Chapter 1 The Role of Fat Grafting in Facial Rejuvenation
Many things that exist only in the imagination later become real.
G C
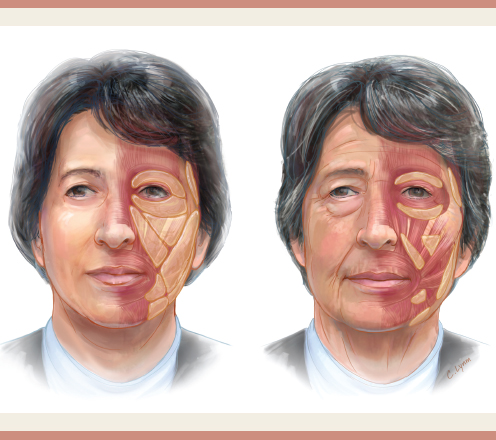
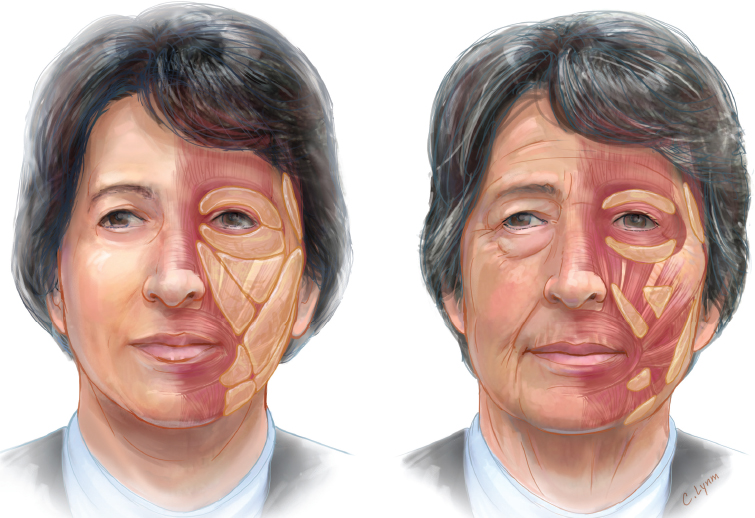
Surgical correction of aging-related sagging of facial structures has existed for more than 100 years. Nevertheless, during the aging process much more occurs than just sagging of the skin (Fig. 1-1). There are changes in skin texture and pigmentation and loss of volume in certain areas of the face (Video 1-1). Certain facial muscles contract, producing folds and rhytids, especially in the frontal area and the neck. All these factors must be considered when educating a patient about facial rejuvenation. If the treatment goal is a total and natural facial rejuvenation, the therapeutic plan must be a combination of different modalities individually adapted to each patient′s needs.
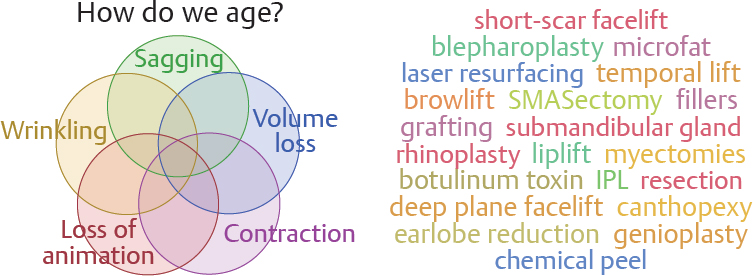
Sagging of facial skin can be corrected with a surgical facelift procedure. The options range from minimally invasive to deep plane or subperiosteal procedures. Surgeons can treat the eyelids, the eyebrows, the lips, and the neck; perform submandibular gland resection; or remove the adipose corpus of Bichat. The difficulty is not to master all the surgical techniques but to choose the right combination of procedures and to understand the correct indications for the different techniques. The texture and quality of the skin can be altered by skin care products with alpha-hydroxy acids or retinoic acid, light therapy such as intense pulsed light, or more drastically with resurfacing techniques such as dermabrasion, a chemical peel, or CO2 or Erbium laser resurfacing. Muscle hypertrophy or hypertony can be treated with surgical myotomies, selective neurotomies, or less invasive temporary chemical denervation with botulinum toxin. Volume depletion can be corrected with volumetric surgical techniques or by adding volume with a heterologous filler or autologous fat. Every patient must be carefully analyzed, and a personal treatment plan must be developed in consultation with the patient. The surgeon is personally responsible for choosing and combining the different treatment modalities according to the patient′s wishes, his or her personal experience, and technical training. For the past 20 years, we have always tried to use a combination of minimally invasive surgical techniques. The magic word in this context is “synergy” (Fig. 1-2).
COMBINING FACIAL FAT GRAFTING WITH FACELIFT PROCEDURES
The combination of fat grafting and surgical facelift is an example of synergy. Performing facial fat grafting alone can produce certain results, whereas surgical facelift procedures have certain other effects. However, the combination of these two can achieve results that cannot be obtained by either option alone. The addition of volume in the routine treatment plan of patients undergoing surgical facial rejuvenation deserves special attention and is the subject of the first part of this book.
Historically, surgical facial rejuvenation techniques have evolved from a skin tightening procedure into a subcutaneous sculpturing and skin redraping procedure. In the late 1980s and early 1990s, some surgeons such as Ramirez et al1 and Little2 focused on “volumetric” facelift techniques; the intent was to preserve or enhance the volume in the midface. However, Coleman3 popularized the technique of surgical fat grafting in the early 1990s. The idea of fat transfer was not really new, because this was already proposed 100 years earlier by the German surgeon Neuber.4 Nevertheless fat transfer did not become popular and was infamous for a high resorption rate and inconsistency of the final result.
Coleman standardized the technique of fat harvesting by using liposuction with specifically designed cannulas, fat preparation by centrifugation, and fat injection with specialized fine blunt cannulas; his technique turned fat transfer into a reliable and efficient tool in the plastic surgeon′s daily practice. Today the introduction of lipofilling in the surgical armamentarium of the twenty-first century plastic surgeon can be seen as a real landmark in plastic surgery, similar to the way breast implants were in the 1970s, endoscopy in the 1980s, and microsurgery in the 1990s. We started to occasionally incorporate fat grafting in facial rejuvenation procedures in 2002 and since 2008 have routinely used fat grafting as an ancillary procedure at the same time as facelift in about 95% of our cases. We routinely use fat to augment the periorbital, malar, and perioral region with different techniques.
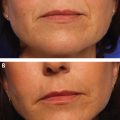
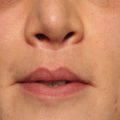
Facial Sagging Versus Facial Deflation
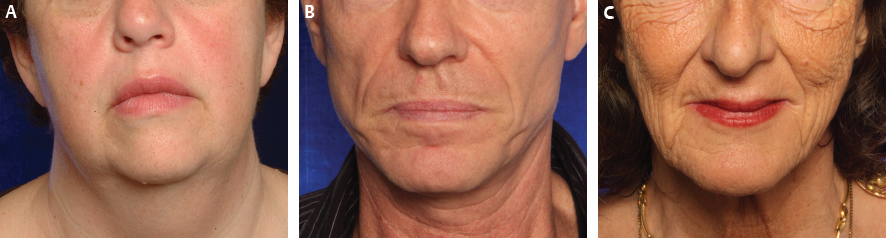
Understanding the importance of facial fat grafting in facial rejuvenation depends on understanding the difference between facial sagging and facial deflation. Facial sagging occurs at the periphery of the face, for example, lateral to the lateral canthus and oral commissure, and continuing in the neck (Fig. 1-3, A). Facial deflation takes place in the central part of the face, such as the periorbital region, including the glabella and the eyelids, the malar area, and the perioral region (Fig. 1-3, B, and Video 1-2). This is exactly the region where most mimic musculature is present and most movement occurs in the face. The superficial changes in the skin surface quality are independent from both sagging and deflation and take place on the whole facial skin (Fig. 1-3, C).
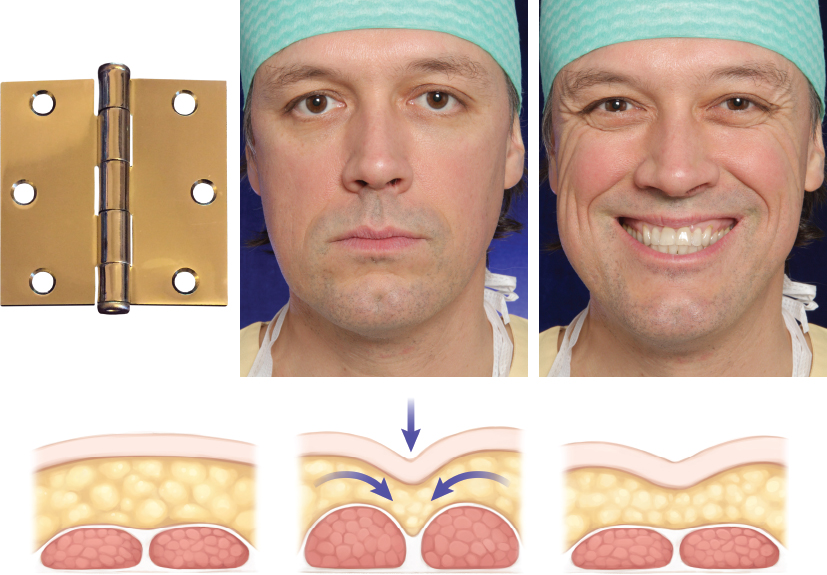
The Hinge Hypothesis
Based on our observations we hypothesized that facial fat atrophy could be caused by a pure mechanical factor; for example, a piece of paper will show atrophy in the region where it is folded over and over again for a certain time interval. In this context we introduced the hinge hypothesis of facial fat atrophy 5 (Figs. 1-4 and 1-5). This hypothesis postulates that fat cells atrophy under high pressure. This can be observed clinically in skin overlying tissue expanders, in which subcutaneous fat atrophy is seen in the expanded flap.6 This also occurs in the subcutaneous tissue of the skin under an abdominal belt. The only peripheral facial area where significant volume atrophy can be observed is the temporal area, overlying the temporal muscle.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


