Symmetric pocket formation and meticulous implant carving are the most critical parts of nasal dorsal augmentation using implants. Innovative three-dimensional printed nasal implants can exactly fit the nasal dorsal contour, decreasing the chance of deviation and malpositioning. Vertically oriented folded dermal graft technique can avoid the high resorption rate of conventional dermofat grafts. Multilayered costal cartilage graft technique for dorsal augmentation can minimize warping and difficulty in the graft carving. Derotation graft allows supple and movable nasal tip while enabling enough tip lengthening, even if the septal extension graft is the most commonly performed procedure for short nose correction.
Key points
- •
Implants for dorsal augmentation should be placed under the periosteum and the caudal end of the implant should be placed at the supratip area.
- •
Three-dimensional printed nasal implants can exactly fit the patient’s nasal dorsal contour, decreasing the chance of deviation and malpositioning.
- •
Vertically oriented folded dermal graft and block costal cartilage are the choices of autogenous material for major dorsal augmentation.
- •
Derotation graft allows supple and movable nasal tip while enabling enough tip lengthening, even if the septal extension graft is the most commonly performed procedure for short nose correction.
Nasal dorsal augmentation
Low nasal dorsum is one of the main characteristics of Asian noses. Thus, nasal dorsal augmentation is one of the most frequently performed rhinoplasty procedures in Asian countries.
Materials used for dorsal augmentation are divided into implants and autogenous tissues.
There is no doubt that the autogenous tissues are superior to the implants in the aspect of complications. However, autogenous tissues have disadvantages of lesser satisfaction aesthetically, donor site morbidity, and tissue resorption. Thus, implant is still the preferred material for dorsal augmentation in Asia.
Nasal dorsal augmentation using implants
Because of the thick skin envelope of Asian noses, as opposed to that of Westerners’ noses, implant showing through the skin or skin thinning and redness after dorsal augmentation with implant is considerably less likely than in white patients.
A high-quality implant carved accurately to match dorsal contour, if placed in the appropriate surgical plane under the correct surgical technique, can minimize the chance of adverse effects and bring esthetically beautiful results for Asians who have thicker skin.
The most commonly used alloplastic implant for Asian dorsal augmentation is silicone implants, followed by expanded polytetrafluoroethylene (e-PTFE) implants. ,
Operative techniques
Marking for Implant Placement
The cephalic starting point of the implant is determined individually, but implants are usually placed between the double eyelid line and the upper pupillary line ( Fig. 1 ).
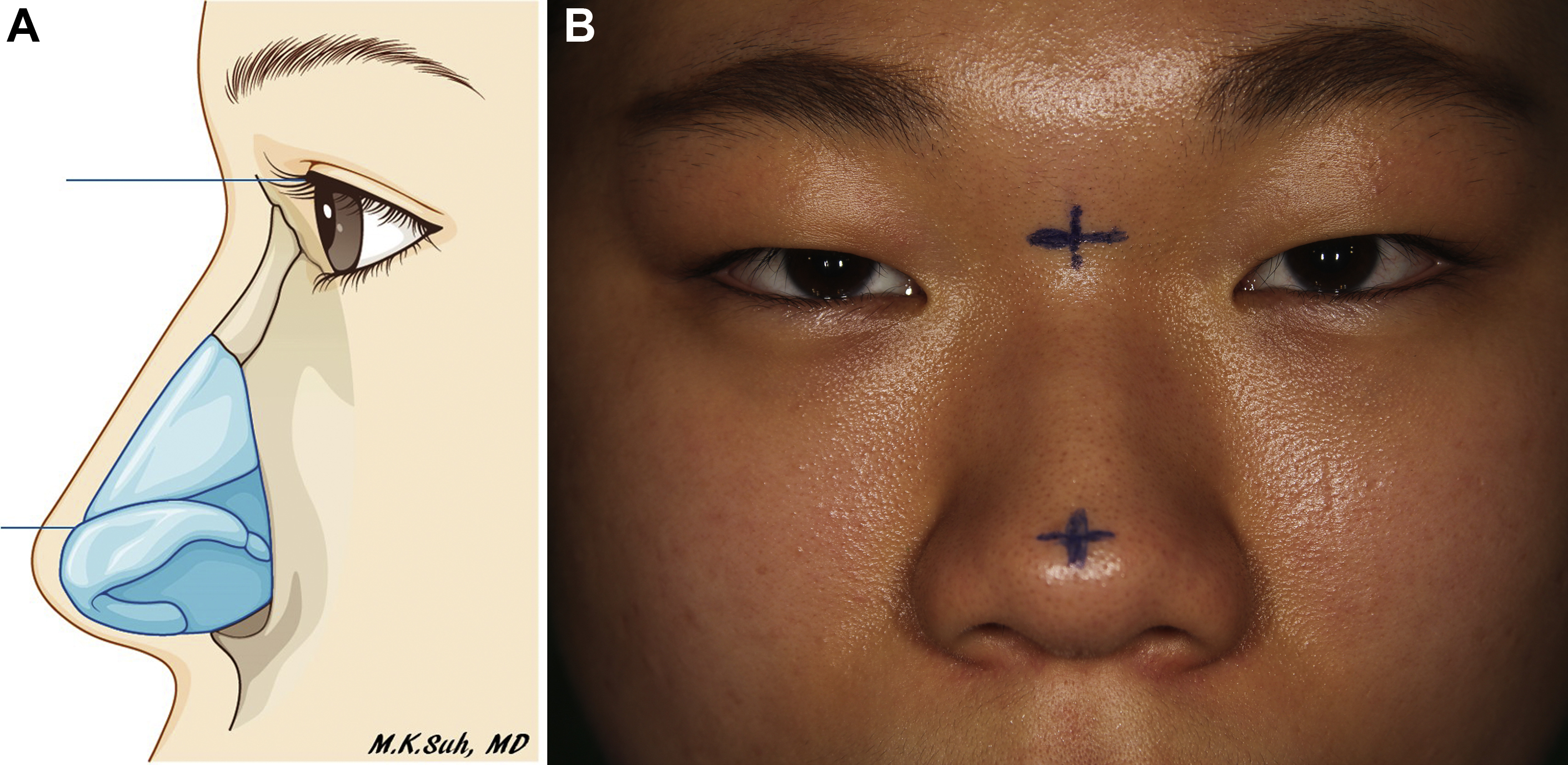
The face may look longer and older after nasal dorsal augmentation in the long face, so it is necessary to set the starting point of the implant to a caudal position and to lower the implant height.
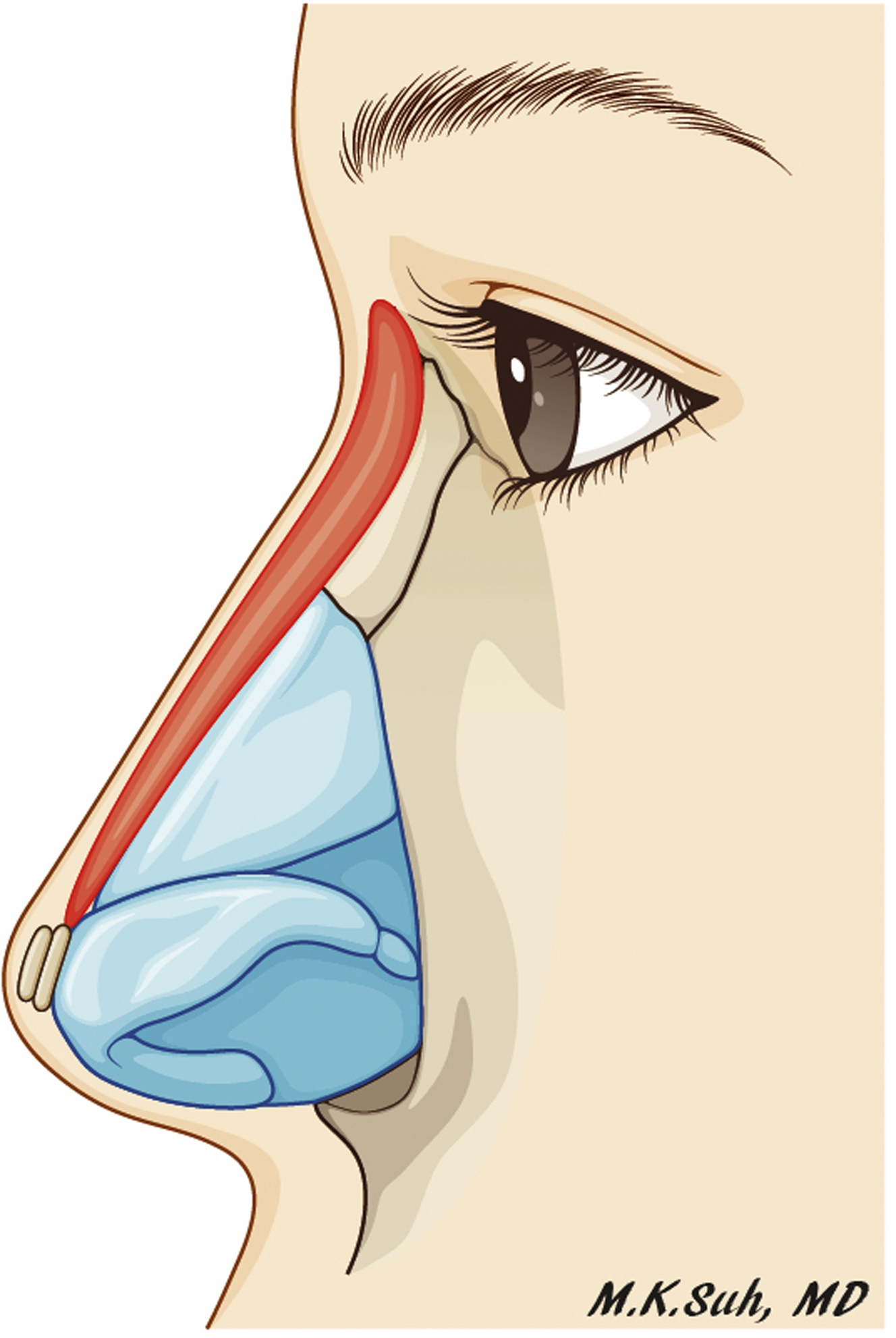
Implant use is limited to dorsal augmentation. Tip projection should be done with a variety of tip plasty techniques, including suture techniques and cartilage grafts. It is safe to use the implant only from the nose to supratip area ( Fig. 2 ). Long or L-shaped implants should not be used.
Carving an Implant
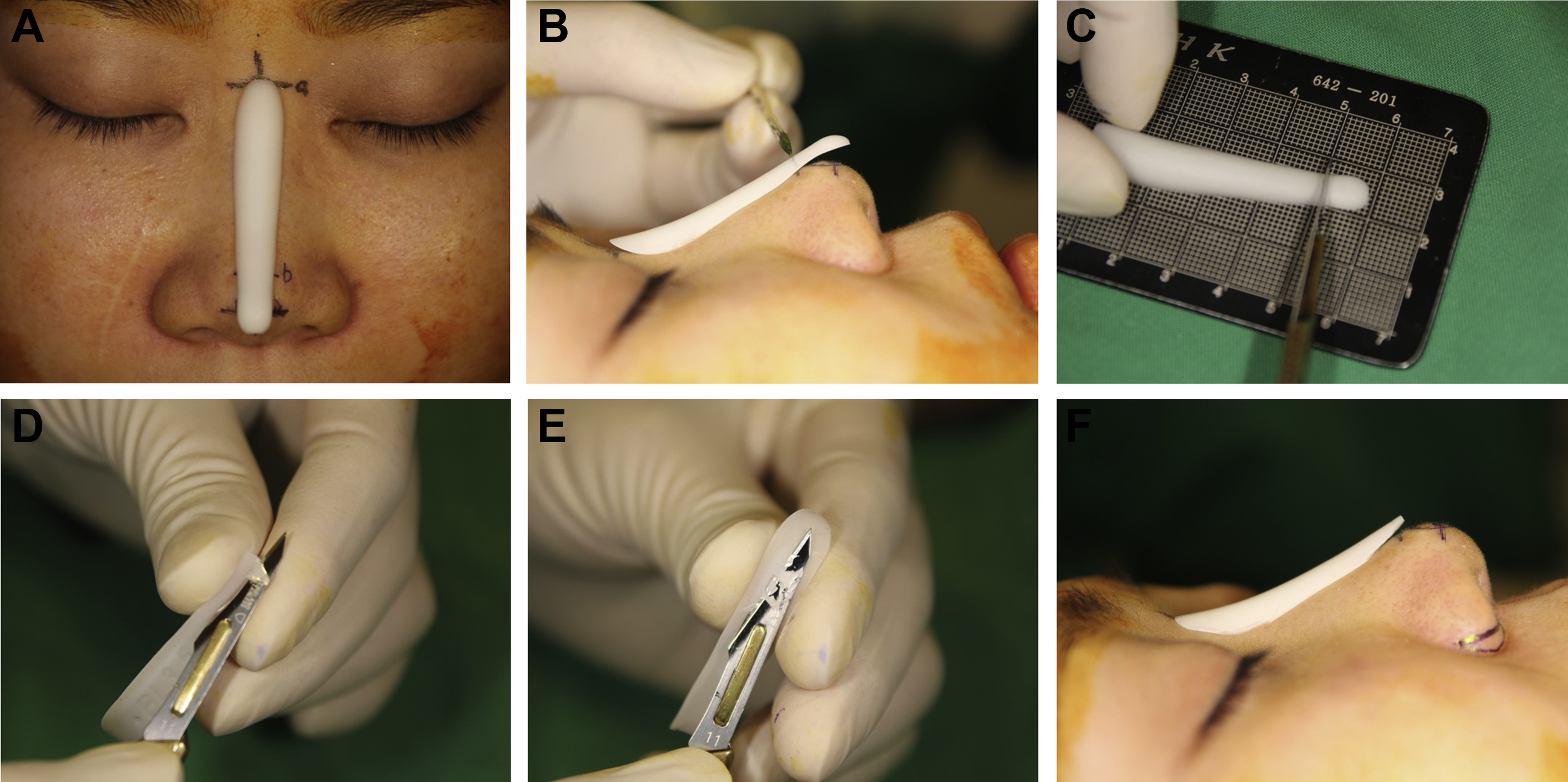
The procedure for an implant carving is as follows ( Fig. 3 ):
- 1.
Among various types of implants with various heights, widths, and curvatures, the operator chooses the most appropriate implant that fits the dorsal contour and the desired height/shape of the patient.
- 2.
Implant is placed on the nasal dorsum, the cephalic part of the implant being placed on the point marked on the radix, and then the caudal ending point of the implant is marked.
- 3.
The marked distal end of the implant is cut, and then the thick distal end is thinly carved.
- 4.
The bottom of the implant is carved and trimmed to match the contour of the dorsum.
Dissection
A dissection to form a straight and symmetric pocket is the most significant part of dorsal augmentation.
Dissection is performed above the perichondrium in the lower lateral and upper lateral cartilages (supraperichondrial plane) and under the periosteum in the nasal bone area (subperiosteal plane). Implant should be placed under the periosteum to avoid movable implant and to decrease visibility of the implant through the skin. Metzenbaum scissors are used for the dissections over the lower and upper lateral cartilages. It is important to make sure a maximum amount of the soft tissue is included in the skin envelope ( Fig. 4 ).
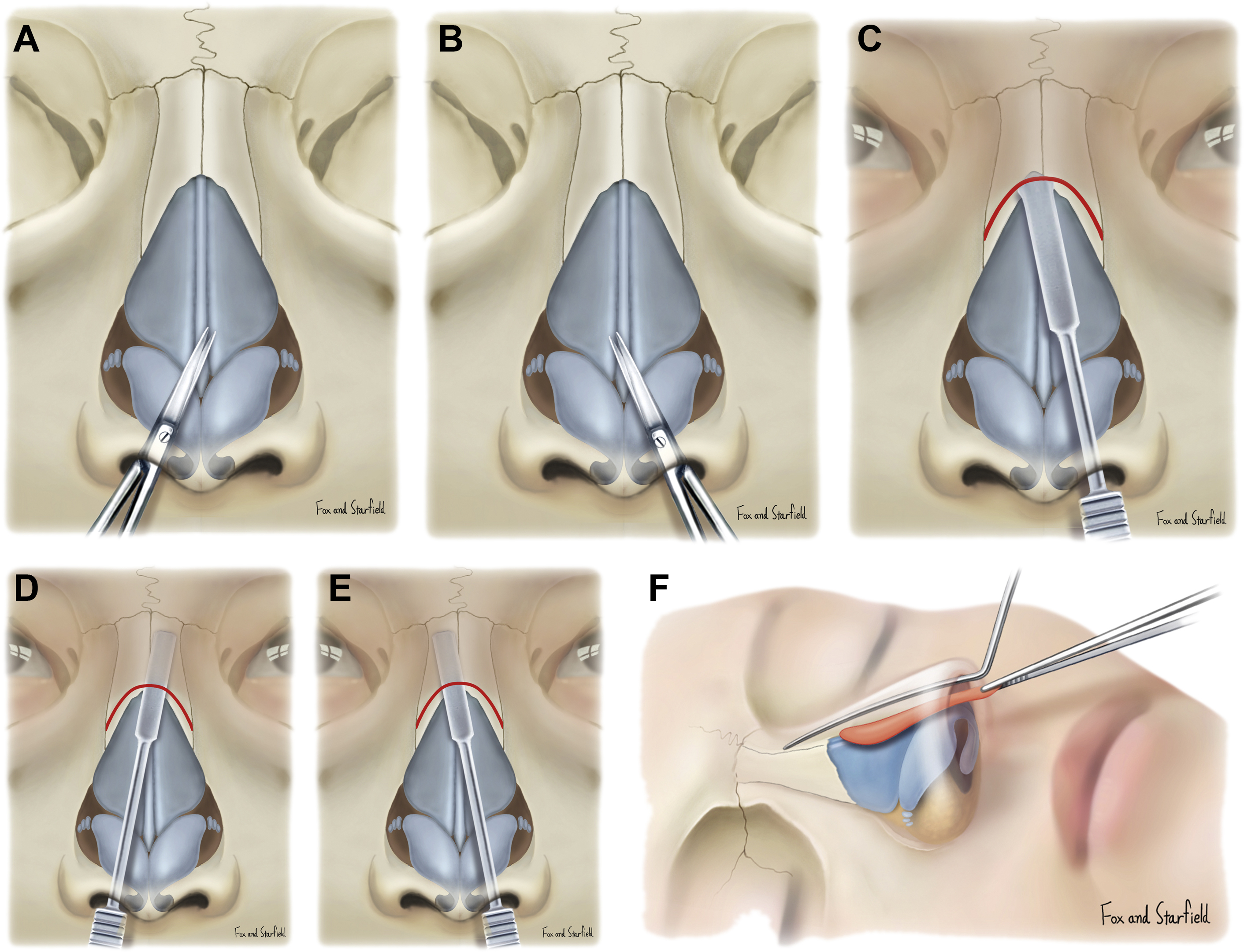
A Joseph knife is used to make incision on the periosteum transversely about 1 mm above the inferior margin of the nasal bone. Then, a Joseph elevator is used to elevate the periosteum.
Dissection and pocket formation are performed through the bilateral incision to ensure a symmetric pocket. Regarding pocket size, this author recommends a slightly larger pocket size than the width of the implant.
After pocket formation, irrigating the pocket with a povidone-iodine solution mixed with an antibiotic is helpful for the prevention of infection.
Implant Insertion
Implant is placed in the center of the pocket without deviation to one side. There is no need to fix the caudal end of an implant. However, when the operator is not sure of the straight symmetric implant positioning, then suturing the caudal end of implant to the septal angle may be helpful.
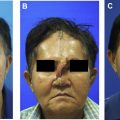
Fig. 5 shows an example of dorsal augmentation using implants in a male patient.

Augmentation rhinoplasty with three-dimensional printing technology
Recently, three-dimensional (3D) printing technology has gained traction in the medical fields. With the rapid growth of 3D printing technology, the paradigm shifted to patient-specific treatment, giving surgeons the opportunity to plan and apply more precise and visible surgery by designing patient-specific medical devices.
Before 3D printing technology, surgeons had to create the shape of the implant they wanted to use, and they had to further process (carve) the ready-made products to suit the patient’s nasal dorsum at the intraoperation step.
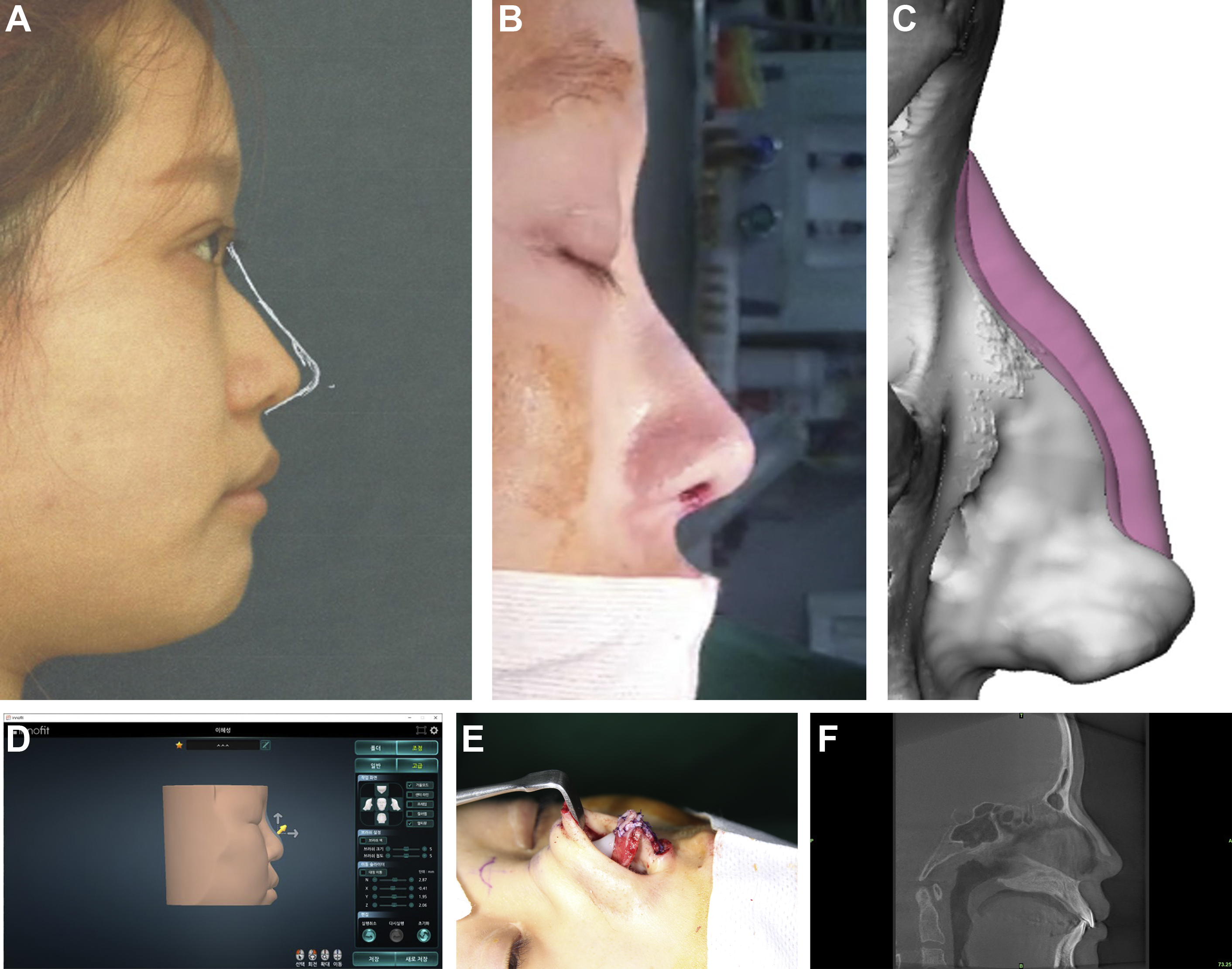
However, 3D printing technology allows surgeons to produce the implant desired by the surgeon at the preoperation step, without the need for carving at the operation step. Implant contour reflecting the asymmetry and irregularity of the nasal bone and upper lateral cartilages can be produced through this technique. It can also reflect the other surgical plans, such as osteotomy, cartilage graft, and lower lateral cartilage realignment ( Fig. 6 ). Patients can participate in the determination of the desired height and profile line before surgery through the simulation program.
Design and Manufacturing Process
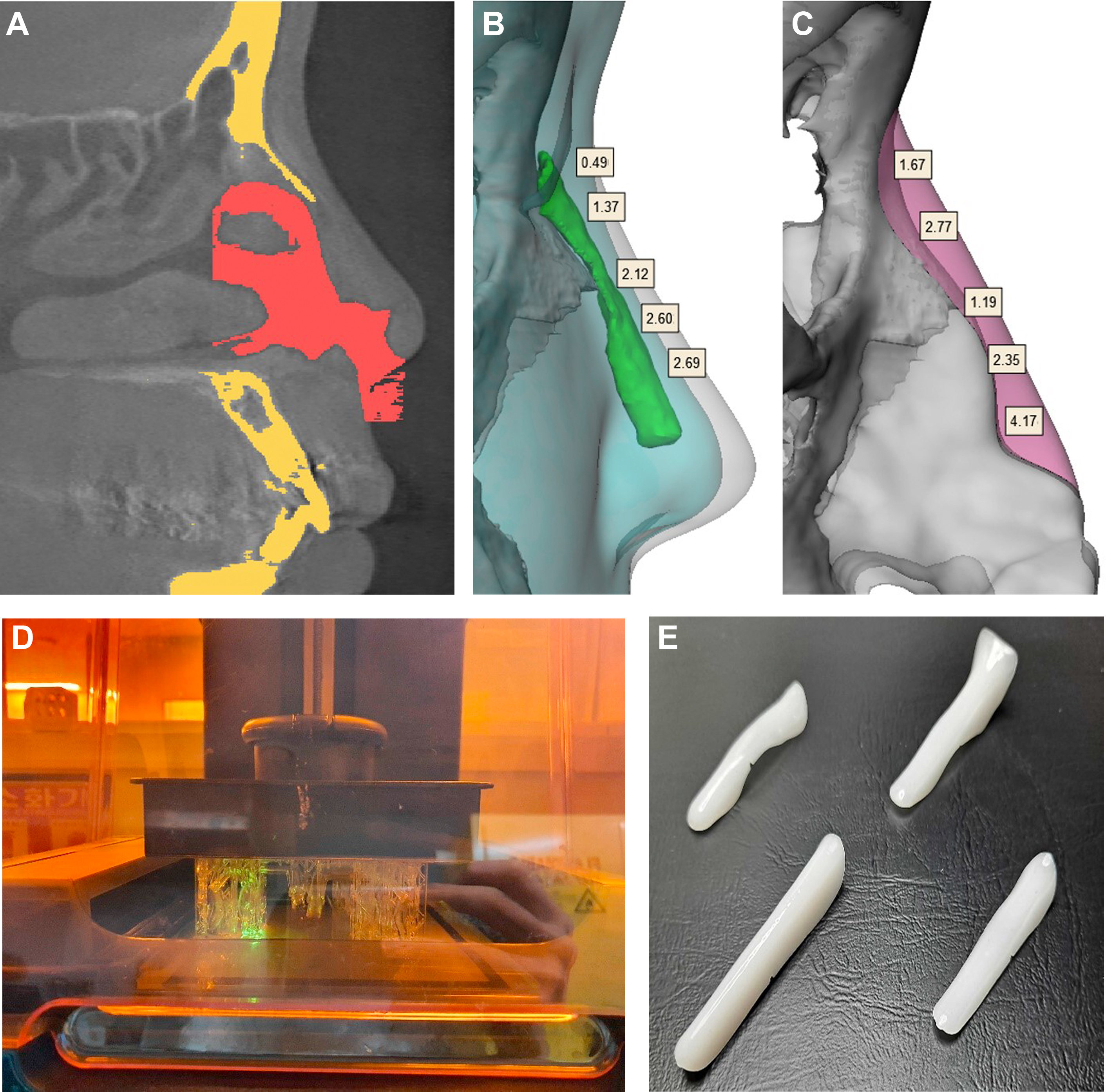
Patient-specific nasal implants for augmentation rhinoplasty are manufactured in the following 5 steps ( Fig. 7 ):
- 1.
Medical images of the nose are acquired through computed tomography or MRI.
- a.
It must be possible to obtain 3D information of human tissue from medical images.
- a.
- 2.
Segment a specific part from the medical image and infer the side where the implant is inserted.
- a.
Divide the skin, the bone in the region (including the nasal bone and the orbital bone), and the nasal cavity.
- b.
It can be segmented using snake algorithm and U-net deep learning algorithm.
- c.
Because most medical images are not of adequate quality to segment nasal cartilages, they are inferred through medical statistical analysis and deep learning.
- a.
- 3.
Computation of the implant volume required for predicted outcome after surgery.
- a.
Predicted outcome after surgery usually refers to two-dimensional information in which the outline of the expected shape is drawn on a picture taken from the side or the back.
- b.
Using virtual plastic surgery technology, 3D information on the predicted outcome can be obtained, which means more accurate information on the predicted outcome.
- a.
- 4.
Design an implant that reflects the surgical plan and the doctor’s request form.
- a.
For example, when glabellar-radix augmentation is required, a long implant capable of glabellar augmentation can be designed.
- b.
The width or angle of nasofrontal slope of the implant can be designed as desired by the doctor.
- a.
- 5.
The implant is fabricated using a 3D printer.
Three-way communication between patient, doctor, and manufacturer is required in patient-specific nasal implant fabrication.
- 1.
In cosmetic surgery, it is important to express what the patient wants.
- 2.
The manufacture of patient-specific nasal implants is the result of both the patient’s desire and the doctor’s surgical plan ( Table 1 ).
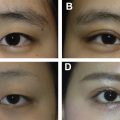
Fig. 8 shows preoperative and postoperative results of nasal dorsal augmentation using 3D printed nasal implant.
Advantages and Disadvantages of Three-dimensional Printed Nasal Implant
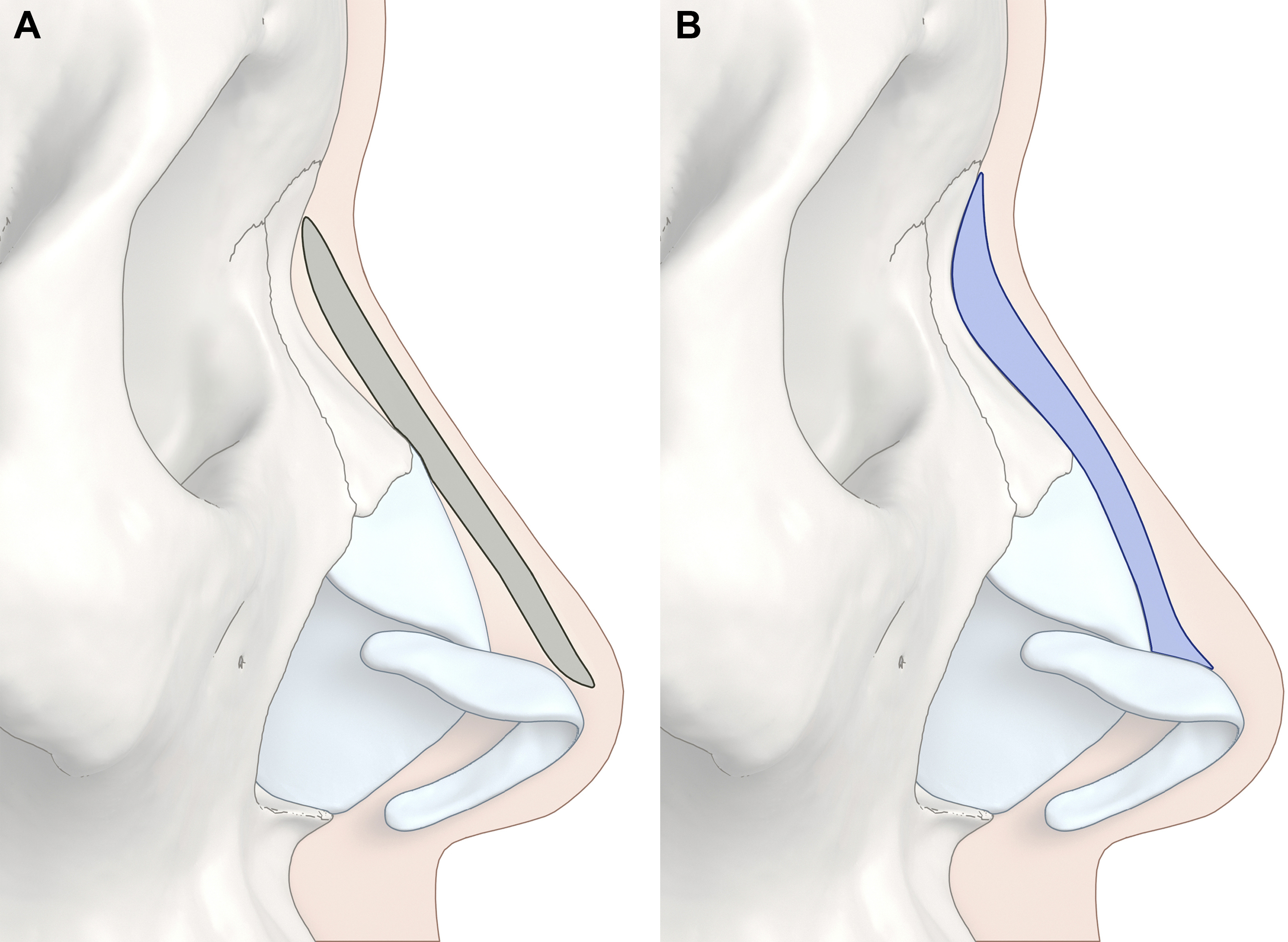
Advantages of 3D printed patient-specific nasal implant are as follows: first, implants that exactly fit the patient’s nasal dorsal contour can be manufactured ( Fig. 9 ). The implant is manufactured to match the contour irregularity of nasal bone and upper lateral cartilages, and also reflects the nasal dorsal asymmetry. Therefore, implant carving is unnecessary or significantly reduced compared with ready-made implants. In the intraoperation process, the time and effort required to carve an implant can be significantly reduced.
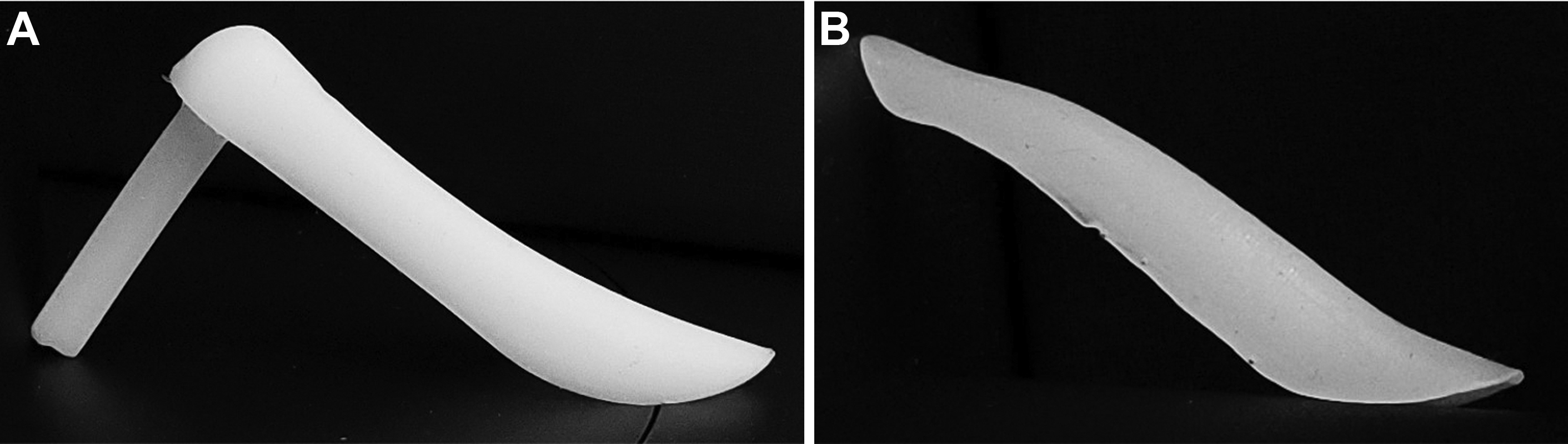
Because the shape of the implant is consistent with the patient’s nasal dorsal irregular contour and asymmetry, it is expected that the possibility of implant deviation and migration can be reduced. Because the dead space between the implant and the underlying nasal framework is minimized, it is speculated that the chance of thick formation of posterior capsule and resulting capsule contracture is also minimized.
Second, patients can participate in simulation surgery and making the desired implant through a virtual plastic surgery application.
Nevertheless, the disadvantage of this technique is that it takes several days for the implant to be manufactured before surgery.
Nasal dorsal augmentation using autogenous tissues
Autogenous tissues are appropriate for dorsal augmentation in patients with extremely thin dorsal skin, and in secondary operation for implant-related complication, such as dorsal skin redness and thinning, or capsular contracture.
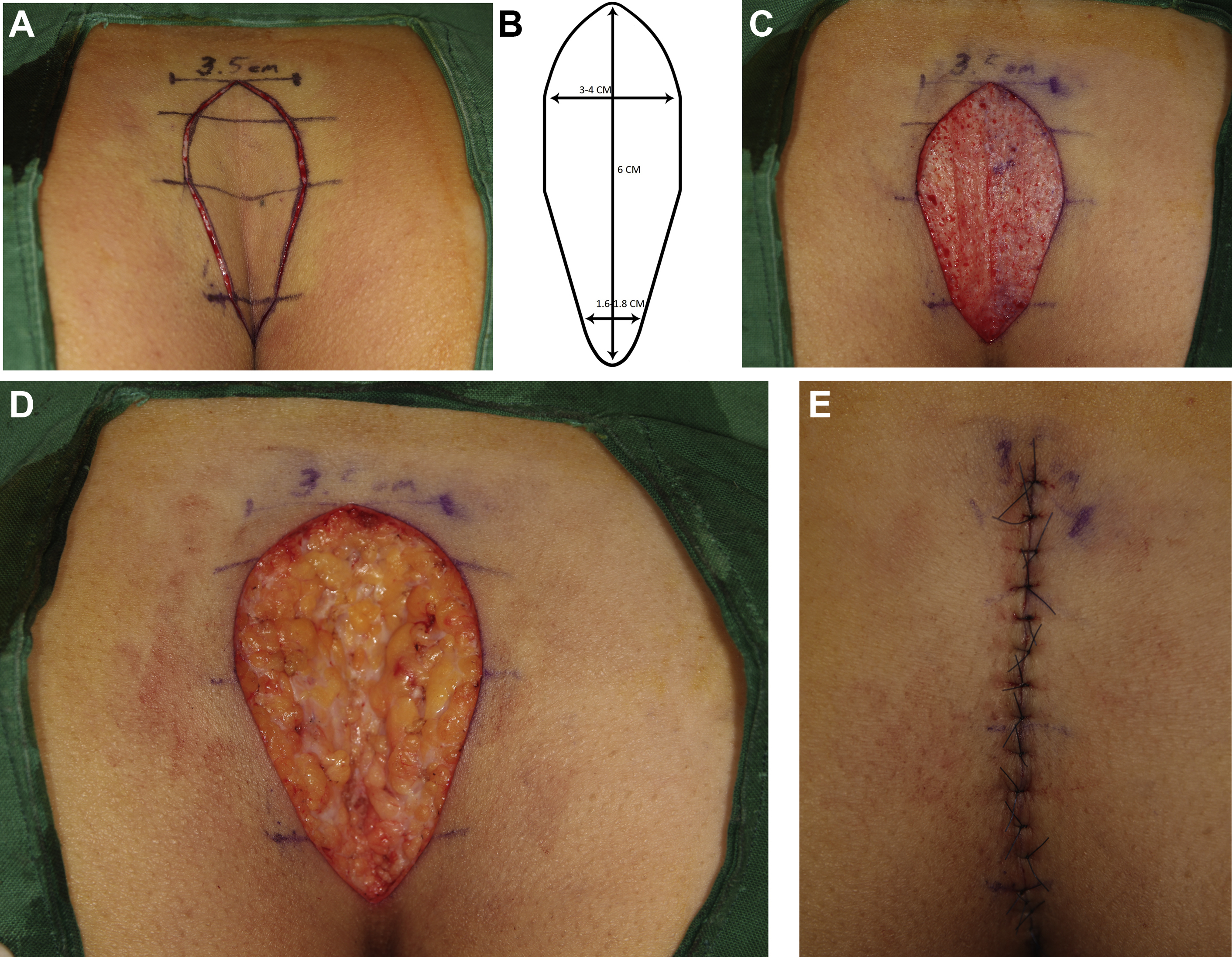
Dorsal augmentation with vertically oriented folded dermal graft
Resorption of generally performed dermofat graft occurs in both the dermal layer and the fat layer, but more resorption takes place in the fat layer. Therefore, it is important to minimize the thickness of the fat layer and increase the thickness of the dermal layer in order to keep the maximum height of the graft. However, because the thickness of the human dermis is limited, a new technique to overcome this is the vertically oriented folded dermal graft technique.
This technique contains minimal fat in the graft, and is mainly a technique of dorsal augmentation using dermal components.
Graft Design
As shown in Fig. 10 , the graft is designed on the sacrococcygeal area. The caudal margin of graft is located 2 cm superior to the coccyx. The cephalic portion of the graft needs to be wider for greater augmentation of the radix area.