Containment Surgery For Early Legg-Calve-Perthes Disease
Benjamin J. Shore
I. Hip Arthrogram Including Botox/Phenol to the Adductor/Obturator Nerve and Petrie Casting
Operative Indications
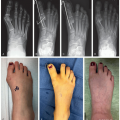
Early stage of Legg-Calve-Perthes (LCP) disease, classified by the Modified Waldenstrom Classification (sclerosis, flattening, and/or early fragmentation), confirmed by sequential plain radiographs and/or contrast enhanced magnetic resonance imaging
Radiographic evidence of early stage with concern for subluxation of the femoral head
Clinical suggestion of decreasing hip range of motion, abduction, and internal rotation
Pain and limp seen on clinical examination
Inability to limit physical activity for a child who is in the early stage of LCP
Age range can be as young as 2 to 4 years but typically between 4 and 8 years of age
Males more commonly affected than females
Often an underlying history of overactivity/attention-deficit hyperactivity disorder
Goal of surgery is to gather dynamic information regarding the shape of the femoral head and if the femoral head “fits” into the acetabulum and to “contain” or protect the femoral head in the acetabulum
Arthrogram rarely done in isolation, commonly performed in addition to soft-tissue or bony containment
Phenol/botulinum toxin is preferred as a first line as there is less morbidity than associated with open soft-tissue lengthening
Equipment
Radiolucent table
Fluoroscopy
18- or 20-gauge spinal needle (3.5 inches)
Nerve stimulator (only for phenol/botulinum)
Contrast agent (Optiray)
5% phenol
Onabotulinum (typically 5 U/kg) no more than 50 units per side for a total of 100 units
If casting, will need fiberglass or plaster supplies and wooden dowel (1 or 2) and two 100 cc syringes
Positioning
Supine on radiolucent table
Can place a small folded towel under buttock if necessary
Pad all other bony prominences
Prep out limbs so that you can take the leg through an arc of motion to dynamically inspect the hip
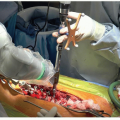
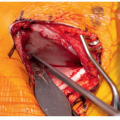
Surgical Approach—Arthrogram
Prep and drape limbs out so that groin is sterile and you are able to move the legs
A subadductor approach is preferred for arthrography
Spinal needle is initially localized with fluoroscopy, with needle resting on skin under the adductor to confirm direction toward the hip joint
Typically, the direction is toward the patient’s ipsilateral nipple and an angle of 45° from the horizontal of the bed or floor
Needle is advanced until images confirm that joint has been penetrated; if uncertain, a small amount of sterile saline can be injected first into the hip. If intra-articular, the fluid will slowly extravasate out of the needle
A mix of Optiray and sterile saline (1:1) is used to perform our arthrogram
It is important to put enough Optiray into the joint to perform an adequate arthrogram, which is typically 6 to 10 cc
Once the dye is in place, perform examination under anesthesia—pay close attention to range of motion of the hip in flexion, abduction, adduction, internal and external rotation in both flexion and extension
Great care is spent looking at the location and relationship between the femoral head and the labrum—the goal is to visualize that with abduction the femoral head can be seen sliding under the lateral labrum and not “hinging” on the lateral labrum and staying outside of the hip joint
Simulated position of the femoral head in abduction and internal rotation is done to help visualize what position in Petrie cast or after proximal femur osteotomy would look like
Technique in Steps
Botulinum Toxin/Phenol Injection
Patient setup is the same as above
We prefer to do injections prior to arthrogram, but they can be done either before or after arthrography
If using botulinum toxin, it is injected prior to the phenol into the adductor longus and brevis neuromuscular junctions
Using a nerve stimulator, the anterior obturator nerve is identified about 1 cm from the adductor tubercle in the adductor compartment
The goal is to identify the anterior obturator nerve with as small an electric current as possible (typically under 1 mA)
Anterior branch of the obturator nerve lies between the fascia of adductor brevis and pectineus muscles
Typically inject phenol to the branch of the anterior obturator nerve, less than 2 cc and titrated to effect; look for loss of conduction with simultaneous stimulation
Petrie A-Frame Casting
Two long leg casts applied in about 20° of knee flexion
We prefer to leave the feet out of the casts, but great care is taken to make a bumper at above the ankle to prevent the casts from sliding down and creating a heel ulcer
A supracondylar femur mold can also prevent the casts from migrating lower
Desired degree of abduction is confirmed by arthrogram to visualize containment of the hip and 1 or 2 wooden dowels are cut to the corresponding length (Figure 22.1)

Figure 22-1 ▪ Petrie casting with bar. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
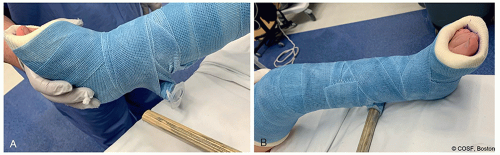
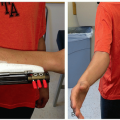
Figure 22-2 ▪ Example of removable bar with syringe. A, Note the empty 10 cc syringe which is used to make the wooden dowel of the A-frame Petrie cast removable. B, Note the dowel is in place and the A-frame is stable. By removing the dowel from the syringe we are allowed for some hip motion and to facilitate easier travel. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
We then take an empty syringe and affix it to the underside of each long leg cast (mid-calf level) (Figure 22.2)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree