Delayed Hard Palate Repair in UCLP Patients
Jan Lilja
DEFINITION
In UCLP patients, the cleft palate will lead to speech difficulties.
Poor ventilation of the Eustachian tubes results in a high incidence of hearing problems due to middle ear infection.
Early surgery on the palate may result in reduced maxillary growth.
Late surgery on the palate may result in aberrant speech.
ANATOMY
The palate can be thought of as an anterior bony part limited by the dental arch and a posterior mobile part where muscles, oral mucosa, and nasal mucosa are important functional structures.
The anterior palate (hard palate) is a horseshoe-formed bony structure concave toward the mouth and convex toward the nose where it forms the nasal floor. Both sides are covered by mucosal epithelium.
The muscles in the posterior part (soft palate) will act on the soft palate and produce tension, lifting, or lowering of the soft palate. Lifting of the soft palate is most important and is accomplished by the levator veli palatini muscles. In speech, the soft palate should be lifted as far back as the posterior pharyngeal wall and be able to stop airflow through the nose in order to produce distinct pronunciation of certain sounds.
PATHOGENESIS
In a complete cleft of a unilateral cleft lip and palate, a cleft separates the lip, the alveolar bone, and the hard and soft palate. The lateral incisor on the cleft side is usually missing in both deciduous and permanent dentition. The cleft separates the hard palate lateral to the vomer, establishing a cleft side and a noncleft side in the hard palate where the vomer is attached to the noncleft side. The soft palate is separated in the midline, but the cleft side is usually smaller.
Feeding is often difficult for the child because there is an opening between the oral and nasal cavity. Food may pass into the nasal cavity and sucking is compromised because adequate negative pressure cannot be achieved during breast-feeding.
In the soft palate, the muscles are not attached to each other; the muscles follow an anteroposterior direction along the cleft edges. Some of the muscles are attached to the posterior edge of the hard palate on both sides of the cleft.
This morphological aberration impairs development of speech and hinders ventilation of the Eustachian tube.
IMAGING AND OTHER DIAGNOSTIC STUDIES
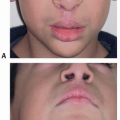
The diagnosis of a patient with complete unilateral cleft lip and palate is usually made by clinical examination.
Photographs taken from anterior, lateral, and inferior views can be taken to document the condition.
In some centers, plaster casts are made from both upper and lower jaws.
Postoperatively, the patients are followed on a regular basis with photos, speech evaluation, cephalometric assessment, and plaster casts.
When needed for evaluation of velopharyngeal incompetence (VPI), nasendoscopy and videofluoroscopy can be used.
SURGICAL MANAGEMENT
There are numerous protocols for operating on the palatal cleft in patients with complete cleft lip and palate. These protocols differ in procedure and timing.
Early surgery of the soft palate is a prerequisite for good speech, but combined with closure of the hard palate, it will produce reduction of maxillary growth.
Closure of the whole palate at an older age will give less problems with maxillary growth but may give more problems with impaired speech.
When delayed hard palate repair is performed in UCLP patients, soft palate closure is performed early to promote speech, and hard palate closure is delayed until 2 years of age to promote growth. The palatal closure is continued over to the oral side, where a pushback procedure can be done within the soft palate.
Closure of the soft palate with a posteriorly based vomer flap will result in anchorage of the anterior part of the soft palate to the base of the vomer flap.
This part of vomer is situated at the insertion of the vomer to the cranial base. The direction of the soft palate will therefore be posterior-upward, resulting in reduction of the openings toward the nose.
This may explain the favorable speech results in our patients, improving the posterior positioning of the levator muscles and thereby reducing VPI.
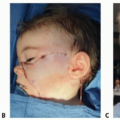
Positioning
The patient is positioned supine on the operating table.
A shoulder roll is placed, serving to tilt the head backward to facilitate visualization.
TECHNIQUES
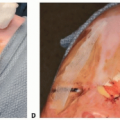
▪ Soft Palate Repair
Incisions begin around the posterior part of the maxillary tuberosities and then follow a zigzag route at the posterior border of the hard palate (TECH FIG 1A).
A posteriorly based vomer flap is dissected, which does not reach the vomero-premaxillary suture anteriorly. The base of the flap lies at the junction of the vomer with the cranial base (TECH FIG 1B).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree