Bilateral Cleft Lip Repair
John A. van Aalst
DEFINITION
A cleft of the lip occurs when the maxillary prominence fails to fuse, first with the lateral nasal prominence and then the medial nasal prominence; when this failure of fusion occurs bilaterally, a bilateral cleft deformity is the result.1
Cleft lip occurs most commonly in patients from Southeast Asia and the southwestern United States (1/250 to 1/400 live births), is less common in Caucasians (1/1000), and is least common among African Americans (1/2000).1
ANATOMY
Bilateral clefts of the lip involve the tissues of the primary palate. This includes the skin, muscle, and mucosa of the lip and the alveolus, extending posteriorly to the incisive foramen.
The premaxillary segment contains the central alveolus (maxilla) with the tooth buds of the central incisors; this bone is attached to the vomer, the bony underside of the septum.
The premaxillary segment presents with variable anterior flaring, which may have variable presentation: it may be very anteriorly positioned or may be correctly positioned within the maxillary arch.
A complete bilateral cleft is likely to have significant anterior flaring, whereas the premaxillary segment of an incomplete cleft is likely to be positioned correctly between the lateral segments of the maxilla.
Gingiva and mucosa cover the bone of the premaxillary segment and then transition to skin; this segment does not contain true lip vermilion. The skin is generally circular in shape and is without a true white roll. No muscle is present in this region (except in incomplete clefts, where the muscle is in continuity with the lateral lip elements).
Lateral segments of a bilateral cleft lip have all of the elements of the lip present lateral to the nasal ala (wet vermilion, dry vermilion, white roll, skin, and muscle); moving medially, the fullness of each of these components diminishes as the lip structures narrow and ascends toward the cleft of the nose.
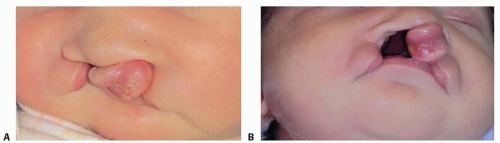 FIG 1 • Infant with bilateral cleft lip. Figure A demonstrates a frontal view of an infant with a bilateral complete cleft lip and palate; the premaxilla is anteriorly positioned (proclined). Figure B is a worm’s eye view of the same infant, demonstrating the asymmetry of the cleft, with the premaxilla positioned more to the patient’s left. As can be noted more clearly in this figure, the patient also has a cleft of the alveolus and palate. |
PATHOGENESIS
Lip fusion occurs on day 42 of gestation.
Fusion may be interrupted secondary to genetic causes (MSX1 gene anomaly), environmental causes (including medications—steroid, anticonvulsants, retinoic acid—alcohol, tobacco use), or a combination of the two (alcohol consumption and cigarette use in the face of an MSX1 genetic anomaly).1
The medial migration of the maxillary prominence is arrested, leading to failure of fusion with the medial and lateral nasal prominences; failure of fusion of these latter two leads to clefting of the nostril floor.
PATIENT HISTORY AND PHYSICAL FINDINGS
Many children with bilateral cleft lip will be diagnosed in utero, prompting a prenatal visit with cleft team members, including the surgeon. The cleft team member describes the concept of team care to the family, the needs of the child immediately following birth, and the surgical preparation for cleft lip repair at approximately 3 months of age.
Patient history should include the presence of family members with clefting; maternal exposure risks: cigarette and alcohol use; medications, including anticonvulsants and steroids; and folic acid supplementation during early pregnancy.1
Following delivery, the first visit to the surgeon is generally within the 1st week of life.
In addition to a full physical examination, the tailored examination of the face detects whether the cleft is complete or incomplete, whether there is asymmetry between the two sides, and whether the premaxilla is proclined (FIG 1). In addition, the presence of clefts of the alveolus and of the palate must be documented.
IMAGING AND OTHER DIAGNOSTIC STUDIES
No routine imaging studies are required for children with bilateral cleft lip prior to surgical repair.
Because these children may have other congenital anomalies, additional findings on physical examination will dictate the need for additional diagnostic studies.
If the child has evidence of breathing difficulties, or sleep apnea, a sleep study may be warranted. If there is any evidence of feeding/swallowing difficulties with concerns about aspiration, a swallow study may be warranted; if other cranial abnormalities are present, a craniomaxillofacial computed tomography scan may be warranted.
NONOPERATIVE MANAGEMENT
Although nonsurgical management of the bilateral cleft lip is not appropriate, presurgical management for control of the proclined maxilla is recommended.
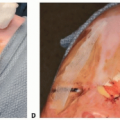
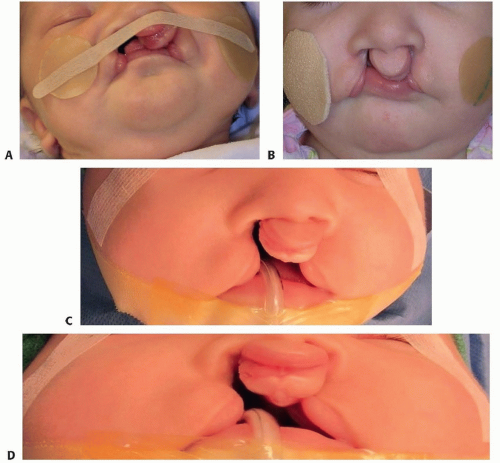 FIG 2 • Preoperative preparation of the patient in FIG 1 with a taping regimen. This taping regimen needs to start shortly after birth to maximize the effect on premaxillary segment retroclining (an early start is also true for other forms of presurgical orthopedics, including nasoalveolar molding). A. During the taping regimen. B. At completion of the taping regimen. C,D. Immediate preoperative photographs demonstrate an improved position of the premaxilla in a more symmetrical position after taping regimen. |
SURGICAL MANAGEMENT
Children are judged ready for surgery using the rule of 10s: approximately 10 lb (4.5 Kg), 10 week of age, and a hemoglobin count of 10.6,7,8
If there are any other symptomatic comorbidities or concerns about appropriate weight gain, delay in surgery is warranted.
Positioning
At the time of surgery, the child is positioned in the supine position and intubated with an oral Ring-Adair-Elwyn (RAE) tube (FIG 3A).
A shoulder roll is placed to obtain gentle extension of the neck.
The entire face is prepped and draped, and a throat pack is placed.
Markings are made for lip repair with tattooing of key landmarks (TECH FIG 1).
Local anesthetic with epinephrine is injected following the markings.
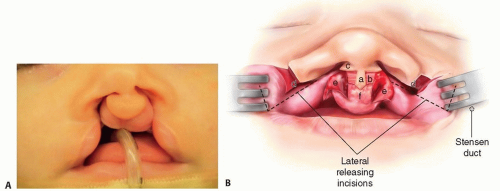 FIG 3 • A. The patient is positioned supine and intubated with an oral RAE tube, with taping on the chin so that the upper lip is not distorted. B. Landmarks. The central philtral column with skin (a) is 2 mm wide at the waist and 2 mm from low to high point of Cupid’s bow. The lateral flanking de-epithelialized regions (b) are also 2 mm wide. The remnant skin and mucosa of the premaxillary segment have been incised into three parts. These areas are labeled (e) bilaterally and (f) centrally and inferiorly. At the superior philtral column (b–a–b) are extensions of skin (c) that will be eventually be used to close the floor of the nose. The central flap (f) is used to reconstruct the central upper buccal sulcus; the two lateral flaps (e) are turned out laterally and used to reconstruct the anterior surface of both alveolar clefts. Bilateral upper buccal sulcus incisions (d) allow medialization of cheek tissue to minimize tension at final closure. The vertical component of the incision is made medial to Stensen duct (the greater the height of this incision, the greater the capacity to medialize cheek tissue). The horizontal incision is made at the junction of the gingiva and oral mucosa to the base of the L flap (without injuring the L flap). A Freer elevator is used to lift the periosteum from the maxillary surface, exposing the infraorbital nerve. The region of the nerve is the most significant area of tethering, which prevents medial movement of cheek tissue. The periosteum medial and lateral to the nerve is cut vertically, avoiding injury to the nerve and releasing the tethering effect of the periosteum. |
TECHNIQUES
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


