Congenital melanocytic nevi (CMN) are the most common congenital nevi.
They are usually present at birth, but “tardive” CMN may arise within the first 2 years of life.
CMN range from millimeter size to giant, covering the majority of the body.
Implications include risk of melanoma, CNS involvement, and disfigurement.
CMN result in a disturbance of neural crest cell migration between the 5th and 24th weeks of gestation, producing ectopic rests of immature melanocytes.1
This is thought to be related to mutations in NRAS and, to a lesser extent, BRAF oncogenes.2
Nevus cells can extend deep into the subcutaneous tissue, fascia, muscle, and/or periosteum (rare).
Involvement of the leptomeninges or brain parenchyma is known as neurocutaneous melanosis (NCM).
Histologic findings specific to CMN include cell clustering, a round shape, and location within eccrine ducts, in follicular epithelium or blood vessels, and in deeper tissues.
Malignant melanoma may arise within the nevus or in extracutaneous locations, most commonly the CNS.
Population heterogeneity, lack of standardized descriptors, and multiple treatment modalities lead to difficulty ascertaining the true melanoma risk in CMN.
Earlier studies reported lifetime risk of up to 40%.
More recent studies suggest much lower lifetime risk: less than 5% for all patients with large CMN and under 2% for smaller lesions.3
Factors associated with increased melanoma risk include larger nevus size, truncal location, and multiple satellite lesions. The greatest risk may be extracutaneous.
Risk of melanoma arising within a small CMN prior to puberty is extremely low.
The same is not true for large (LCMN) and giant (GCMN) lesions; 50% of those developing malignancy do so within the first 3 years of life.4
To date, there has not been a confirmed case of melanoma arising within a satellite lesion.
Other tumors associated with CMN include lipomas, schwannomas, sarcomas, malignant cellular blue nevus, and undifferentiated spindle cell neoplasms.
Reduction of the risk of melanoma is still viewed as a valid medical indication for excision.
The presence of nevus cells within the leptomeninges, brain, or spinal column is NCM.
Symptoms can range from none to progressive, severe neurologic impairment, hydrocephalus, seizures, and death.
Problems arise from either benign proliferation of nevus cells blocking cerebrospinal fluid flow or malignant degeneration.
Exact incidence is unknown but thought to be around 5%.
Approximately 5% of these patients will be symptomatic, the vast majority developing symptoms before age 3.
Prognosis of symptomatic NCM is poor, with over 90% dying within 3 years of diagnosis.
The highest risk of NCM is thought to be in patients with LCMN of the posterior midline or greater than 20 satellite nevi. These patients should be strongly considered for MRI screening.5
MRI demonstrates shortening of the T1 relaxation time and, less commonly, T2 relaxation time.
For best sensitivity, MRI is recommended prior to 4 months of age due to the lack of myelinization in the newborn.
In patients with symptomatic NCM, aggressive management of the cutaneous lesion needs to be decided on a case-by-case basis and is generally not recommended. This does not hold true for asymptomatic patients, in which the prognosis is more favorable.
Blue nevus
Mongolian spot
Nevus of Ota/Ito
Café au lait spot
Nevus spilus
Sebaceous nevus
Spitz nevus
Several classification schemes have been proposed, most of which use the projected adult size (PAS) of the nevus as the main feature.
PAS is calculated by multiplying the largest diameter of the nevus in infancy by a factor that which varies by anatomical region (Table 1).
Large CMN are considered as any nevus with a PAS of greater than 20 cm or greater than 2% of total body surface area.
Table 1 Projected Adult Size (PAS) of Congenital Nevi in Infancy (Data From Krengel et al., 2012)
Body Area
Projected Adult Size (PAS) Multiplication Factor
Head
1.7×
Neck, trunk, buttocks, arms
2.8×
Legs
3.3×
CMN may arise anywhere on the body.
Large and giant CMN often occur in recognizable patterns or distributions.
Size and extent of involvement vary considerably between patients.
Extensive nevi often involve multiple adjacent areas and/or cross the midline.
Commonly encountered distributions include:
Scalp, forehead, root of nose, and upper eyelid
Face: cheek, nose, and lower eyelid
Trunk (posterior, anterior, or circumferential “bathing trunk” nevus)
Upper extremity (sleevelike distribution)
Lower extremity (as part of bathing trunk or isolated lower extremity)
The surgical management of these patients is tailored to the location of nevus, extent of involvement, and presence of adjacent normal skin.
However, we describe common techniques and principles, many of which may be applicable for the management of nevi in any location.
The example provided in this chapter focuses on a nevus involving the unilateral cheek and lower eyelid (FIG 1).
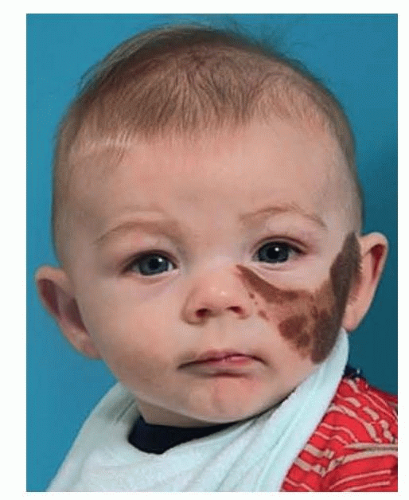 FIG 1 • Facial nevus, involving the unilateral cheek and abutting the lower eyelid. |
Table 2 Proposed New Classification of Congenital Melanocytic Nevi | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||
Patients are often seen in infancy.
Any changes in appearance of the lesion over time should be noted.
Nevus size and location and the presence of multiple satellite nevi should prompt screening for NCM.
A family history of melanoma should be elicited.
Potential psychological problems associated with this diagnosis should not be underestimated, especially in older children and adolescents.
Emotional, behavioral, or social problems are present in 30%.
On initial examination, the extent of the nevus should be noted, including involvement of critical structures and any areas of adjacent normal skin for treatment planning.
Serial examinations every 3 to 6 months are recommended.
Darker pigmented areas or raised nodules may represent neural nevus rather than malignancy.
Selective biopsy can be used to exclude malignancy for any suspicious areas but is rarely indicated if excision and reconstruction are already contemplated.
Treatment of CMN is most often surgical, with excision and reconstruction. Other modalities include dermabrasion, curettage, and laser therapy. Some cases are best approached with observation alone.
Some giant nevi are so extensive as to preclude excision, and regular follow-up by a pediatric dermatologist is recommended.
Although many LCMN are amenable to surgical excision and reconstruction, the surgical experience needed for successful surgical management is not readily available in many areas of the world.
Dermabrasion and curettage are used to reduce, but not eliminate, the number of nevus cells within a lesion.
Dermabrasion is used to abrade away the surface cells within the epidermis and upper reticular dermis.
Curettage separates the cells at a natural cleavage plane between superficial and deep dermis.
Both techniques are best performed within the first 15 days of life.
Lightening of the nevus can be successful initially, but this is variable and the lesion may tend to redarken over time. Follow-up may also show marked hypertrichosis.7
These techniques are theoretically less effective at reducing malignancy risk, due to persistence of nevus cells at deeper levels. Resultant scarring may also complicate surveillance of the lesion. Cases have been reported of melanoma arising within the field of previous dermabrasion.8
Laser remains an attractive option, potentially reducing the level of pigmentation without scarring.
Lasers used in the treatment of CMN include ruby, Q-switched, Er:YAG, and carbon dioxide, either alone or in combination with Nd:YAG or Q-switched ruby lasers.
Serial treatments are required, and scarring can occur with aggressive treatment or improper settings.
Hypo- and hyperpigmentation may also occur and may be transient or permanent.
The disadvantages of laser treatment are similar to those of dermabrasion/curettage and include continued malignancy risk, scarring, difficulties with surveillance, and redarkening of the lesion over time.
Despite their current limitations, nonoperative modalities do offer some benefits in certain situations.
For example, lightening a thin lesion on the eyelid
Improvements in laser technology will likely continue to improve outcomes with this modality, expanding its usefulness in the future.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


