Anatomy
The anatomy of the eyelid and midface has been well described in Chapter 1 .
While the lower eyelid and the cheek are two separate cosmetic units that are separated by bone to skin adhesions, a smooth transition between them is a feature of a youthful face and thus a desired outcome as we approach the rejuvenation of this region. Both the eyelid and the cheek areas have their own subunits that respond differently to the process of aging resulting from fat loss, muscle attenuation, fluid retention, bony resorption, and the retaining ligaments that unite and subdivide them, not to mention the changes in the overlying skin that loses its elasticity, pigmentation, and texture, thus accenting the visible signs of aging of these regions. Each factor in the aging process, whether together or independently, leads to a cascade of events that manifest themselves through the hallmarks of the eyelid and cheek aging.
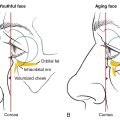
Fat herniation from the suborbital compartments causes the thin overlying eyelid muscle (orbicularis oculi muscle) to become more lax and prolapse, a factor improved when it is contracted during squinting and aggravated when aging leads to bone resorption. It manifests as orbital socket enlargement that is more pronounced in Caucasians and very minimal in Asians. The aging orbital expansion occurs in a diagonal vector superomedial to inferolateral ( Fig. 10.1 ). This causes the eyeball to sink deeper in the socket, further prolapsing the suborbital fat pads anteriorly, which when combined with maxillary bone resorption produces a negative vector ( Fig. 10.2 ).

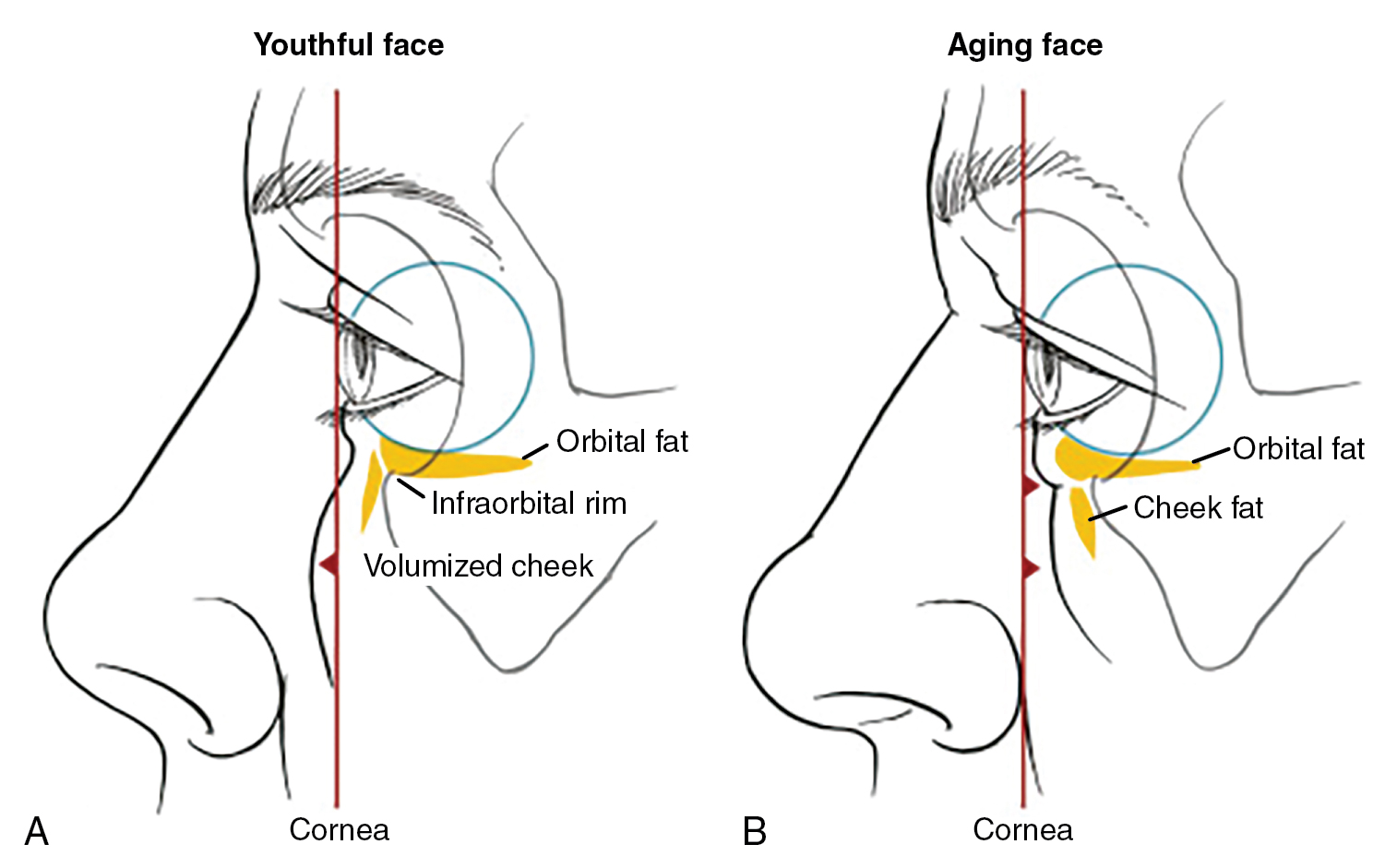
Depending on the bone structure and age of the patient, the lower eyelid fat herniation may appear either as a discrete bulge directly over the infraorbital hollow or as an abdominal pannus where the fat, muscle, and fibrous skin herniation drapes over the infraorbital bone, confusing the surgeon as to the source of the lower eyelid bags. The upper cheek skin, immediately below the eyelid skin, manifests itself in its most dramatic aging of the lower eyelid as festoons (see glossary below, Figs. 10.3 and 10.4 ). This area represents edematous tissue trapped between the superior and inferior lamellae of the orbital retaining ligament ( ORL —see glossary below). The lower lamellae of the ORL are further supported medially by the zygomatico-cutaneous ligament ( ZCL —see glossary below). The ligamentous bands of the ORL fuse medially to form one band called the tear trough ligament ( TTL —see glossary below) ( Figs. 10.3 , 10.5 , and 10.6 ). The ORL then splits into two main bands (lamellae) beginning a bit medially to the midpupillary line (see Fig. 10.3 ). The separation of the two lamellae becomes widest (∼7 mm width) at about 7 o’clock from the midpupillary line, accounting for the almond shape of the festoons as they extend over the orbital rim, ending just lateral to a vertical line drawn from the lateral canthus (see Fig. 10.3 ). Since both the ORL and ZCL ligaments form an impregnable wall to water stretching from skin to bone, any accumulated fluid in this upper cheek/lower eyelid skin area has no place to drain inferiorly, leading to continuous stretching of the tissue (skin, fat, the deep orbicularis oculi muscle fibers, and the lateral and medial SOOF ( suborbicularis oculi fat —see glossary below), that together comprise and shape the festoons (see Figs. 10.3–10.6 )




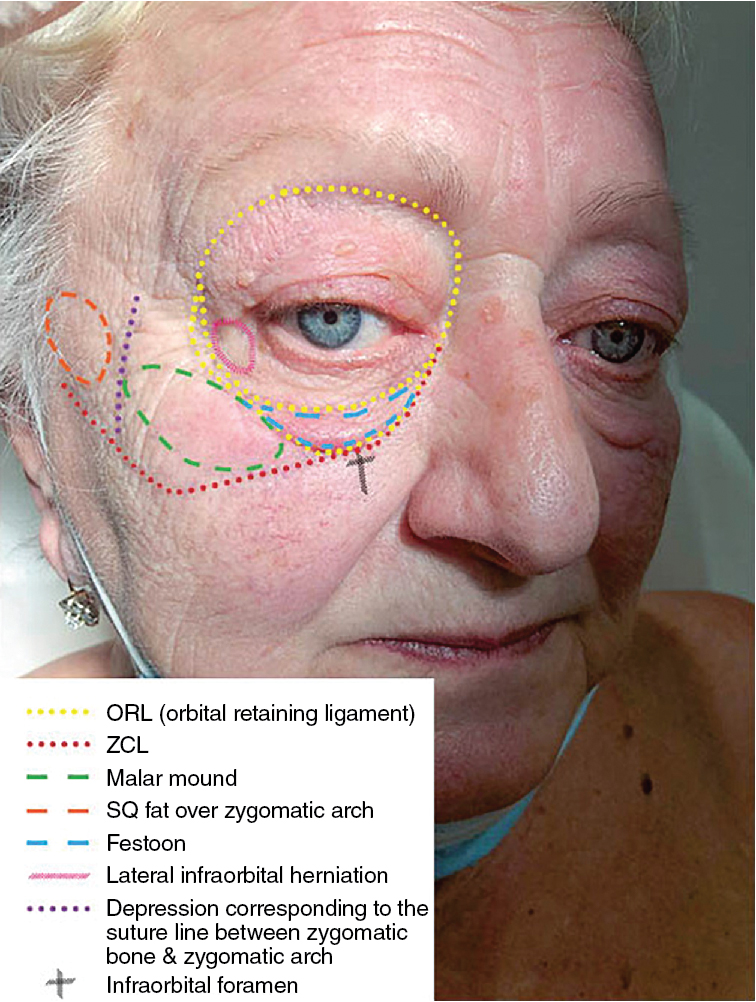
The anatomical location of the different components of the eyelid can be localized in a manner of the dials on a watch in relation to the pupil that serves as a central reference point (see Fig. 10.3 ). The position, width, and course of the orbital retaining ligament (ORL), with its medial fusion into a single fiber called the tear trough retaining ligament ( TTL ) and its lateral bifurcation into two lamellae/fibers responsible for the water impregnable bands that prevent egress of local edema and the subsequent stretching of its layers (skin, superficial fat, orbicularis oculi muscle, and SOOF (with its medial and lateral compartments) resulting in the appearance of festoons, is illustrated above in an off-white color. The three orbital fat pads are represented by the three solid colored yellow ovals superior to the ORL .
Care must be taken not to injure the Inferior oblique muscle that tracks between the Medial and middle fat pads (see Fig. 10.3 , between 4 and 5 o’clock). The inferior oblique is most susceptible to injury during the transconjunctival approach.
The nasojugal fold widens with age due to the inferior drooping and loss of the underlying superficial medial cheek fat pad and medial maxillary bone resorption, giving the appearance of a wider indented triangular depression (see dotted yellow triangularly shaped line) and the ZCL (outlined as a green line) showing its accentuation of the malar mound and its added support for the lower lamellae of the festoon that occasionally merges into, and hangs over, the malar mound (see Fig. 10.5 ).
The outlines of the eyelid and cheek boundaries become more pronounced as the bone resorbs, pulling on the ligaments ( ORL and ZCL ) that stretch from the bone to the skin. As the inferior orbital rim and maxilla are pulled further posteriorly and inferiorly (as part of the bone resorption seen with aging (see Fig. 10.1 ), the dermis is also pulled with it, further etching and widening the demarcation lines of the tear trough deformity , the palpebromalar groove (see glossary below), the nasojugal fold (see glossary below), as well as the submalar fold (see glossary below) (see Figs. 10.3 and 10.4 ,  ).
).
The ZCL has different forces pulling on it along its path. Medially, the central maxillary bone resorbs faster in a posterior inferior direction, causing the bowing central appearance of the nasojugal fold/crease/groove (a.k.a. mid-cheek groove ) (see Fig. 10.5 ). Laterally, the lateral-cheek, malar (zygomatic) bone, undergoes a much slower resorption giving rise to the pronounced malar mound [malar eminence] —see glossary below). This malar mound becomes more noticeable since not only the medial cheek bone deflates but also its overlying fat involutes (see Fig. 10.4 A–D,  ).
).
The interplay of anatomy, its aging, and a consensus on terminology is critical to understanding the process of aging. In this chapter, we hope to share with you the formulation of a comprehensive and reproducible approach for rejuvenating this area in a natural and safe way. As we reviewed the literature in preparation for this chapter, we noticed similar names given to different anatomical landmarks. To avoid the confusion and help best address the rejuvenation process, we must use the same terminology.
Thus, a brief review and glossary of essential terms and their other common names encountered in the literature is included below:
Orbital Retaining Ligament (ORL) — ORL is also referred to, in some papers, as orbitomalar ligament (OML) , tear trough orbicularis retaining ligament complex, and malar septum (the latter a completely different entity). It is a ligamentous fibroelastic tissue connecting the periosteum (originating 2 to 3 mm below the infraorbital rim, although its uppermost fibers originate usually from the Arcus Marginalis, a junctional area between the periosteum and the orbital septum, to the dermis and piercing in its path superiorly and inferiorly the palpebral and orbital portions of the orbicularis oculi muscles. The ORL manifests visually as the tear trough deformity medially (see Figs. 10.3 , 10.5 , and 10.6 ); some further subdivide this part of the ligament calling it the tear trough retaining ligament ( TTL ). As the ORL extends laterally from the midpupillary line it divides into many small fibers with two more distinct thick fibers called the upper and lower lamellae (see Figs. 10.3 , 10.5 , and 10.6 ). The dermal insertion of the ORL defines the end of the preseptal orbicularis oculi muscle as it dives deeper with its orbital portion, the latter finding its border (with an exception of a few fibers that track further down into the upper lip and corner of the nose) at the inferior most fibers of the ORL as it interlaces, part of its way, with the fibers of the ZCL (see Fig. 10.3 ). The ORL has insertion along the upper (not only lower) orbital rim, separating the upper eyelid from the forehead in a crease hidden by the brow (see Figs. 10.5 A and 10.6 ). As it wraps along the lateral orbital rim, the ORL contributes laterally to the lateral orbital thickening. Its fibers become more layered, complex and thinner laterally (thus being more tenuous and stretching more), and thicker and fused medially as it curves up to form the TTL that inserts at the medial canthal tendon. Based on recent three-dimensional micro-computer tomography results of the ORL , it appears that the ORL is composed of two or more distinctly thicker band layers separated from one another by 4 to 8 mm space. The ORL appears as a broadly extended ligamentous process with tree-like arborization on sagittal sections and plexiform plates on a 3D morphology, reminiscent of the inside of a puff pastry. These fibers reach into the orbicularis oculi muscle as well as below it into the pre-zygomatic region with lateral insertion points in the zygomatic skin and the lateral canthal tendon. As we age, the ORL often takes the form of a V-shape deformity in its central path, tracking superolaterally to form palpebromalar groove , medially to fuse into the tear trough ligament that forms the tear trough deformity and inferiorly interlacing with the ZCL to form the nasojugal fold/groove (see Figs. 10.5 and 10.6 ).
Zygomatico-Cutaneous Ligament (ZCL) —defines medially (together with the inferior ORL fibers) the inferior limit of most of the deep fibers of the orbital orbicularis oculi muscle (some fibers of this muscle continue to insert into the corner of the nose and upper lip and form a boundary preventing fluid from passing through. The ZCL thus supports the lower ORL fibers as the inferior boundary of the festooning deformities. The ZCL forms a fold inferiorly called the nasojugal fold tracking laterally and supporting above it the malar mound (see Fig. 10.5 ) before inserting into the periosteum of the lateral zygoma. Some studies suggest the ZCL lateral fibers extend to where the zygomatic arch joins the body of the zygoma at about 3.8 to 4.5 cm in front of the tragus, although other articles report this ligament extends laterally along the zygomatic arch to the tragus. The ZCL fibers are thick and discrete, and can be identified both in the subcutaneous fat as well as in the Sub-SMAS plane. This information is critical as Sub-SMAS ZCL division and release are important when attempting to redrape and reposition the malar fat pad (corresponding anatomically to the drooping medial, middle and SOOF fat pad compartments) during a deep facelift procedure. If one only wants to redrape the skin, it’s enough to release the ZCL in the subcutaneous plane and reduce the possibility of the fibers readhesion by grafting small amounts of fat in the subcutis as well as in the periosteal layers.
Tear Trough Retaining Ligament (TTL) —Corresponds visually to the etched medial depression called the tear trough deformity . This ligament is formed from the fusing of the upper and lower ORL lamella as they merge medially at the midpupillary point into a single thick fiber that extends all the way to its insertion at the medial canthal corner. It can be seen immediately below the dermis tethering the dermis along with the underlying orbicularis muscle to the orbital bone.
Arcus Marginalis —The area on the periosteum of the infraorbital rim that is the origin of attachment for the orbital septum (see Fig. 10.8 ).
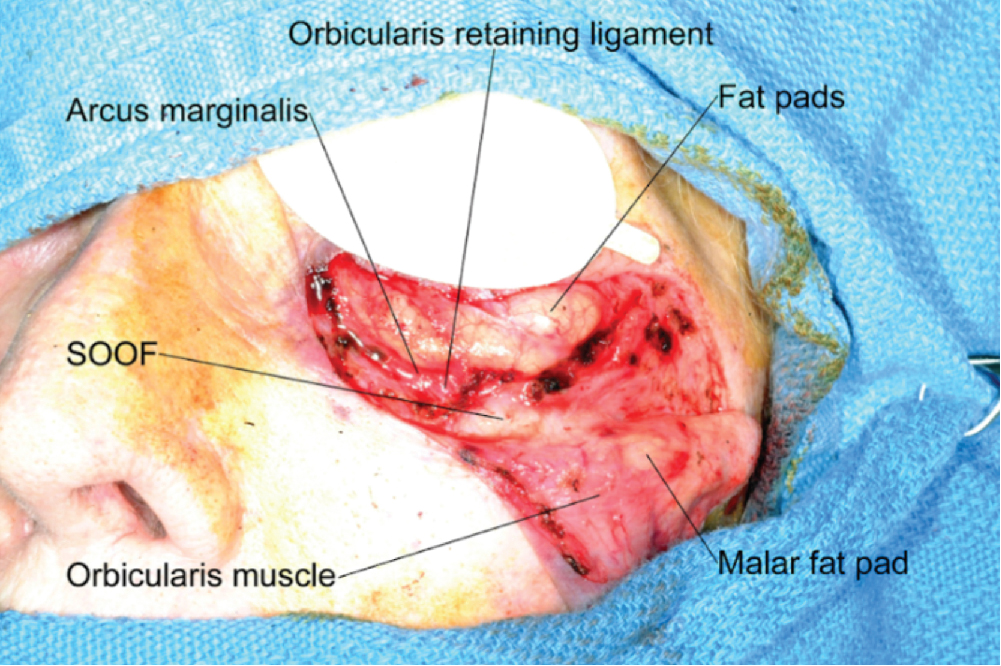
Fig. 10.8
Mohs surgical defect demonstrating pertinent tear trough anatomy. The skin and orbicularis muscle are reflected inferiorly. The malar fat pad is located superficial to the orbicularis muscle but is visible due to muscular attenuation.
(Courtesy Dr. William Ramsdell.)
Tear Trough Deformity —(a.k.a. Lid-cheek crease/junction, infraorbital hollowness, eyelid-cheek crease, palpebromalar groove [sometimes used to refer only to the lateral component of the tear trough], nasojugal groove [sometimes used to refer only to the medial component of the tear trough deformity] we do not like the term nasojugal groove as it confuses the reader with its use of the word nasojugal that is also used when referring to the nasojugal fold located on the cheek—see glossary below and Fig. 10.5 .)—Formed by the taut ORL tethering of the dermis and muscle to the orbital rim and the medial canthal tendon at an angle that keeps drooping inferiorly, widening in diameter, and thus becoming more defined as the skin stretches, the orbital socket widens, the subcutaneous fat thins and atrophies, and the supporting maxillary bone resorbs. The maxillary bone resorption causes a loss in outward projection (described by some as a move from a positive to a negative vector — Fig. 10.2 A and B) and pulls with it the ORL and the dermis inferiorly and posteriorly. The tear trough deformity extends on an inferior and lateral path crossing into the cheek where it forms a crease called the nasojugal fold . At this junction, corresponding to the midpupillary line, this fold measures at about 8 to 12 mm from the lid margin in youth and 15 to 18 mm with advanced age. This fold turns, arching upward and laterally on its path to the lateral canthal tendon. This latter fold, extending from the midpupillary line laterally, should be differentiated from the tear trough deformity and is labeled by many as the palpebromalar groove which defines below it the malar mound . The tear trough deformity and its lateral extension, the palpebromalar groove, represent not only the course of the ORL but also the junction where the orbicularis oculi muscle switches its travel from superficial position over the lower eyelid below the epidermis and above the fat and dives deeper into the cheek area where it lies below the subcutaneous cheek fat and over the SOOF ( Fig. 10.7 showing it in cross section).
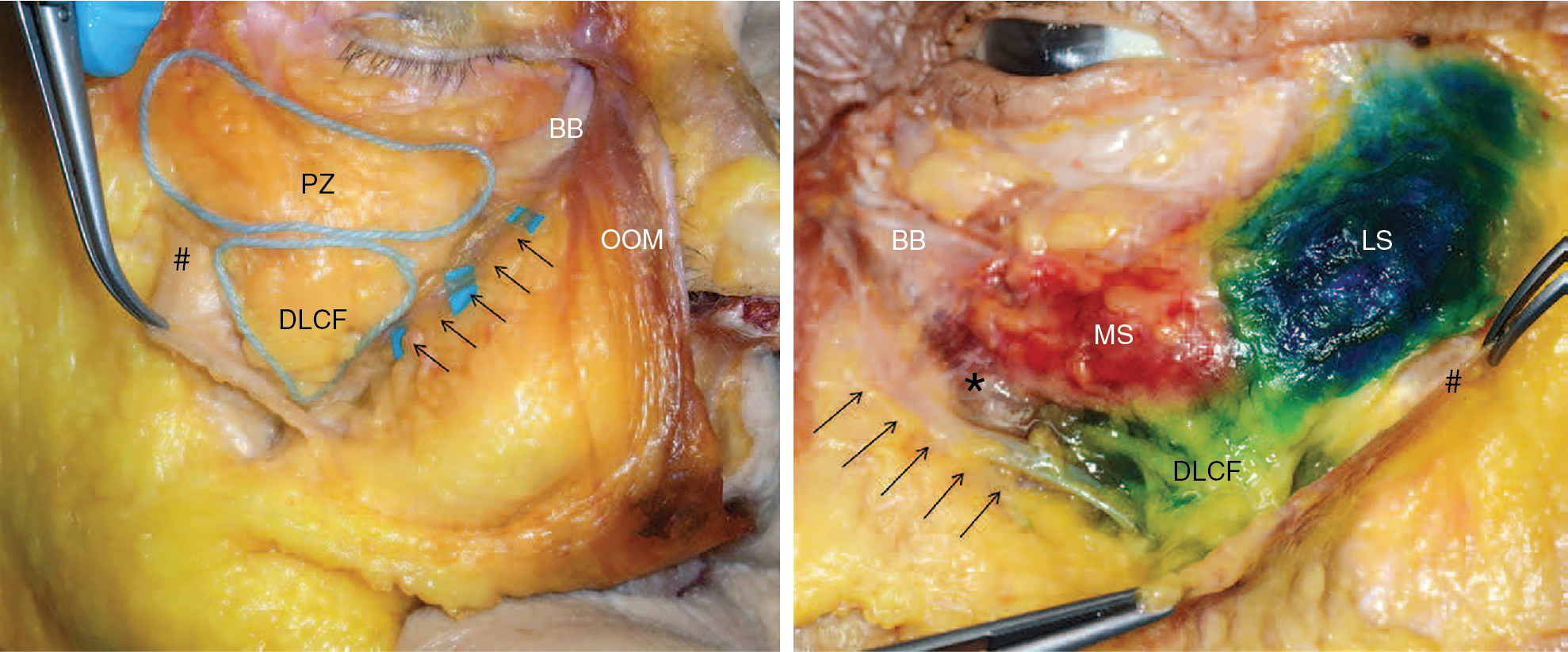
Fig. 10.7
View onto the right and left infraorbital region of layer 4 (deep to the orbicularis oculi muscle (OOM) in a female ( left ) and male ( right ) fresh-frozen specimen. Left , The prezygomatic space ( PZ ) and the lateral part of the DMCF ( DLCF ) are circled. The hash symbol ( left ) indicates the zygomaticus major muscle with its broadly based fibrous origin. This long attachment represents the lateral-inferior boundary of the DLCF. The facial vein is marked by the arrows and represents the medial-inferior boundary of the DLCF. The OOM is flipped toward the nose to expose the bare bone ( BB ) where this muscle attaches on the orbital rim. Right , Dyer has been injected into the prezygomatic space ( red and blue ) and into the lateral part of the DMCF (DLCF, green ). Note that the injection was performed with constant contact to the bone during application in all 3 locations. The red and blue areas correspond to the medial SOOF ( MS ) and to the lateral SOOF ( LS ). The hash symbol ( right ) indicates zygomaticus major muscle with its broadly based fibrous origin; BB , bare bone area after sharp removal of the OOM from its attachment on the orbital rim. The asterisk marks the levator labii superioris alaeque nasi muscle. The arrows point to the facial vein.
(From Cotofana et al. Midface: Clinical Anatomy and Regional Approaches with Injectable Fillers, Plast Reconstr Surg. 2015 Nov;136(5 Suppl):219S-234S.)
Palpebromalar Groove —the lateral extension of the tear trough deformity beginning from the midpupillary line and ending at the lateral canthal tendon, corresponding to the lateral dermal insertion of the ORL . Below and lateral to it lies the malar mound (see Fig. 10.5 ). As we age, it becomes wider and deeper.
Nasojugal Fold/Crease/Groove —(a.k.a. the mid-cheek groove ) a crease that is formed from the central resorption of the medial malar cheek bone tethering on the retaining ligaments and is accentuated by the involution and inferior migration of the medial superficial and deep fat pad compartments inferior to it (see Figs. 10.5 A and 10.9 A and B). This crease corresponds to the junction between the orbicularis oculi muscle and the levator labii superioris alaeque nasi muscle. The crease starts at the nadir of the arch of the ORL right after its bifurcation from the tear trough ligament and is joined at that spot by the ZCL. This point is at about the midpupillary line immediately above the infraorbital foramen. From this point, extending medially and superiorly, this crease turns into the tear trough deformity that continues its ascent towards the medial canthus. Below this point, the crease crosses into the cosmetic subunit of the middle cheek where it defines the medial boundary of the malar mound and curves laterally to form the submalar fold (an extension of the nasojugal fold that follows the osseocutaneous insertion of the ZCL ). The term mid-cheek groove is occasionally used, in some books, when the nasojugal fold appears very deep due to the presence of festoons above it that merge into the malar mound and overhang over a resorbed medial malar bone, making the fold seem deeper and more pronounced (see Fig. 10.5 ).
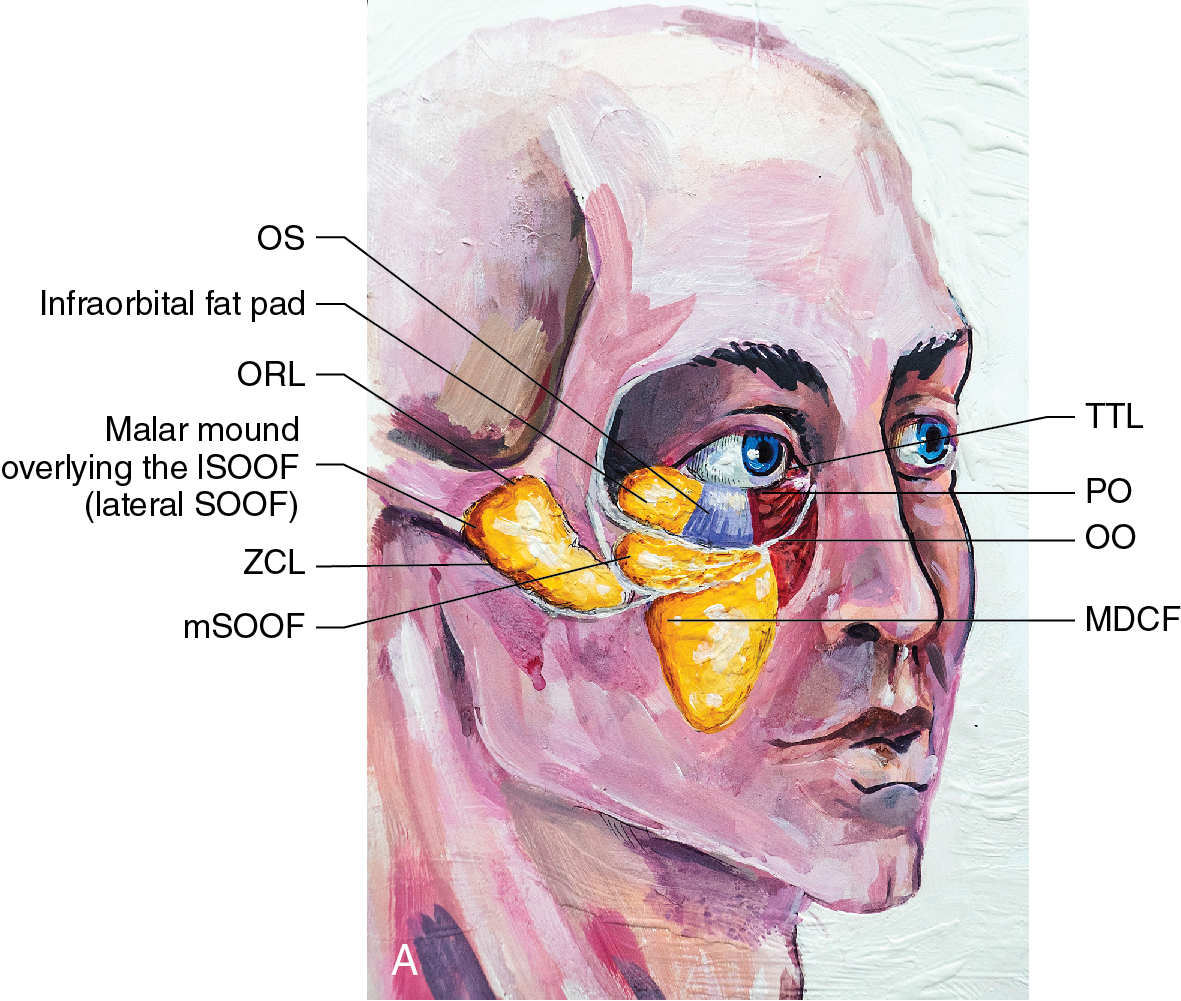
Fig. 10.9
(A and B) Illustrate the position of the facial fat compartments relevant to the eyelid and midface and their relationship to the supporting bone, retaining ligaments, and overlying orbicularis muscle and skin in (A) young face and (B) aged face. Note the changes with age illustrated by the downward migration of the trapped medial SOOF (mSOOF) (6) as well as the inferior and posterior migration of the deflated superficial medial and middle fat pads as well as the deep middle cheek fat pad (DMCF) (7). This, in turn, leads to a more widened and etched separation of the eyelid and cheek compartments tethered by the retaining ligaments due to bone changes as seen with the widening orbital septum and central maxillary bone resorption. Note the relative unchanging position of the malar mound located over the lateral SOOF (lSOOF) (1) and supported by the ZCL. SOOF , Suborbicularis oculi fat. TTL (tear trough ligament), ORL (orbital retaining ligament), ZCL (zygomaticocutaneous ligament), IOF (infraorbital fat pad) (2), OS (Orbital septum) (3), PO (palpebral orbicularis oculi muscle) (4), OO (orbital orbicularis oculi muscle) (5).
(Art courtesy of Dr. Oleg Borshch.)

Malar Mound —(a.k.a. malar eminence ). The malar mound/eminence is different from the festoons with which it is often confused in many articles and books. This confusion can be found even in recent article illustrations. The malar mound is an elongated tear-shaped prominence of soft tissue seen as the lateral projection of the medial part of the zygomatic arch with its superomedial boundary defined by the ORL, its inferior boundary defined by the ZCL , its medial boundary the nasojugal fold, and its lateral boundary defined by an imaginary vertical line drawn inferiorly from the medial border of the zygomatic arch. When festoons form, they often blunt the palpebromalar groove, thus appearing as a medial extension of the malar mound despite being distinct etiologically from it (see Fig. 10.5 ).
Festoons— (a.k.a. malar bags, saddle bags, secondary bags (to differentiate from eyelid bags), triangular cheek festoons)—composed of lax skin, edematous subcutaneous fat, and attenuated orbicularis oculi muscle that cascades in a hammock shape, stretching between the medial and lateral canthi and overhanging as a “poorly supported roof” over the mid-cheek groove at a point of about 3 cm below the lateral canthus . The festoons are a result of multiple factors, the primary one being repeated tissue swelling that leads to chronic edema that is trapped between the superiorly stretched ORL border above it and the inferior water impregnable ZCL that is retracted posteriorly below it. This bone, fat, muscle, and skin repositioning, that is further aggravated by the trapped edematous tissue, leads to the sliding cascade appearance of the festoons . These festoons can be occasionally seen as a temporary complication of infraorbital neurotoxin injection (by reducing the pumping action of the lower orbicularis muscles and zygomatic cheek muscles) or post lower lid blepharoplasty. Author EL has also seen festoons as a consequence of lower eyelid fillers appearing a few years after the injections and completely resolving as soon as the filler was dissolved in the lower eyelids. Festoons can also appear after facelift surgery (when no midface lifting is performed, no deep planes undermining with release of the retaining ligaments and/or when the facelift flap is moved postero-laterally rather than along the natural vectors of the corresponding retaining ligaments without releasing the ZCL or ORL producing a vertical scar barrier to the lymphatic drainage of the lower eyelid and thus chronic recurrent swelling of the area). Other causes of festooning are smoking, high salt diets, crying, lack of sleep, recurrent allergies, blocked tear ducts, eye or sinus infections, mononucleosis, or as a complication of medications, cardiac, renal, thyroid, or hepatic disease.
Submalar Fold —Defined by the fold formed by the extension of the nasojugal fold laterally and accentuated by the hollow below the malar mound inferiorly. This fold corresponds to the lateral osseocutaneous insertions of the ZCL that becomes more pronounced during the malar bony resorption seen with advancing age and demonstrated in Fig. 10.1 .
Mid-Cheek Groove —(a.k.a. nasojugal fold) defined as the inferior boundary of the festoons that begins at about 7 o’clock from the midpupillary line (see Fig. 10.3 ) corresponding to the inferolateral end of the TTL at the insertion point of the ZCL and tracks laterally along the medial path of the ZCL and continues inferolaterally along the nasojugal fold below the malar mound.
Suborbicularis Oculi Fat (SOOF) —is part of the deep fat compartment of the upper cheek and is divided into medial and lateral components ( Figs. 10.5 , 10.8 , and 10.9 ). It is located under the orbital portion of the orbicularis oculi muscle that separates it from the subcutaneous, supra orbicularis, fat compartment. Below the SOOF runs the deep temporalis fascia that separates the SOOF from the muscles of facial expression (the zygomaticus major and minor, the levator labii superioris, and the levator anguli oris muscle), such that the facial mimic muscles are covered by this deep fascia (see Fig. 10.7 ).
Rejuvenation approach
The lower eyelid and midface are continuous entities and should be handled as one unit when preparing for periocular and midfacial rejuvenation surgery. Particularly important is the lid-cheek junction of the lower eyelid. Addressing one and not addressing the other will often create suboptimal results and potential patient’s dissatisfaction. With aging, the face tends to “sag and deflate.” Changes associated with aging occur at all anatomical levels starting from skin down to the bone. Aging skin has more wrinkles and appears saggy secondary to loss of its strength, elasticity, and thinning of the epidermal layer. Additional processes that contribute to lower eyelid deformity are volume loss in the upper cheek, orbital fat herniation from weakening of the orbital septum, soft tissue descent secondary to loss of tissue elasticity, and bone resorption particularly in the maxillary area with resultant tethering of the skin, through the pulling effect of the ZCL, leading to the deepening of the nasojugal groove.
When addressing the folds and SOOF mentioned above in detail, it is key to understand the facial fat compartments and the septa that separate them. Although genetic variations may make the boundary of these structures visible at a young age, aging is the most significant contributor to the noticeable facial changes resulting from these compartmentalized fat divisions. With advancing age, the fat compartments along with their supporting structures of bone deflate and shift inferiorly and posteriorly, causing the boundaries between these compartments to be more pronounced, in turn leading to a more noticeable festooning , periorbital hollowing, nasojugal, and nasolabial folds (see Fig. 10.4 ). To correct this midfacial aging, one can approach these areas both via nonsurgical and surgical techniques.
Nonsurgical approach
If a nonsurgical technique is chosen, one can address this sagging process through thread lifting (lift and support of the folds and fat compartments, such as the SOOF ( suborbicularis oculi fat ) (see Chapter 9 , Figs. 9.2 , 9.3 – 9.4 ) and/or fillers (such as injectable hyaluronic acid [HA], poly-L-lactic acid [Sculptra], fat, stem cells or exosomes— Figs. 10.10–10.12 ).