the incidence of sudden infant death syndrome in the United States. One of the unforeseen consequences of the campaign was a rise in deformational cranial flattening and asymmetry. Such alternations of cranial shape were less commonly seen in prone-slept infants and were very common in certain Eastern countries that historically placed their sleeping infants supine. However, precipitous rise in deformational changes in the early 1990s sparked much concern from clinicians and parents alike. Several large craniofacial centers even misdiagnosed this condition as lambdoidal craniosynostosis and began undertaking widespread operative correction. The confusion eventually cleared; however, the diagnosis and treatment of plagiocephaly remain a topic of much debate. According to some estimates, the prevalence is as high as 20% in healthy infants.
3.2 Diagnosis and Terminology
The literature is full of incorrect terminology related to deformational flattening. Many authors and clinicians refer to every form of cranial flattening as “plagiocephaly.” This generally applied term is nonspecific. Deformational cranial flattening can be asymmetric, symmetric, or a combination. Plagiocephaly is derived from the Greek words plagios, meaning oblique or slanted, and kephalē, meaning head (Fig. 3‑1). This condition occurs primarily in infants who consistently favor turning their head to one side, that is, those with congenital muscular torticollis (CMT). The resultant cranial shape has been compared to a “parallelogram,” but the frontal asymmetry is less severe than what is observed in the occiput, and the shape is more trapezoidal. Asymmetric growth of the head often is accompanied by facial asymmetry—anterior (sagittal) shift of the ipsilateral forehead, ear, and cheek. Plagiocephaly is the most common cause of clinically evident facial asymmetry in infants and should be included in the differential diagnosis for any child with such findings.

Brachycephaly (Greek word brachy = short) denotes symmetrical occipital flattening and compensatory parietal widening. Infants with this condition have little or no rounding on the back of the head and appear to have a disproportionately wide or “big” head when viewed from the front (Fig. 3‑2). The posterior vertex may appear taller than the front (turricephaly), giving a sloped appearance to the head in profile. The cranial width-to-length ratio, termed the cranial or cephalic index (CI), is generally higher than normal (>0.85). Most children with this condition also have some element of concurrent asymmetry, or plagiocephaly. The combination effect, termed “asymmetric brachycephaly,” is the most common type of deformational shape.

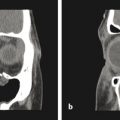
Deformational scaphocephaly (“boatlike head”) is an uncommon variant of plagiocephaly (Fig. 3‑3). It is more commonly seen in infants who have extreme head rotation to one side or in premature infants that are positioned side to side in the intensive care units. Flattening develops on the side(s) of the head, and compensatory expansion occurs in the anterior and posterior cranium. These infants tend to develop a long, slender head, colloquially referred to by some as a “toaster head.” There is often relatively pronounced facial asymmetry. This presentation can be confused with scaphocephaly caused by sagittal craniosynostosis, or premature fusion of the sagittal suture. In contrast to deformational scaphocephaly, sagittal craniosynostosis typically results in frontal bossing, bilateral occipital/parietal narrowing posterior to the anterior fontanelle, and decreased vertical height of the posterior cranium. Facial asymmetry is rare in sagittal synostosis. Most infants with this type of craniosynostosis have a head circumference in excess of the 90th percentile.

3.2.1 Radiographic Imaging
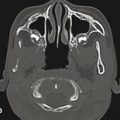
In general, any child with an abnormal head shape should be referred to a specialist before ordering radiographic studies. The overwhelming majority of infants with cranial asymmetry will have deformation and not synostosis, and a specialist can usually distinguish these processes from craniosynostosis by history and physical examination alone. This approach avoids exposing infants to unnecessary radiation and possible anesthetic exposure. If imaging is deemed necessary, the specialist is best suited to determine what is needed, based on the diagnostic need. The accuracy of plain radiography to diagnose suture fusion is questionable. Computed tomography (CT) is costly, often requires sedation, and involves low-dose ionizing radiation. The impact of such exposure is controversial; however, theoretical studies suggest that even a low-dose CT in an infant can increase the risk of lethal brain cancer.
3.3 Etiology
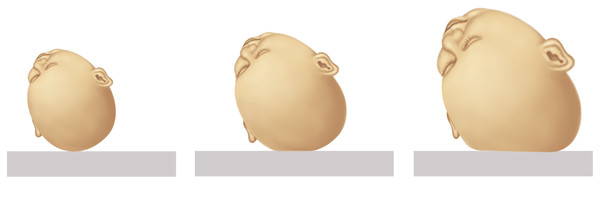
Deformational changes are thought to arise predominantly in the postnatal period in response to external forces between the sleeping surface or bed and the growing infant cranium. The cranium grows passively in response to minor internal pressure exerted by the rapidly growing infant brain. This process is fastest in early infancy and tapers dramatically even after the first year of life. When an infant is placed on a resting surface, there is a contact force generated between the head and the surface (Newton’s third law). If the point of contact is not changed, the counterforce will restrict cranial growth in the area of contact, and over time, any volume increases will be displaced to areas where there is no resistance (Fig. 3‑4). This is analogous to how a pumpkin flattens as it grows in a field—it cannot expand into the ground and must grow parallel to it. Most parents of affected children begin to notice head flattening in their infants at an average of 6 to 8 weeks of age, because it takes this long for cranial flattening to manifest. The compensatory and redirected growth will result in progressive flattening. Fortunately, most infants have sufficient neck range of motion and strength to alter (or allow the parent to alter) their head position and the area of contact with the bed. Those who lack this capacity are at greatest risk for developing flattening.
The reasons why some infants are able to change their head position (and avoid flattening) while others are not is worth discussion. Numerous risk factors have been linked to the development of deformational flattening, including supine sleep position, multiple births, developmental delay, small maternal pelvis, breech position, oligohydramnios, male gender, gestational diabetes, nulliparity of mother, high birth weight, large neonatal head size, vaginal delivery, prolonged length of postdelivery hospital stay (>4 days), and prolonged duration of stage II labor. Although these variables seem unrelated, they share a common pathogenic link to the development of deformational cranial flattening: each directly or indirectly impairs infant head mobility early in life. For example, most of the risk factors described earlier are also associated with the development of CMT, the most common risk factor for deformational flattening. Congenital muscular torticollis is not always easy to detect in a newborn, but the presence of a “preferred” head position early in life is highly suggestive. Infants with CMT have restricted motion in one direction and excessive head rotation in the other. This is an imbalance of the sternocleidomastoid muscles from in utero positioning—one contracted and the other stretched and atrophied. The characteristic head position is tilted to one side (toward the side of the tight muscle) and rotated to the other (toward weaker muscle). In most infants, increased motor development allows gradual resolution of CMT. The timing of improvement can vary based on the severity of the contracture or imbalance and the neuromuscular development of the infants. Once the infant can move his or her head, usually at 4 months of age, further flattening is unlikely.
The two other major etiologic groupings, prematurity and developmental delay, can also increase the risk of developing cranial flattening because they delay the development of independent head mobility. In infants who have both CMT and one of these other variables (e.g., twins), the risk of developing deformational flattening is markedly increased.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


