Chapter 7 Centrofacial Rejuvenation: Putting It All Together

It is not what you look at that matters, it is what you see.
H D T
The eye sees only what the mind is prepared to comprehend.
W R D
Historically facial rejuvenation surgery initially focused only on correction of laxity and apparent skin excess in the face, completely disregarding the other aspects of the aging process such as volume loss and structural changes in the skin surface. As a consequence, many operations resulted in a tight facial appearance but were defective in restoring a natural youthful appearance. This situation was further exacerbated by secondary and tertiary facelift surgeries.
Parallel with facelift evolution, other modalities for facial rejuvenation were developed, including volume restoration either with nonautologous or autologous materials and surface enhancement by either physical (laser) or chemical processes.
Around the turning of the millennium the awareness that physical aging of the face is a multifactorial process was growing. Aging is now understood to consist of facial sagging and skin laxity, changes in skin texture and pigmentation, changes in volume in certain areas of the face, and contraction of certain facial muscles producing permanent folds and rhytids.
If the surgeon does not actively consider the contribution of all these factors to facial aging, it will be impossible to reproduce or even approximate the lost natural appearance of youth. As David Thoreau wrote, “It is not what you look at what matters, it is what you see.” For decades aesthetic surgeons have overlooked important causes of facial aging such as deflation, simply because they had no awareness of this aging phenomenon. Only after they understood the effects of facial deflation on the aging process did facial aesthetic surgeons actually begin to see it in virtually every aging face. Or, as quoted from William Davies, “The eye sees only what the mind is prepared to comprehend.”
This understanding has caused a true paradigm shift in the way surgeons now analyze and treat the aging face. The deflation process is most important in the centrofacial area, which consists of the periorbital and perioral areas.
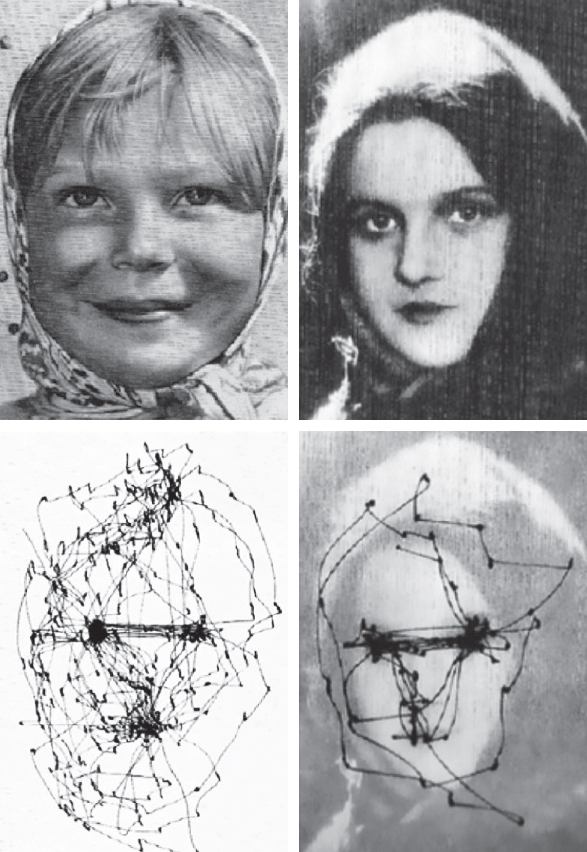
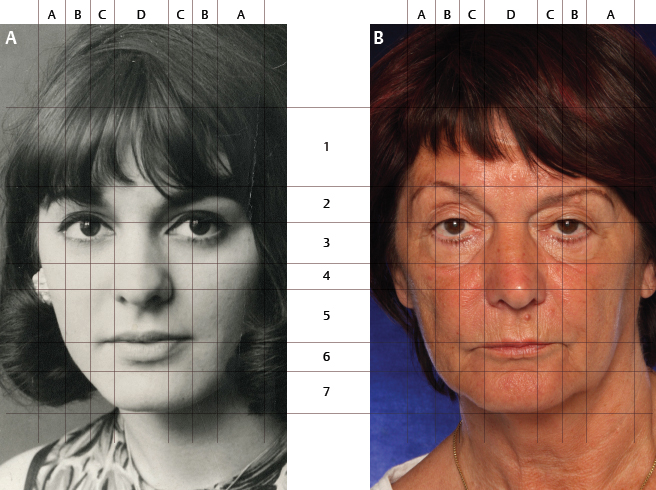
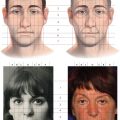
Based on studies of eye-tracking movements it is apparent that, when looking at a human face, the observer scans the eyes and the mouth following an inverted triangular pattern1 (Fig. 7-1). The accepted explanation for this is that the eyes and the mouth are the source of facial expression, which radiates the emotional status of the person. The centrofacial area harbors the emotional expression of the face, which explains the importance of restoring it.
It is not only the appearance of old age, but also the physical appearance of fear, grief, pain, doubt, fatigue, and other negative states that people wish to remove with the help of a facial rejuvenation procedure. A simple cervicofacial lifting procedure, which only affects the neck and the peripheral parts of the face, cannot change this emotional expression of the face.
Combined with surgical correction of skin laxity, the various modalities of fat grafting have become an integral and indispensable part of the modern facial rejuvenation process. This chapter presents several cases in which the different modalities of facial rejuvenation worked synergistically toward a natural facial rejuvenation result. In all these cases the change in emotional expression of the face is obvious—in some it is even more important than the mere lifting procedure that works in the peripheral areas of the face. A striking example of centro-facial aging can be seen in the facial aging process of Fabiola de Mora y Aragón, late Queen of Belgium (1928–2014; Fig. 7-2).
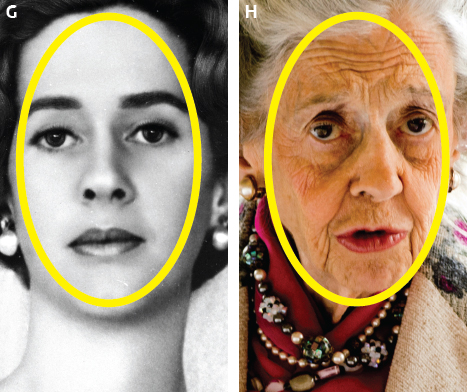
Despite the peripheral laxity in the jowls and the neck, the centrofacial volume loss in the perioral and the periorbital region are much more important with respect to the Queen′s emotional expression. The final comparison between age 32 (Fig. 7-2, G) and 86 (Fig. 7-2, H) highlights that the most important aging changes occur in the central oval of the face. This underscores the importance of centro-facial rejuvenation and the techniques described in this book.
CASE STUDIES
The 51-year-old woman in Fig. 7-3, a smoker, presented for a facial rejuvenation procedure (Fig. 7-3, A). After the consultation she decided to postpone the surgery and underwent a gastric bypass procedure because she felt slightly overweight. She lost 20 kg in 3 years; the result of the weight loss on her facial appearance was evident—she appeared to have aged 15 years in the 3-year period (Fig. 7-3, B). At that time, at the age of 54, she again presented for facial rejuvenation. Compared with her appearance at the age of 28 years (Fig. 7-3, C), the centrofacial deflation is obvious in her upper eyelids, midface, and perioral area. Sagging of the peripheral area is visible, with drooping of the tail of the eyebrow, loss of definition of the jowl line, and neck laxity with platysmal bands, especially on the left side. Fine wrinkles in the frontal, glabellar, and perioral area appear together with a lengthening of the vertical height of the upper lip and loss of definition of the lip contours.

Nonsurgical Plan
The nonsurgical treatment plan consisted of the following:
Smoking cessation
A Retin-A skin care program
Botulinum toxin in the glabellar and frontal area
Surgical Plan
The surgical treatment involved the following:
Simple minimal access cranial suspension (MACS) lift with retroauricular incision
Open neck procedure with platysmarrhaphy and partial transection of the platysma at the level of the hyoid
Short-scar temporal lift
Upper augmentation blepharoplasty with skin-only resection
Lower skin-pinch blepharoplasty
Microfat grafting, 80 cc, harvested from the abdomen
– Infrabrow: 2 cc/side
– Malar: 13 cc/side
– Nasolabial fold: 1.5 cc (including 0.25 cc after subcision)
– Marionette grooves: 2.5 cc/side
– Sharp needle intradermal fat (SNIF), 21-gauge needle:
Upper white roll: 1.3 cc
Lower white roll: 1.0 cc
Philtrum: 0.4 cc
– SNIF, 23-gauge needle:
Barcode (upper lip): 1.2 cc
Frontal wrinkles: 2.0 cc
Glabella: 0.5 cc
Cheek rhytids: 2.3 cc
Nasolabial rhytids: 2.0 cc
Nanofat in the anterior neck area (17 cc)
Liplift
Postoperative Result
The 1-year postoperative result demonstrates the correction of the neck laxity with restoration of the cervicomental angle (Fig. 7-4). Mandibular definition is restored by correction of the jowling. The degree of platysmal banding required a platysmarrhaphy and consequently a full facelift incision. Most important was the correction of the volumetric deflation of the centrofacial area. Compared with her appearance at age 28 years, the rejuvenation is very natural, with the essential replenishment of the upper eyelids, the malar area, and the perioral area. The effect of the liplift is seen by the shortening of the vertical height of the upper lip. The SNIF to the white roll and the philtral columns restores the definition of the lip contours to her younger appearance. The glabellar and frontal rhytids are eradicated by the synergistic effect of botulinum toxin and SNIF. In the profile view in downward gaze (the Bruce Connell view), the restoration of the cervicomental angle and the stable correction of the platysmal banding are evident. The improvement in the quality of the neck skin is a result of the microfat in the horizontal rhytids and nanofat in the whole anterior surface of the neck.

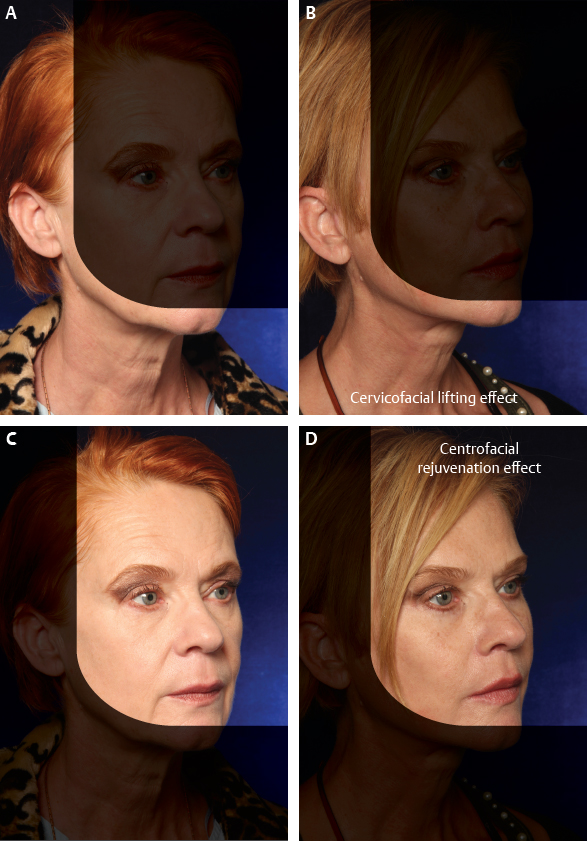
When the effect of the lifting procedure in the peripheral part of the face is compared with the effect of the centrofacial rejuvenation, the centrofacial rejuvenation is clearly much more important than the actual lifting procedure (Fig. 7-5). Both techniques work synergistically toward a total natural facial rejuvenation.
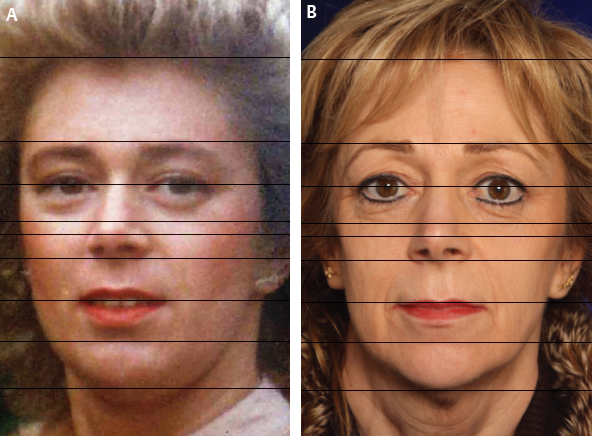
The woman in Fig. 7-6 consulted for facial rejuvenation at the age of 64 years. Analysis of and comparison with her picture at the age of 20 years reveals that the sagging component of her facial aging is moderate (mainly in the neck and jowls), whereas the deflation component is very marked, especially in the periorbital and perioral area. She has bilateral very lax lower eyelids, with a positive snap-back test. She shows an important deflation of the upper and lower eyelids, midface, and upper and lower lips, including loss of vermilion and philtral column definition. Positional analysis of the anatomic landmarks (pupils, orbitomalar groove, nasal tip, mental groove, and chin) shows that in the periorbital and midface regions, all anatomic landmarks stay exactly at the same position. The optical illusion of sagging is mainly caused by the important deflation taking place in these areas. The only feature that comes down in the central part of the face is the upper lip, where an obvious lengthening of the vertical height of the upper lip is visible in the aged face, which is a good indication for a surgical liplift. A marked change in emotional expression is also obvious between the young and the aged face.
In the preoperative photos, a slight inclination of the head on the cervical spine was obvious. When asked to put the head straight, she revealed that she was not able to do so, as she has a degenerative condition in the cervical vertebrae that has caused her to be in pain for the last 15 years. This pain is in part responsible for the emotional expression of the face. Changing this emotional expression was the most important mission of this facial rejuvenation case. This was planned with correction of the deflation in the periorbital and perioral region.
Nonsurgical Plan
The nonsurgical treatment plan consisted of the following:
A Retin-A skin care program
Botulinum toxin in the glabellar and frontal areas
Surgical Plan
The surgical treatment involved the following:
Simple MACS lift with limited postauricular dissection
Open neck procedure with platysmarrhaphy and partial transection of the platysma at the level of the hyoid
Short-scar temporal lift
Augmentation blepharoplasty
– Upper: skin-only resection plus microfat grafting
– Lower: fat redraping and microfat grafting of the malar area
Bilateral canthopexy
Microfat grafting, 65 cc harvested from the abdomen
– Infrabrow: 3 cc/side
– Malar: 10 cc/side
– Nasolabial folds: 2 cc, including 0.5 cc after subcision
– Marionette grooves: 3 cc/side
– SNIF, 21-gauge needle:
White roll, upper and lower: 2.0 cc
Philtrum: 1.0 cc
– SNIF, 23-gauge needle:
Barcode (upper lip): 2 cc
Nasolabial rhytids: 2.2 cc
Frontal wrinkles: 1.8 cc
Glabella: 0.7 cc
Nanofat in the perioral area (10.5 cc)
Liplift
Erbium-YAG laser resurfacing in the perioral area
Excision of tuberous nevi on left upper eyelid and upper lip
Postoperative Result
The 1-year postoperative result shows a stable correction of all the deflated areas (Fig. 7-7). This case illustrates the importance of adding volume in the central part of the face as part of a total facial rejuvenation procedure. The correction of the neck laxity and the restoration of the cervicomental angle is important, but in this case the centrofacial correction of the deflated periorbital and perioral areas is indispensable. The periorbital hollowness that occurred with aging has disappeared by the volumizing effect of the augmentation blepharoplasty. The aspect of the eyelids is very similar to that at age 20 years, with a full infrabrow area and a complete blending of the eyelid-cheek junction. This is a very different approach from the traditional resection blepharoplasty, which in her case would have made her eyelids tighter and more hollow but would not have resulted in a true rejuvenation.


Three-dimensional sculpting of the upper and lower lips was accomplished with several techniques: volume augmentation by microfat grafting and enhanced definition of the vermilion border and philtral columns; reduction of the vertical height of the upper lip by the liplift; and improved skin quality by laser resurfacing and nanofat injection. All these techniques work synergistically.
The 4-year postoperative pictures show the stability of the result (see Fig. 7-7, D, G, and J).
The woman in Fig. 7-8 presented at the age of 55 years for facial rejuvenation. When her current appearance was compared with a picture taken at the age of 20 years, the following features were observed:
Laxity of peripheral facial tissues, with temporal hooding, jowling, loss of mandibular definition, downward slanting of the oral commissures, and submental skin laxity.
Most striking is the centrofacial deflation with a periorbital, midfacial, and perioral loss of volume. The periorbital and midfacial deflation is most obvious in the medial part of the upper eyelid, the tear trough, and the flattened malar area. The perioral deflation appears as nasolabial folds, marionette grooves, and deepened oral commissures.
Vertical positional analysis of the anatomic landmarks of the face shows no change in position of most centrofacial features, except for the upper lip, which shows a discrete vertical lengthening.
Surgical Plan
The surgical treatment involved the following:
Simple MACS lift with a “hockey-stick” extension and a limited postauricular dissection
Submental liposuction
Short-scar temporal lift
Augmentation blepharoplasty
– Upper eyelid
Conservative skin resection
Microfat grafting of the upper eyelid sulcus: right, 1.6 cc; left, 1.7cc
– Lower eyelid
Augmentation of the malar area: 9 cc of microfat per side
Skin-pinch blepharoplasty
Microfat grafting, 35 cc, harvested from the abdomen
– Infrabrow: right, 1.6 cc; left, 1.7 cc
– Malar: 9 cc/side
– SNIF, 21-gauge needle:
White roll, upper and lower lips: 1.6 cc
Philtrum: 0.8 cc
– SNIF, 23-gauge needle:
Barcode (upper lip): 0.5 cc
Nasolabial rhytids: 1.2 cc
Nanofat in the perioral area (5 cc)
Erbium-YAG laser perioral resurfacing of individual rhytids with a 2 mm spot at 200 mJ
Liplift
Postoperative Result
The results are shown at 1 year and 4 years postoperatively (Fig. 7-9); the correction of the peripheral laxity by the surgical lifting procedures is evident: correction of the temporal hooding, restoration of the jawline definition, and correction of upper neck laxity. However, most of the rejuvenative effect is produced by the restoration of centrofacial volumes. In the periorbital area the augmentation of the infrabrow and malar area are obvious. In the perioral area the replenishment is achieved by deep layer microfat grafting and superficial SNIF and nanofat grafting.

This case illustrates very clearly the necessity of incorporating fat grafting in the surgical rejuvenation procedure. Classic resection blepharoplasty would not have restored the fullness of the periorbital area to its younger appearance. Many surgeons would propose a surgical midfacelift procedure for this patient. Although expert surgeons can produce consistently good results with midfacelift techniques, this procedure involves a prolonged recovery and a risk of very serious complications like scleral show and ectropion. Because the central part of the face ages by deflation and not by sagging, the midface should be filled rather than lifted. Compared with often complicated and dangerous midfacelift techniques, fat grafting of the midface is simple, is quick, has a swift recovery, and is very safe with regard to possible complications, assuming that the right technique and adequate instrumentation is used.
In this case the cervicomental lift procedure was responsible for about 20% of the total facial rejuvenation. The remaining 80% was produced by the centrofacial rejuvenation (periorbital and perioral fat grafting and laser resurfacing). The liplift is an integral and essential part of centrofacial rejuvenation, as illustrated in the postoperative result.
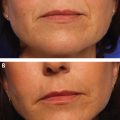
The woman in Fig. 7-10 presented at 55 years of age for facial rejuvenation. She had marked sagging of the cervicomental area, producing an obtuse cervicomental angle and obvious jowling. She had good zygomatic bony structure but some soft tissue loss in the anterior malar area and in the medial part of the upper eyelid (A-frame deformity) and the nasolabial groove.

Surgical Plan
The surgical treatment was performed under local anesthesia and involved the following:
Simple MACS lift
Submental liposuction
Short-scar temporal lift
Upper augmentation blepharoplasty with resection of skin only and fat grafting of the medial part of the upper eyelid (1.3 cc)
Microfat grafting (20 cc) of the upper eyelids (1.3 cc), nasojugal groove (0.4 cc), nasolabial crease (2.0 cc), marionette groove (2.0 cc), upper lip (0.6 cc), SNIF in the upper and lower lip white roll (1.3 cc), forehead rhytids (0.6 cc), upper lip (0.6 cc), nasolabial area (2.0 cc), and sublabial scar (0.8 cc)
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


