Chapter 6 Nanofat Grafting
It′s kind of fun to do the impossible.
W D
Lipofilling has become a very important and valuable tool in plastic surgery. The indications for fat grafting are increasing steadily.
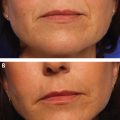
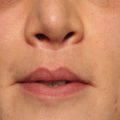
For the past 20 years, aesthetic and reconstructive plastic surgeons have safely and effectively used autologous fat grafting to provide structural augmentation of the subcutaneous layers of different regions of the human body. For the first decade, most reports suggested that the goal was to obtain as pure adipocyte cellular grafts as possible, isolated with minimal trauma, and transplanted into adipose-containing tissues. A high number of case reports and small series reported trophic changes in the overlying skin, and some surgeons described remarkable results after lipotransfer in atrophic and radionecrotic ulcers. Personally we could perceive changes in quality, pigmentation, and texture of the facial skin of many patients, months after they had fat transferred into certain regions of the face. Clinically, however, it was not easy to determine whether these changes in skin quality were a result of better filling under the relaxed skin rather than to intrinsic structural changes of the skin.
Adipose-derived stem cells were first discovered in 2001. In the past 10 years, biocellular regenerative medicine has recognized the potential value and availability of stem cells in adipose tissue. More and more, adipose tissue is no longer seen as a simple layer of insulation material and a storage organ of caloric energy. Fat tissue is now recognized to be a complex endocrine organ that is intrinsically involved in metabolism and immunomodulary activities and that provides an extensive reservoir of multipotent, undifferentiated cell populations that are involved in homeostasis and regeneration. Although adipocytes represent 90% of the volume of fat tissue, they only account for 20% of the number of cells in the fat. The function of the other 80% population of small cells in adipose tissue is still under investigation.
Two important concepts in this context involve stromal vascular fraction (SVF) and cell-assisted lipotransfer (CAL). SVF is defined as all living cells in the lipoaspirate except mature adipocytes. The SVF of adipose tissue is a rich source of preadipocytes, mesenchymal stem cells (MSC), endothelial progenitor cells, T cells, B cells, mast cells, and adipose tissue macrophages. To obtain the SVF, fat isolated by liposuction is classically processed by collagenase treatment and centrifugation. CAL is an autologous stem cell procedure that is basically a fat transfer procedure with a boost of SVF to increase its potency. Whether the results of CAL are any better than classical lipofilling is debatable. The separation of the SVF from the adipose tissue by enzymatic treatment and centrifugation is still time-consuming, expensive, and in many countries clinically not permitted because of regulatory issues of “biological drugs.”
At first, the main goal was to isolate, concentrate, and expand stem cells for future reconstructive and regenerative tissue engineering applications. In recent years, many researchers and clinicians began to understand the complexity, contents, and paracrine functions of the adipose-derived SVF. Some researchers and clinicians believe that it might be more effective to transfer the intact microenvironmental mixture of components within the lipoaspirated sample without any manipulation. The clinical results obtained with nanofat grafting support our hypothesis that the use of the entire mixture of cells and their native scaffold (extracellular matrix, perivascular structural tissues, and intracellular messengers) may be of greater value than any of the components of SVF used separately. The complex signaling and paracrine activities of intercellular cross-talking may be hard to reproduce if these isolated elements are injected separately.
With the nanofat grafting technique, we inject regenerative cells and elements in the clinical setting by processing adipose tissue with a very simple mechanical manipulation. This technique destroys the mature adipocytes and leaves the complex mixture of perivascular smaller-sized cellular components intact and in their native paracrine environment. Nanofat grafting may open possibilities of adipose tissue as a primary source of mesenchymal cells and SVF in biocellular therapies in the future.
Our experience with fat grafting started with Coleman′s standard lipostructure technique to correct volume losses caused by disease, trauma, or aging. Fat was initially injected with relatively large blunt cannulas of approximately 2 mm diameter. Inspired by Coleman and several other authors who promoted fat grafting as an essential part of facial rejuvenation, we started to incorporate lipostructure in our cosmetic facial cases. For delicate areas such as the eyelids and lips smaller cannulas became popular. Lipofilling with cannulas as small as 0.7 mm diameter, also called microfat grafting, was described in Chapter 2 of this book. Also, these small-particle fat grafts proved to be applicable for sharp 23-gauge needle intradermal fat grafting, published as the SNIF technique (Chapter 5). Our ambition was to inject fat through even smaller needles (27 gauge) in even more superficial layers of delicate skin areas to enable us to fill very fine rhytids and to improve the quality of the skin. To allow passage of the fat graft through these 27-gauge needles, we emulsify the microfat mechanically. We refer to these extremely reduced microfat particles as nanofat. Surprising clinical changes in the quality and texture of the treated skin areas led us to investigate the content of this nanofat. This chapter describes the technique and our experience with nanofat grafting. It also explores the basic research on the cellular content of the nanofat.
INDICATIONS AND CONTRAINDICATIONS
Nanofat is not a soft tissue filler; hardly any viable adipocytes are present in the injectable substance. Nanofat is applicable in a wide range of indications to improve the skin quality.
There are three categories of indications for the use of nanofat:
1. Trophic skin changes caused by age and sun damage
2. Pigmentary skin conditions
3. Scarring and atrophic skin conditions
Presently nanofat is an integral component of our facial rejuvenation strategy, and we offer it to all of our patients. Nonfacial areas such as the neck, the décolleté area, and the hands can also greatly benefit from the use of nanofat grafting, sometimes in combination with microfat or SNIF.
Because of the simplicity and safety of the procedure, nanofat grafting has no specific contraindications.
PATIENT EVALUATION AND SELECTION
Trophic skin changes caused by age and sun damage
– Thin dermis (cheek, lower eyelids, lip mucosa)
– Atrophy
– Craquelé surface
– Spotted pigmentary changes
Pigmentary skin conditions
– Dark circles under the eye caused by a combination of translucency of the skin because of thin dermis and a degree of melanin pigment deposits (both components appear to improve after nanofat grafting)
– Mottled pigmentation of the face
Scarring and atrophic skin conditions
– Hypertrophic scars
– Atrophic scars
– Postradiotherapy skin atrophy
– Ischemic necrosis of skin flaps
PREOPERATIVE PLANNING AND PREPARATION
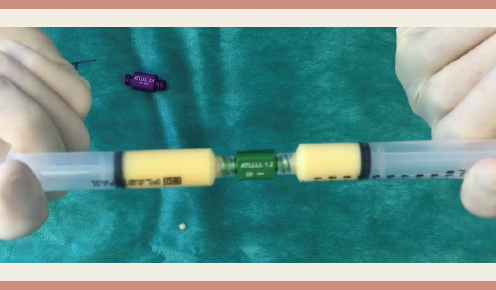
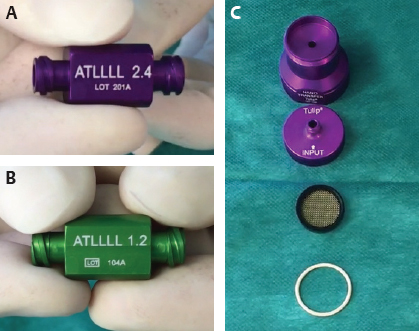
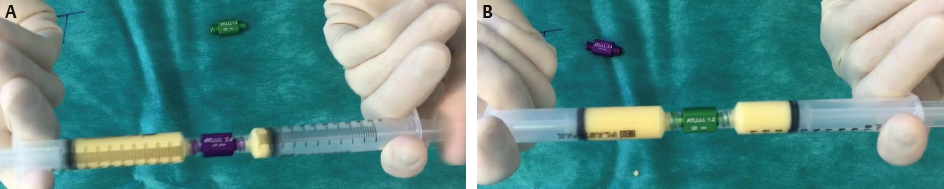
Microfat is harvested with the multiholed microcannulas and processed as described in Chapter 2 of this book. The rinsed and filtered microfat is then transferred into 10 cc Luer-Lok syringes and mechanically emulsified. Emulsification of the fat is achieved by vigorously shifting the microfat between two 10 cc syringes, connected to each other by a purple, 2.4 mm diameter female-to-female Luer-Lok connector (Figs. 6-1 and 6-2). After 30 passes the fat becomes more liquid and whitish (see Fig. 6-2, C). This number of passes is arbitrary but has proven to be effective in our experience. This process is then repeated with the green, 1.2 mm diameter connector, also for 30 passes. This ensures that even the most fibrous fat can be emulsified, and that no viable adipocytes remain in the resulting nanofat. The change in color is a result of the emulsification of the grafted material. The endpoint of the emulsification is a visible change in the consistency and color of the material in the syringes. After the emulsification process the fatty liquid is passed through a strainer cartridge with a dual 400/600 micron filter. This maneuver removes connective tissue remnants that could block the fine 27-gauge needle. The effluent is the end product, nanofat. It is transferred from the 10 cc Luer-Lok syringes into 1 cc syringes for injection.
NANOFAT ANALYSIS
Adipocyte Viability
We analyzed the content of three samples of lipoaspirate obtained from the same patient. Fat was harvested from the lower abdominal region after infiltration with a Klein anesthetic solution. Two different aspiration cannulas were used, and three different lipoaspirate preparations were analyzed:
Sample 1 (Fig. 6-3, A and B): Aspiration with a standard 3 mm “Mercedes” liposuction cannula with three large side holes (2 by 7 mm) to produce macrofat
Sample 2 (Fig. 6-3, C and D): Aspiration with a multiport 3 mm cannula with multiple sharpened 1 mm side holes, processed by saline rinsing and filtering into microfat
Sample 3 (Fig. 6-3, E and F): Microfat processed into nanofat as described previously
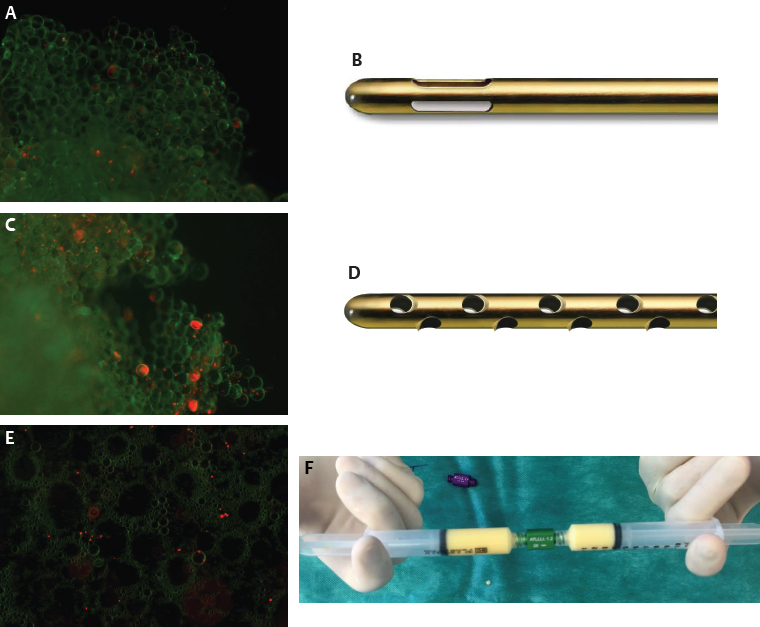
The viability of the adipocytes in these three samples was evaluated using fluorescence microscopy after a live-dead staining. The adipose tissue of the macrofat and the microfat had a normal histologic structure, with preserved viability of most of the adipocytes (green color on Fig. 6-3, A, C, and E). In the nanofat, however, no viable adipocytes were observed, and the adipose tissue structure was histologically completely destroyed and replaced by an oily emulsion.
Cell Culture
Stem Cell Isolation
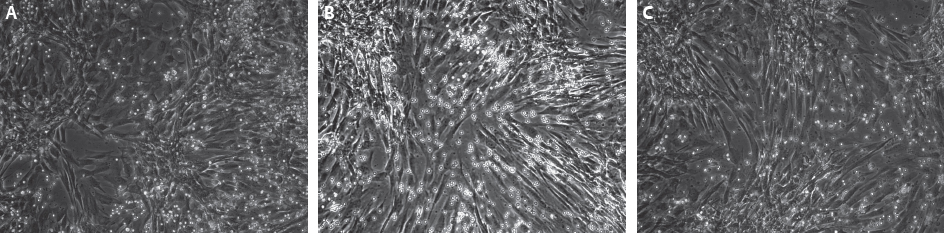
Stem cells in the three samples were isolated with a standard method using collagenase and centrifugation, and a cell count was performed. The SVF and isolated stem cells were analyzed. The stem cells are identified by the presence of the CD34+ surface antigen, detected by bioassay. SVF cells and viable stem cells derived from the SVF were abundantly present in macrofat, microfat, and nanofat, in comparable amounts. Apparently the mechanical emulsification process only killed the adipocytes, which are up to 100 times larger than SVF cells that were preserved. The number of CD34+ cells (stem cells) in the SVF also was comparable in all three samples (Fig. 6-4). These stem cells were then cultured in a standard medium and developed the same fibroblastic morphology in the three samples, which is a typical feature of adipose-derived stem cells.
Stem Cell Differentiation
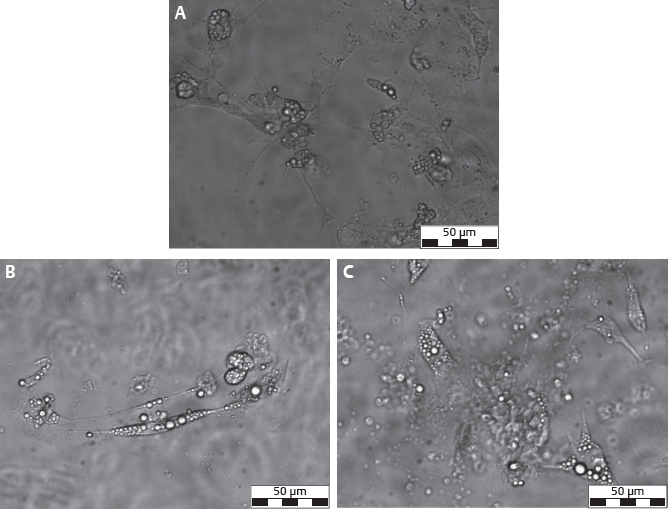
The typical property of stem cells is their ability to differentiate into different cell lines. To demonstrate the stem cell nature of the SVF and CD34+ fractions, these cells were transferred onto an adipogenic differentiation medium (Fig. 6-5). After 10 days of culture, phase-contrast microscopic evaluation showed spherical cells containing lipid vacuoles, indicating differentiation into an adipogenic lineage. No difference in quality or quantity of adipocytes were noticed between the different lipoaspirate samples. Light microscopy after red oil O staining confirmed the presence of large adipocytes independent of the lipoaspirate processing method.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


