Chapter 9 Filling Temples With Highly Diluted Hyaluronic Acid Fillers
The eyes say nothing but a cyclone of meaning swirls all around them
V L
Many of the changes of aging can be understood by observing changes of facial weight. Some faces gain weight, albeit unevenly, from bottom to top. Other faces thin, and the cheeks, orbits, and temples all hollow with age. As the temples subside, the effect is not just to conspicuously narrow the upper part of the face, but as the tails of the brow fall into the temple hollow they seem to shorten and descend. Temple wasting, like the prejowl sulcus, can be an early sign of aging; some younger people who otherwise look reasonable for their age can exhibit this phenomenon.
Problems involving the temple are both technical and aesthetic. The normal temple may be flat or slightly concave or convex, and the point where a slightly concave temple becomes an aged-looking hollow temple is a matter of judgment. What a temple emphatically should not be is very convex. This appearance can vary from alien to hydrocephalic and is not desirable in any case.
The loss of temple volume is likely from soft tissue—fat and muscle—because the temporal bone isn′t thick enough to explain the collapse of shape. An older temple can be quite thin with no subcutaneous padding and have visible vasculature.
Certain concepts of facial injections are not at all intuitive. Patients simply don′t understand how filling in the anterior jawline, temples, and brows will look, and photographs do not express the anticipated changes to a particular individual in the examination room.
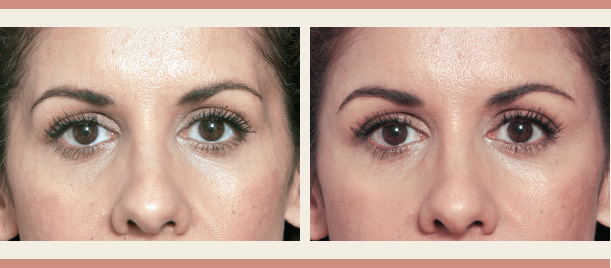
The concept of trying on clothes to see how they look is a traditional and universal way to choose between options; it is no surprise that computer-assisted patient imaging has become a powerful tool to demonstrate possible outcomes of surgery. I rely heavily on a simple form of injection imaging, which is simply to preview the result by injecting dilute local anesthesia to duplicate the effects of the ultimate filler injection in an attempt to show the patient the aesthetic choices. I use one and one half times the projected filler amount to fill the temple hollow and then massage it into place.
Although injecting the brow this way requires some practice, temple and anterior jawline previews are easy. This simple maneuver is immensely helpful for a number of reasons: The patient will have seen the result beforehand, which is the most effective informed consent possible. Patients like to be able to make the decision on whether to do a procedure; here the balance of power shifts to the patient: If they don′t like the preview, the saline simply resorbs. If they like the preview, they know the result and are more likely to be satisfied with their new look. Hence postinjection complaints are very rare. Doing the preview enables the clinician to adjust the final injection to maximize the effect. If I am unsatisfied with how the preview looks, I share that opinion with the patient.
As a byproduct, the area is now numb and vasoconstricted and ready to inject. The deep subcutaneous tissue of the temples is less sensitive than most areas of the face, and local anesthetic can be foregone; however quite large vessels are present in the vicinity and vasoconstriction is a good idea for all injections. The presence of the anesthetic does not make the final injection more difficult; the clinician should know the effect of the dose given. In the temple it ranges from 1 to 2 cc.
This chapter discusses the use of highly diluted hyaluronic acid (HA) products to fill and level the temples. The physical properties of the highly diluted injectate distribute the filler in a way not possible with traditional injection practices. This technique is very effective and yields predictably smooth results. Experienced injectors typically have an extremely low incidence of complications.
PATIENT EVALUATION AND SELECTION
The ideal patient for temple filling is one whose temples look hollow, most easily seen as a shadow behind the superior lateral orbit. Patients who have an imbalance in the size of the face below the arch and above it (“my head looks like a peanut”) should also be considered. Ultimately, because this is a cosmetic procedure, the best determinant of patient happiness is whether the patient looks better with the temples filled.
TECHNIQUE
Procedure
The boundaries of the temple are defined by the patient′s anatomy and don′t necessarily have textbook borders. The temples are marked; one side is almost always deeper than the other. The apex of the temple hollow is at the temporal fusion line and is marked. The hollow is oblong and is commonly deepest immediately lateral to the orbit and above the arch. The injection site is planned just inferior to this area over the arch; using this site automatically places more fill in the hollow without having to make a conscious accommodation. I originally used needles to fill the temple; however, now I only use cannulas because of their minimal pain and bruising and higher safety profile. The length of the cannula (usually a 2-inch No. 22 or 1.5-inch No. 25) should reach from the injection site to the upper border of the defect; otherwise the temple deformity will not be fully corrected.
There are two main commercially available HA filler lines in the United States at present. One is particulate and the other is more highly crosslinked. I have found that the long-term results (2 years and longer) are slightly more smooth with crosslinked fillers, but they are also more difficult to inject when diluted because of their much higher viscosity.
Dilution
One of the keys to this procedure is a high dilution of the product with saline. It is difficult to expand a flat surface smoothly by injection (the same in reverse is true with liposuction). Dilution makes it easier to maintain evenness of the product placement, because each pass of the cannula puts in a relatively small amount of product. Although fillers can be placed without dilution, this technique makes a difficult injection much easier.
The injection site is blocked with a small amount of 0.5% lidocaine with epinephrine, and the preview is conducted. Using 1 cc or less of an HA filler per side is not likely to produce a sufficient visual change in the volume of the temples; I find that 1.5 to 2 cc per side is almost always the right amount for women and that men require 0.5 to 1 cc more, depending on their anatomy and the depth and size of the hollow.
The product is diluted, using a Luer-Lock transfer hub. More dilution results in a safer and smoother result; a 2:1 ratio of saline and local anesthetic to filler is my usual. Therefore the most common dilution is 2 cc HA, 1 cc 1% lidocaine with epinephrine, and 3 cc normal saline to make a total of 6 cc (when 1% plain lidocaine was used in the diluent, the incidence of lower lid bruising was higher). Once the injection point is blocked, the rest of the injection is surprisingly painless.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


