Introduction
In 2018, more than 366,000 invasive cosmetic procedures were conducted in the United States. Among these, rhytidectomy, blepharoplasty, and forehead and brow lift constituted over 20% of all cosmetic procedures. While these procedures can be very satisfying for patients and are generally considered safe, they are not risk-free. Complications are best managed through proper patient selection, pre- and postoperative patient education, and meticulous surgical technique. While nearly all surgical procedures carry risk of infection, hematoma, and unsightly scar, each of the procedures listed above have additional complications that are procedure specific. The avoidance, management, and correction of these common and unique surgical complications will be discussed below. Appropriate techniques for the forehead and brow lift can be found in Chapter 3 , blepharoplasty is covered in detail in Chapters 4 , 5 , 6 and 10 , while techniques for face and neck rhytidectomy are discussed in Chapters 7 and 8 .
Preoperative assessment and preparation
Along with careful patient selection, a thorough medical history should be obtained with special attention paid to any bleeding diathesis, use of anticoagulant or antiplatelet medications and supplements. Identifying medical comorbidities that may predispose the patient to poor surgical outcomes, such as smoking, diabetes, hypertension, and autoimmune disease is essential, and the management of these conditions should be optimized. Considering the elective nature of aesthetic procedures, it is often wise to collaborate with the patient’s medical team and assess medications that could potentially increase the risk of excessive bleeding. Since most agents have to be discontinued for 7-10 days prior to the surgery, it is paramount to ensure that this will not predispose the individual to a thromboembolic event. If the risk is too high, a consultation with hematologist may be appropriate in order to consider a bridge-therapy with heparin. Patients should be extensively counseled about the benefit of smoking cessation at least 2 weeks before and after the planned procedure. A complete physical examination of the surgical site should be performed, including an ophthalmologic exam prior to blepharoplasty to exclude any undiagnosed visual abnormalities. The preoperative assessment is covered in additional detail in Chapter 2 .
Management of expectations and a review of common and rare complications with careful documentation of informed consent are essential for all surgical procedures and paramount for elective cosmetic procedures. Setting realistic expectations and reviewing possible adverse outcomes prior to the procedure will help to alleviate anxiety for both the patient and provider. If complications do arise, then both parties are better prepared to deal with them appropriately.
The ability to perform rhytidectomy, blepharoplasty, forehead and brow lift without general anesthesia increases the safety of these procedures and decreases the postoperative recovery time, as well as decreasing the cost to the patient. The authors recommend, whenever possible, local anesthesia for blepharoplasty and brow lift and to consider tumescent anesthesia for rhytidectomy. Tumescent anesthesia for rhytidectomy aids hemostasis and dissection by separating tissue planes and making the inadvertent injury of vital nerves and vascular structures less likely, but the need for large volumes of tumescent fluid places excess tension on the facelift flap (SMAS and skin) and in the editors EL’s experience makes it harder to achieve a similar amount of lift and skin excision as with IV sedation. Low-dose anxiolytics can be used to increase comfort during the procedure for select patients; however, they must be counseled about the risks of these medications and not be allowed to leave the office alone following the procedure.
Common complications
Hematoma: Bleeding and hematoma formation are the most common complications encountered following blepharoplasty and rhytidectomy. Patients should be counseled about the likelihood of mild bleeding and the early signs of a hematoma, which include pain, swelling, redness, and abnormal bruising. Minimal surface bleeding should be controlled with a pressure dressing. Careful preoperative assessment and control of intraoperative bleeding are the simplest ways to avoid hematoma formation. Ensuring patient comfort and thereby reducing intraoperative blood pressure, the use of tumescent anesthesia, when feasible, and blunt dissection with good visualization, will further decrease the risk of hematoma formation. Multiple publications in the plastic surgery literature advocate for the application of fibrin glue to the flap and wound bed prior to closure, and/or the use of tranexamic acid, to help mitigate the risk of hematoma formation.
A hematoma ( Table 12.1 ) will generally occur within the first 24 hours and remain fluid for 48 hours. This necessitates prompt management as a hematoma increases the risk for tissue necrosis, wound dehiscence, unsightly scarring and skin dyspigmentation, infection, and the need for further surgical intervention. The first and most reliable indication of hematoma formation is significant, worsening pain. While purpura and edema are generally also present, their presence is often obscured by the bandage in the immediate postoperative period.











Management of a hematoma requires removal of the bandage and thorough hemostasis. This often requires taking down the flap and carefully examining the surgical site. If a hematoma is simply drained via needle aspiration (18 G) it is likely to reform. Removal of the hematoma directly with lavage, aspiration, or suction should be performed through the existing skin incision, if possible, to reduce the risk of further scarring. If a drain is deemed necessary, it should be removed as soon as possible to decrease the risk of infection. Maintaining a pressure bandage on the surgical site following the management of a hematoma is essential, even if it requires the patient to return to the office daily for dressing changes.
Hematoma formation, excess tension on skin closures, and intraoperative damage to the dermis and epidermis can result in tissue ischemia and necrosis (see Table 12.1 ). Generally, by the time this is apparent, damage to the underlying tissue has already occurred. If a hematoma or seroma is responsible, then the management of that cause can be undertaken. Other causes are difficult to correct and will generally result in some tissue death. The resultant eschar should be carefully monitored and initially left intact to protect healing tissue beneath. Eventually, the eschar may need to be debrided to aid in wound healing and reduce the risk of infection.
Infection: Infection is a rare complication of blepharoplasty and rhytidectomy; however, it has the potential to cause significant morbidity and even death. Sterile surgical technique and a short course of postoperative oral antibiotics are the most effective preventative measures to reduce the risk of infection. Any infection of the skin or soft tissue of the face should be treated rapidly and aggressively. Generally, this requires a prompt examination of the patient, and drainage of any abscess with wound culture to allow for narrowing of antibiotic coverage based on sensitivities. Typically a broad spectrum coverage is started while the cultures are pending. A thorough history can help identify the culprit, just like in one case where the editor EL traced a facelift infection back to the use of ice in the hotel where his colleague’s patient was recovering. The ice was applied to her incision sites to reduce swelling and bruising. The infection responded well to the use of macrolide antibiotics, effectively treating her Legionella infection. This regimen varies but often consist of gram positive coverage with Doxycycline 100 mg PO BID, gram negative coverage with Amoxicillin/Clavulanate 825/125 mg PO BID, and anaerobic coverage with Clindamycin 300mg PO TID. Cellulitis and necrotizing fasciitis require hospital admission, IV antibiotics, and careful monitoring to optimize outcomes.
Scar: Unwanted scar formation (see Table 12.1 ) can dramatically reduce patient and physician satisfaction from an otherwise successful cosmetic surgery. Ensuring that there is little to no tension on the closure and closing each layer of tissue appropriately will reduce the risk of hypertrophic or spread scars. Scars, depending on their type, can be managed with a variety of techniques including surgical revision, (see  ) dermabrasion, ablative and nonablative laser resurfacing, (see
) dermabrasion, ablative and nonablative laser resurfacing, (see  ) vascular laser, massage, topical silicone products, and intralesional injections (steroid, 5-fluorouracil, filler, fat) (see
) vascular laser, massage, topical silicone products, and intralesional injections (steroid, 5-fluorouracil, filler, fat) (see  ). In the past we were instructed to wait 6 months before treating scars.
). In the past we were instructed to wait 6 months before treating scars.
The new scar treatment dogma is to treat scars much earlier, at around 6-8 weeks.
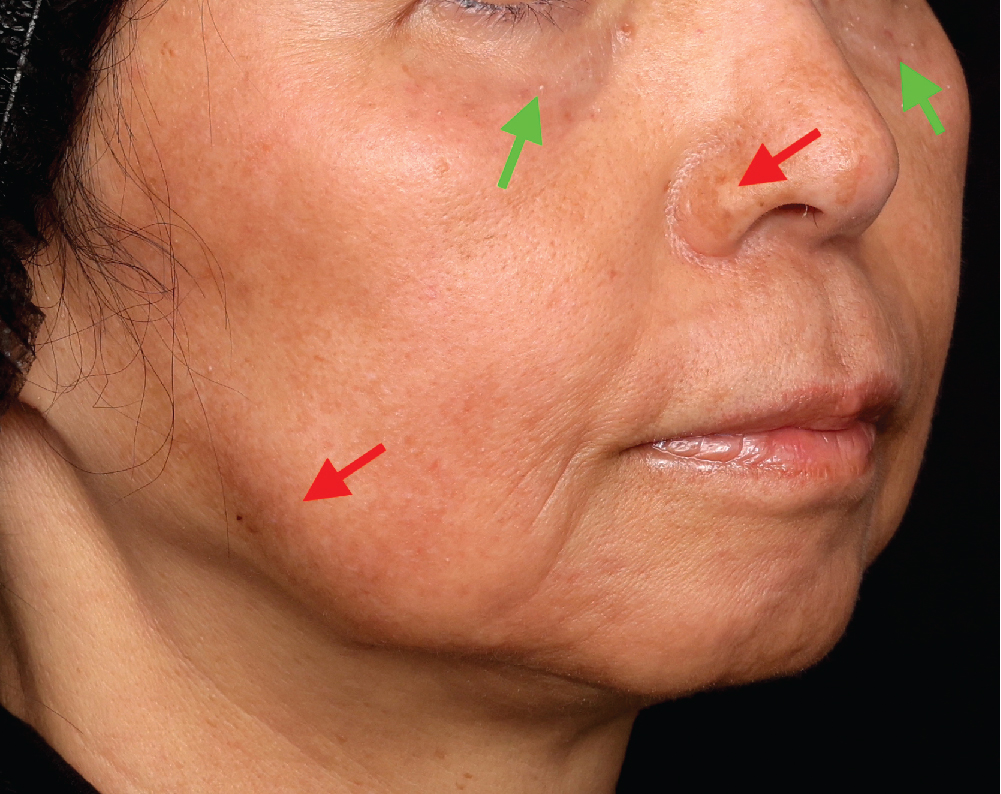
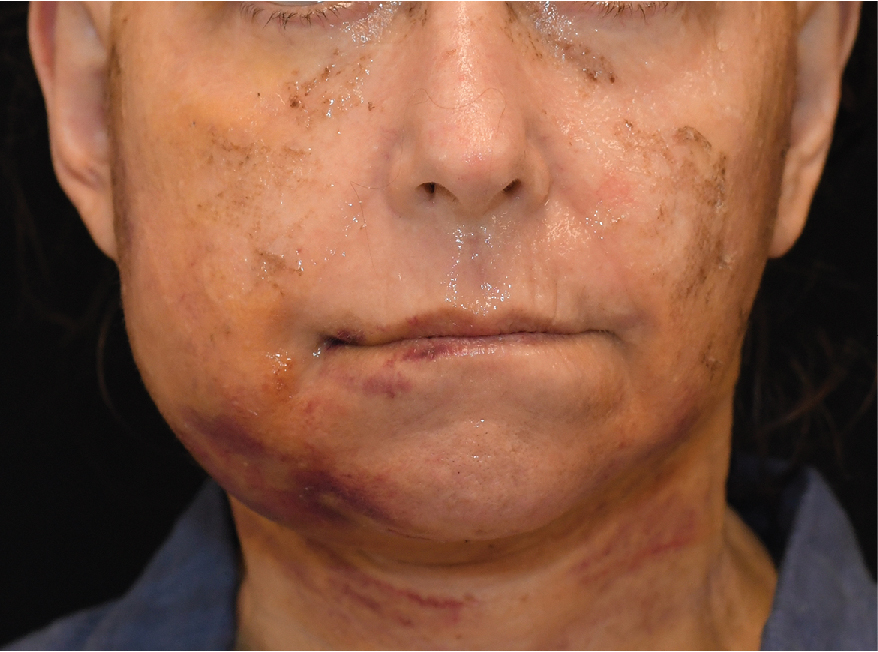
This new dogma was recently validated in a randomized split-scar study by Khorasani et al., examining the safety and efficacy of early scar intervention following skin cancer excisions. Furthermore, most scar experts including Dr. Khorasani believe in a combination approach for scar treatments. For instance, a scar excision or fat transfer may be prudent for larger contour irregularities whereas dermabrasion may be used for minor surface irregularity. Fractional ablative Co 2 resurfacing is often used for dermal remodeling to address scar texture and Pulse Dye Laser (PDL) is used to treat dermal vasculature to improve erythema. The case shown in figure 12.1 nicely illustrates the benefit of this combination treatment approach. Given the vectors of this traumatic chin scar the re-excision was done in separate stages in order to prevent the closure vectors pulling on each other. Stage 1 included re-excision of scar on left chin followed by re-excision of the scar on right chin 6 weeks later (Stage 2). Once the deeper contour irregularity was addressed with re-excision, patient returned for Stage 3 on post operative day 42, which included the treatment of the surface irregularity via dermabrasion and scar texture via ablative fractional Co 2 resurfacing. Finally, Stage 4 of the treatment was concluded by addressing scar erythema with the use of a PDL laser on post-operative day 70 and 84.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


