Craniofacial Anaplastology: Prosthetic Osseointegration
Chad A. Purnell
Rosemary Seelaus
Pravin K. Patel
DEFINITION
Anaplastology derives from the Greek ana to make again, anew, upon plastos—something made, formed, molded logy—the study of art and science of restoring a malformed or absent part of the human body through artificial means.
Prosthetic derives from Greek prósthesis, addition, application, attachment as an artificial device that replaces a missing body part that may be lost through trauma, disease, or congenital conditions.
Prosthetic and autologous reconstructive techniques are complementary, and in many circumstances, both are required to achieve an optimal aesthetic outcome in the reconstruction of craniofacial defects.1 Prosthetic reconstruction can result in significantly improved quality of life for patients when conventional reconstruction reaches its limits.1,2
Although autologous techniques remain the standard for long-term stable nasal and ear reconstruction, it frequently requires multistage surgical procedures with difficulty in achieving consistency of outcome and patient acceptability. Though the prosthetic approach can achieve consistency in outcome with minimal surgical intervention, it requires a lifetime of maintenance4,5 (Table 1). Each approach must be considered by having the patient and family involved in the discussion. However, in some instances such as orbital exenteration, ocular and periorbital prosthesis is the only option for the patient as no autogenous alternatives exist.3
Facial prosthetics can be either adhesive retained or fixed to osseointegrated implants. Other means of retention have been described but are less ideal. Due to disadvantages of skin reactions and less secure fixation with adhesives, implant-retained prostheses are most commonly used and result in the higher patient satisfaction.1,4
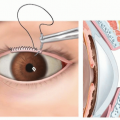
Osseointegration derives from the Greek osteon, bone, and the Latin integrare, to make whole. The term refers to the direct structural and functional connection between living bone and the surface of a load-bearing implant.5 Osseointegrated implants may retain a prosthesis through magnets or through a bar-and-clip mechanism (FIG 1).
Table 1 Comparison of Autologous vs Prosthetic Techniques for Facial Reconstruction | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
ANATOMY
The placement of osseointegrated implants into the craniofacial skeleton requires an understanding of the bony buttresses of the face (FIG 2). These areas of greater bony strength provide adequate bone stock for implant placement.
The patient-specific anatomy for cranial bone thickness and the mastoid region must be taken into consideration for placement of temporal bone osseointegrated implants and implants for bone conducting hearing amplification.
Orbital prostheses are retained by the thickened bony rim of the orbit. Nasal prostheses are retained by the thickened bony rim of the pyriform aperture.
PATIENT HISTORY AND PHYSICAL FINDINGS
Because of the extensive deformity whether of congenital, traumatic, or from tumor ablation, a multidisciplinary team tailored to the patient’s needs will help in achieving the patient’s goals with an understanding of what can and what cannot be achieved by surgical autologous and prosthetic approaches. The team ideally consists of a craniofacial surgeon, an anaplastologist, a psychologist, and in the case of auricular reconstruction and bone anchored implants, an audiologist and otolaryngologist are included. The psychologist plays a critical role in providing the supportive voice for the patient during the decision-making process and in the accepting of the outcome with their own expectations, which may not be technically achievable. Communication and educating the patient and family is critical.
A history of the patient should be collected, with particular focus on the area to be reconstructed. History of pathology leading to tissue loss, prior reconstructive attempts and donor sites, and pathology that contributes to wound healing should all be elicited. This importantly includes a history of tobacco use, corticosteroid use, and radiation therapy.
This examination should fully assess soft tissue quality and vascularity of the area to be reconstructed. Areas targeted for placement of implants must have stable and adequate soft tissue coverage.

FIG 1 • Magnet (left) and bar-and-clip (right) attachment methods for prostheses.
Bone in areas for potential osseointegrated implant placement should be assessed for quality and areas of potential bone loss. This assessment is best done through skeletal imaging.
The patient should be evaluated to determine the appropriateness of practical prosthetic use. This includes an evaluation of manual dexterity (to don/doff prosthesis), general personal hygiene, social support, history of compliance with medical treatment, and access to anaplastology services.
IMAGING
Conventional 2D photography and 3D soft tissue imaging is ideal not only for documentation but for virtual design and planning of prosthetic implants.
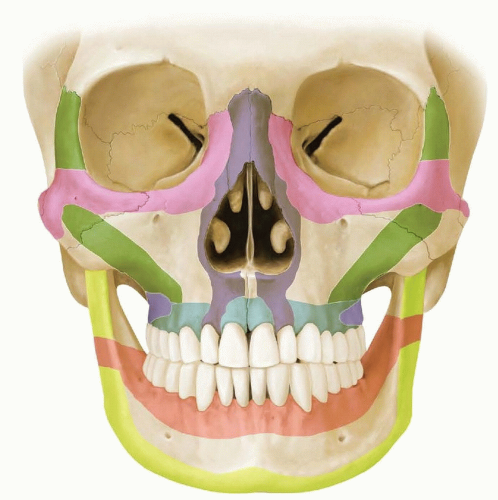
FIG 2 • The craniofacial buttresses (shown in color) are areas of increased bony strength in the facial skeleton, which are the safest locations for implant placement.
For straightforward placement of osseointegrated implants in the temporal/mastoid region in patients with normal bony anatomy, imaging may not be necessary. However, imaging is frequently necessary for symmetrical anatomical restoration and for virtual planning of the implants. CT or CBCT imaging is essential to evaluate bone depth and density, which may be abnormal. Areas of prior bony resection or reconstruction are evaluated carefully for residual bone. Bone quality is of paramount importance after radiation therapy, and abnormal anatomy in craniofacial syndromes should be noted.
Preoperative 3D planning software that integrates the soft tissue and the underlying skeletal anatomy allows the simulated placement of screws into bone to determine ideal vectors and locations of placement (FIG 3). These technologies can be merged with intraoperative stereotactic guidance for particularly challenging cases to ensure optimal placement.6 At our center, we prefer to use a computer-generated guide for precise implant placement7 (FIG 4).
SURGICAL MANAGEMENT
Preoperative Planning
The number of implants to be placed should be decided with an anaplastologist to ensure adequate fixation. This decision will be affected by the location of the prosthesis
as well as the type of fixation (magnet vs bar-and-clip). Magnet fixation may require additional implants to be placed.
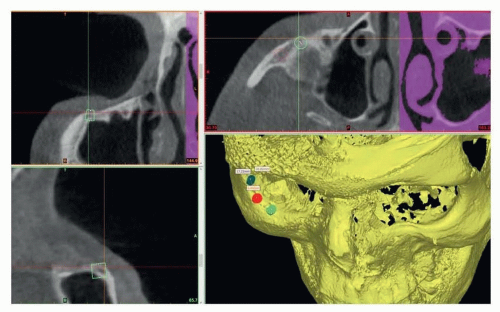
FIG 3 • Three-dimensional virtual planning for ideal implant placement.
FIG 4 • Custom 3D printed drill guide for precise implant placement.
The anaplastologist, with the craniofacial surgeon, will prepare a template of the area to be reconstructed with implant locations designated to guide surgical placement. In the case of the ear, this template is usually made from the position of the contralateral ear and centered around the external auditory meatus or tragus if present.
The implant depth is often decided prior to implant placement but can be decided intraoperatively based on clinical assessment of bone depth and density. Most craniofacial implant systems come in 3 and 4 mm depths.
Positioning
Standard supine positioning with a head drape and general endotracheal anesthesia is used for most implant placements. For uncomplicated implant placement, some surgeons may prefer local anesthesia with sedation.
Hair in the operative area is trimmed in a limited fashion.
If surgical drapes will obscure visualization of a contralateral normal structure, marking should be performed prior to draping to ensure symmetry.
Approach
A one- or two-stage technique can be utilized for implant placement. In a one-stage technique, the implant is positioned and an abutment is immediately placed through the skin. The one-stage approach is appropriate in a majority of scenarios.
In a two-stage technique, skin is reclosed over implants capped with a cover screw. The implants are then allowed to integrate into bone (approximately 3 months). Exposure of implants and abutment placement occurs at a later stage. A two-stage approach is generally indicated if bone is irradiated or of poor quality, in children, or in the orbital or maxillary region.8,9 We typically favor a more conservative two-stage approach for many of our patients rather than early loading of the implant.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree