Chapter 4 Perioral Rejuvenation
Watch your mouth.
D H
PATIENT EVALUATION AND SELECTION
The mouth and the perioral area is, like the periocular area, a source of the emotional expression and sensuality of the face. Nevertheless this area′s aging is often overlooked, resulting in a disappointing result of a comprehensive facial rejuvenation. Nearly every facial rejuvenation treatment should involve some modality of perioral rejuvenation.
Aging changes around the mouth are multifactorial, and contrary to common belief they are not limited to deflation alone. Therefore only revolumizing the vermilion may result in disappointing or even unnatural results. Redefining the lip contours should also be a consideration rather than blowing the vermilion up with volume. This, combined with resurfacing or liplift, delivers a more comprehensive restoration of the youthful appearance of the lips and perioral area.
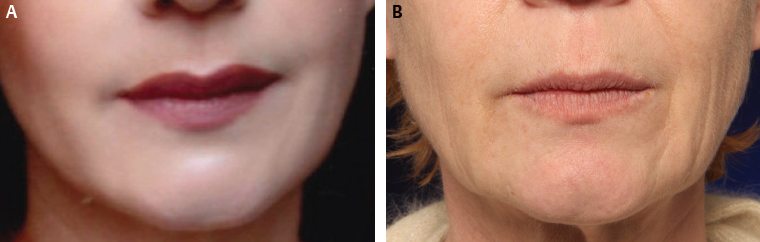
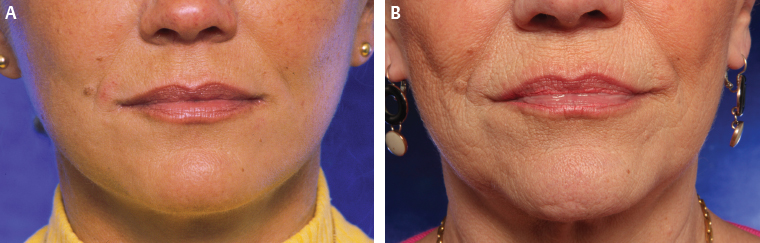
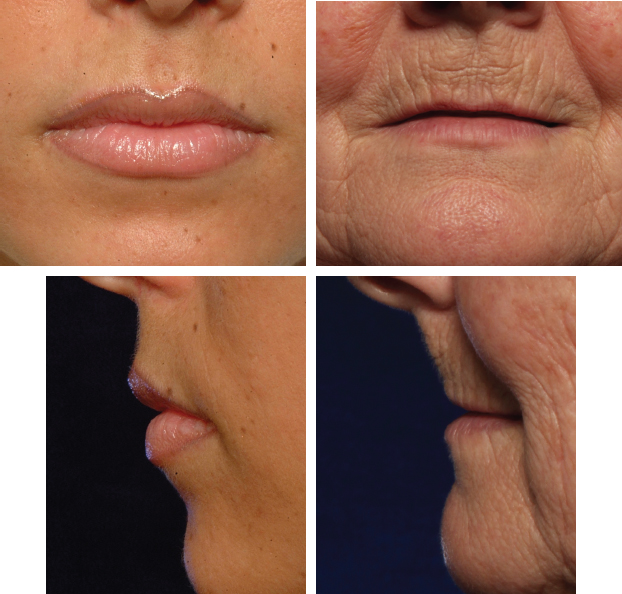
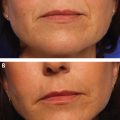
Aging of the perioral region involves the accentuation of the nasolabial crease and fold; changes in skin texture with the appearance of perioral rhytids (barcode); atrophy of the vermilion volume; loss of definition of the vermilion border, white roll, and philtrum; and increase in vertical height of the upper lip between alar base and vermiliocutaneous border (Figs. 4-1 and 4-2). Remarkably, this lengthening of the upper lip is the only region in the central part of the face where “sagging” is obvious, observed in long-term photographic studies of facial aging. The treatment plan is multimodal by combining fat grafting, resurfacing techniques, and surgical liplift. The combination of these techniques is another example of synergy in the rejuvenation of the perioral area.
Anesthesia
In general the perioral area can easily be numbed by a double nerve block of both infraorbital and mental nerves. This usually does not anesthetize the philtrum and the oral commissures, which need additional infiltrative anesthesia. The specific areas to be microfat grafted are additionally infiltrated with a solution of lidocaine and adrenaline to provoke vasoconstriction.
Perioral Rejuvenation Techniques
Correction of the Nasolabial Fold
The nasolabial fold has historically been corrected with a multitude of techniques, which is most often a sign that none of them is perfect. In particular the “lifting” techniques, for which the nasolabial fold was seen as a component of the descent of the midface, were prone to relapse. Some techniques even described very extensive undermining from the facelift incision progressing under the nasolabial fold or even more medially, but they could not guarantee long-lasting results. If the nasolabial fold is considered as an atrophying area, because of repetitive movements over the years, the logical treatment is filling. In theory another option would be to stop the movement in this area with toxins. This can be observed in the case of facial paralysis, in which the affected hemiface nasolabial groove is completely eradicated. However, clinically this is impossible, because all mimic activity of the face would be disturbed. Therefore correction of the nasolabial fold is better achieved by microfat grafting.
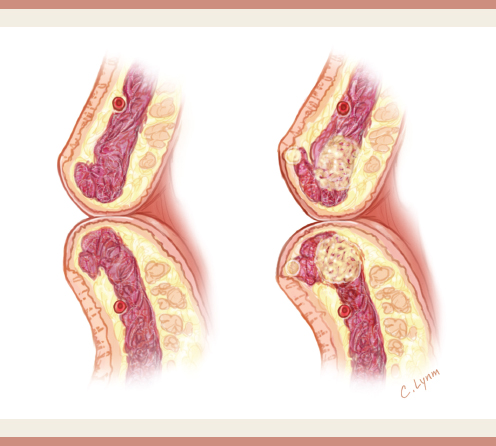
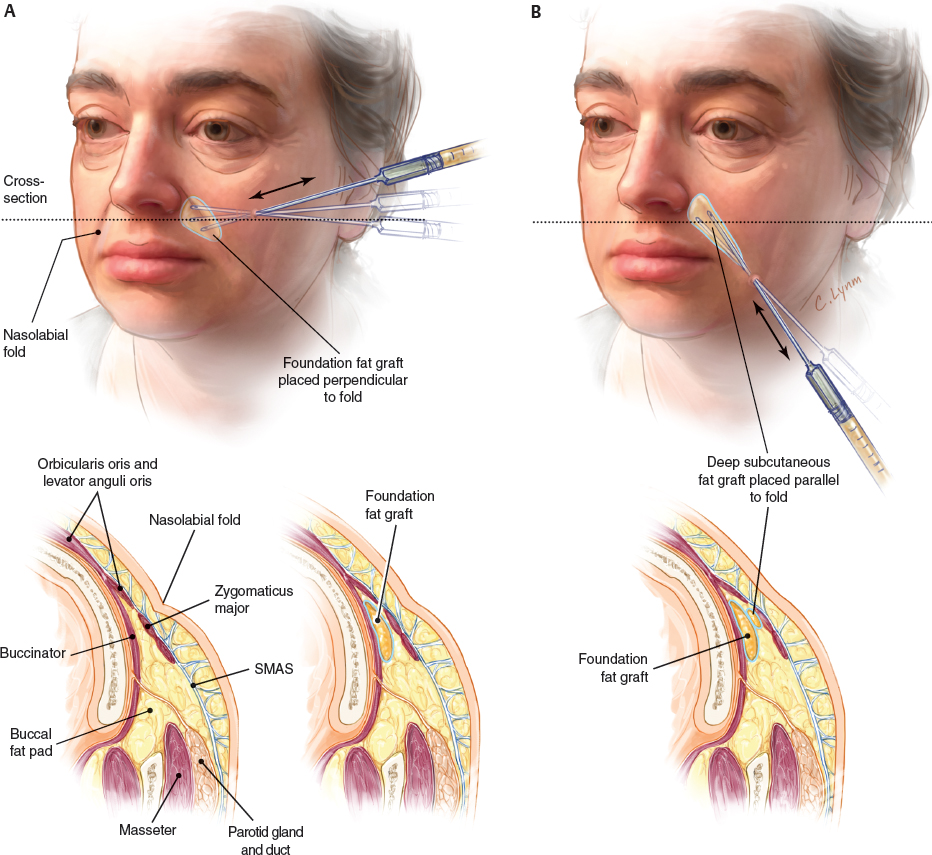
The deep filling of the crease is accomplished with classic 0.7 to 0.9 mm fine blunt cannulas via a puncture hole with an 18-gauge intravenous needle. A crisscrossing approach is used, starting perpendicularly to the crease in the deep plane to build up a foundation. This is important to prevent a sausagelike deformity, as seen in parallel lipofilling techniques. Most volume goes into the canine fossa, with a triangular blending extension toward the corner of the mouth (Video 4-1). Next a second, more superficial layer is deposited parallel into the fold. Finally a subdermal subcision maneuver is executed with an 18-gauge needle, used as an internal knife.
This procedure cuts all the ligament attachments from the skin to the deeper structures (Fig. 4-3). A small volume of microfat (0.3 to 0.5 cc) is then injected into the created cavity, not as much as a filler but rather as a spacer to prevent reattachment of the skin to the deep tissues.
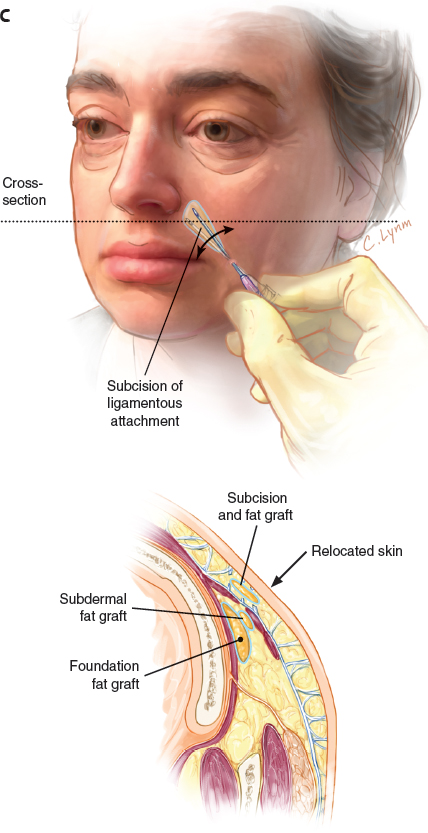
The average injected volumes are 1 to 3 cc of microfat per side. Undercorrection is preferable to overcorrection in this area. Effective, natural, and long-term correction is expected with this technique.
Lip Rejuvenation and Enhancement
Adding volume to the lips and vermilion can be very rejuvenating and feminizing. This explains the popularity of this procedure, either with fillers, implants, or fat grafting, and this is true for all age categories. Lip augmentation is not only restricted to rejuvenation procedures but also is used for younger patients who wish to enhance the shape and volume of their native thin lips.
Volumizing the lips can certainly enhance the sensuality of the mouth. However, when a certain volume limit is exceeded, the global result can become rather unnatural or even ridiculous, because adding volume to the lips will augment the anterior projection of the lip and vermilion. When this is exaggerated, it likely will result in a sausagelike or ducklike deformity of the upper and/or lower lip. Eversion of the vermilion border is better achieved by adding a liplift.
Female Lip Aesthetics
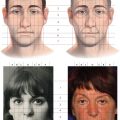
The proportion of upper to lower lip volume must be respected (Fig. 4-4 and Table 4-1). In most people the lower lip is slightly larger than the upper lip in the frontal view. When this proportion is violated by augmenting only the upper lip, an unnatural appearance may occur. Therefore the upper and lower lip are typically augmented simultaneously.
In patients of Western European descent, in the frontal view the upper to lower lip height ratio is approximately 1:1.618, in accordance with the golden proportion. In other words, the lower lip is roughly 50% larger than the upper lip. These proportions are important, and must be preserved when enhancing the lips. Often patients ask for an isolated upper lip augmentation. In most cases this disturbs the natural proportions of the upper to lower lips. The surgeon should explain to these patients that the lower lip needs to be enhanced in proportion to the upper lip. Often a higher volume is needed in the lower lip than in the upper. Failure to respect these observations may result in an unnatural appearance (Fig. 4-5).
Ideal lip aesthetic proportions may cause some confusion:
In the frontal view the lower lip should be approximately 60% higher than the upper lip (the golden proportion of 1:1.618).
In the profile view the upper lip should project slightly (1 to 2 mm) further anterior than the lower lip.
In the young lip, the vermiliocutaneous border, or white roll, is well defined and pouted, with a distinct Cupid′s bow in the frontal view. In profile view the youthful upper lip should project 1 to 2 mm anterior to the lower lip. The contour from the nasal base to the vermilion border should be slightly concave. The philtral columns are prominent and well-defined. The oral commissures should be horizontal or curve slightly upward. The mucosa is soft with a distinct turgor. The skin surface is smooth, equally toned, and without rhytids.
Aging disturbs these parameters to a certain degree: The vermiliocutaneous border loses its definition and flattens out. The definition of the Cupid′s bow fades in the frontal view. The projection of the upper lip decreases and becomes level or even posterior to the lower lip. The contour from the nasal base to the vermilion border becomes straight to convex because of lengthening of the lip and subsequent inversion of the vermilion. The philtral columns lose prominence and definition. The oral commissures tend to turn downward. The vermilion mucosal surface becomes dryer and atrophic and loses turgor. The skin surface becomes rough, pigmentary irregularities occur, and vertical rhytids appear (the barcode appearance).
Harmonic lip enhancement should ideally treat all of these aesthetic features. A combination of several treatment modalities will work synergistically toward a natural enhanced appearance. The tools are volume enhancement, liplift, and resurfacing.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


