Chapter 3 Augmentation Blepharoplasty

When the wind of change blows, some seek shelter while others build windmills.
H
Loss of fat tissue is an important cause of physical aging of the face. Clinical findings reveal that most deflation in the face takes place in areas where most movement from muscle activity occurs, namely the temporal areas and in the central part of the face.
THE CONCEPT OF AUGMENTATION BLEPHAROPLASTY
The concept of augmentation blepharoplasty is based on the hypothesis that periorbital aging is essentially a deflation phenomenon. This has led to a paradigm shift from resection toward filling in periorbital rejuvenation. A paradigm is a collection of generally accepted principles, methods, assumptions, and techniques that have proven themselves over time and are passed on to different generations. Working within a paradigm produces a certain comfort level, because everyone agrees on the method and philosophy being applied. Nevertheless, the accumulation of unsolved problems can change the value of an existing paradigm. New solutions from outside the accepted framework (“out of the box”) can then lead to a migration from the old paradigm to a new one. This is exactly what has taken place regarding the need for extra volume in periorbital rejuvenation.
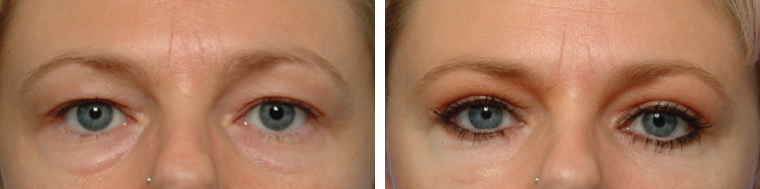
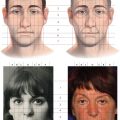
Traditionally blepharoplasty is a resection operation in both the upper and the lower eyelid. Eyelid skin can be resected, either with or without orbicularis muscle and fat from one or more compartments. As a consequence, classic resection blepharoplasty can lead to hollow, excavated and empty eyelids, whereas youthful eyelids are mostly full and crisp and rarely hollow (Fig. 3-1).
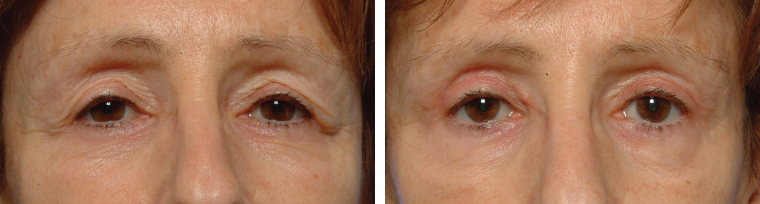
As aging continues, the eyelids continue to deflate and an apparent skin excess develops. Because skin growth likely is not occurring in that region, the skin excess can be seen as an optical illusion provoked by both the deflation phenomenon and the descent of the tail of the eyebrow. The deflation phenomenon is a gradual and continuous process. Analysis of photographs of very old people (80 to 100 years) reveals almost all of them have hollow eyelids (Fig. 3-2). Even in the presence of a bulging medial fat pad, a hollowing in the apex of the eyelid can be observed, often referred to as the A-frame deformity. Failure to correct this will result in an incomplete rejuvenation of the eyelid.
The descent of the tail of the eyebrow is known as temporal hooding and is explained by the lack of muscular suspension from the frontal muscle in its lateral part. The logical way to rejuvenate the upper periorbital region is thus to suspend the tail of the eyebrow by a temporal lift together with filling the hollowness below the supraorbital rim. Skin resection can be limited to a small strip of skin without resecting any orbicularis muscle to preserve as much volume as possible.
The classic lower eyelid blepharoplasty is even more problematic because of the risk of changing the shape of the eye opening, causing scleral show or even ectropion. This can originate from cicatricial retraction of the midlamellar structures or from excess skin removal. The fat bulging in the lower eyelid compartment is classically resected by a transcutaneous or transconjunctival approach. This corrects the puffiness of the lower eyelid, but it does not change the marked eyelid-cheek junction. Fat-conserving techniques have been described that involve transposing the herniating orbital fat over the orbital rim in an attempt to blend the eyelid-cheek junction. Generally, the aging eyelid deformity is accentuated by the deflation of the midface or malar area below the orbit. Most of this deflation takes place in the anterior malar area medial to the lateral canthus. This is logical in relation to the “hinge hypothesis,” which states that most deflation takes place in a region overlying the mimic muscles (see Chapter 1). A logical correction of the lower eyelid aging deformity is to add volume to the deflated malar area, especially in its anterior part medial to the lateral canthus. This can be combined with a resection or transposition of the bulging fat from the lower eyelid compartments over the inferior orbital rim.
In 2003, on the basis of studies by Trepsat,1 Lambros,2,3 Little,4 Roberts,5 and Benslimane,6 we began using fat grafts to address periorbital aging, gradually incorporating the correction of volume loss into standard orbital rejuvenation procedures. Since 2008 we have been using this revised approach, which now incorporates fine-particle fat grafting (microfat grafting) in 95% of cases. This was published in the Aesthetic Surgery Journal as augmentation blepharoplasty.7
Similar to the term augmentation mastopexy in breast surgery, the term augmentation blepharoplasty refers to the two components of the surgical procedure: the addition of volume and the resection of skin. Unlike classic resection blepharoplasty techniques, our approach is based on maximal preservation of all existing volume, along with correction of volume loss in the eyelids and the periorbital region by means of microfat grafting and conservative trimming of excess skin.
PATIENT EVALUATION AND SELECTION
Rejuvenation involves restoring a youthful, fresh, or untarnished appearance. In aesthetic surgical terms this means making patients look younger. We routinely ask all blepharoplasty and facial rejuvenation patients to bring pictures taken at a younger age (20 to 30 years), and these are analyzed during the preoperative consultation. Because of the different mechanisms that influence facial aging (such as sagging, deflation, wrinkling, contraction, and loss of animation) and because facial aging is not the same in every patient, accurately imagining a patient′s younger face without these pictures of the patient at a younger age is impossible.
The Upper Eyelid
Critical analysis of the pictures of patients at a younger age reveals that there is nearly always a certain degree of volume loss in the upper eyelid, especially in the medial part. This was earlier described as the A-frame deformity.8
Classic resection blepharoplasty removes the apparent excess of upper eyelid skin and orbicularis muscle with or without emptying of the medial and lateral fat compartments.9,10 This approach will rarely restore the features of youth if volume loss is not addressed. A browlift traditionally completes the classical resection blepharoplasty.11 In most cases, however, a hollowing of the upper eyelid occurs with ongoing aging. Therefore the postoperative result does not always resemble the full upper eyelids most patients have in their 20s and 30s.
The Lower Eyelid
Analysis of a patient′s pictures at a youthful age also reveals that most patients experience a loss of volume in the malar area, especially in the anterior part, even those who have gained some weight in recent decades. The malar area typically supports the lower eyelid; therefore volume loss in this area will accentuate the appearance of the “bags” in the lower eyelid. In traditional lower eyelid blepharoplasty, fat is removed from the medial, median, and lateral compartments, with or without suspension of the orbicularis muscle and trimming of the lower eyelid skin.12 Although the bulging of the lower eyelid is temporarily corrected, the blending of the eyelid-cheek junction is seldom improved, especially as further deflation of the malar area takes place with aging.
These shortcomings thus decrease the rejuvenative value of standard resection blepharoplasty techniques.
INDICATIONS AND CONTRAINDICATIONS
Deflation is an integral part of the aging process. Consequently volume restoration is necessary in almost every aged eyelid situation. This is the true expression of a paradigm shift. Once one learns to analyze the aging eyelid properly, a deflation can be discovered in nearly all situations. Aesthetic surgeons have a responsibility to recognize this condition, to point it out to the patient, and to take the necessary measures to treat it. Volume restoration by microfat grafting is imperative in periorbital rejuvenation.
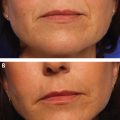
An isolated skin redundancy can be found in a small subpopulation of young people who have a familial eyelid laxity. In those cases a pure skin resection may still be indicated (Fig. 3-3). When deflation has not yet occurred as a consequence of the aging process, such as in very young patients (younger than 35 years), a conservative skin excision may be sufficient.
Once deflation begins a classic resection blepharoplasty will result in more tarsal show, but an aged, deflated eyelid will remain (Fig. 3-4). Many patients specifically ask to remove skin and to make the eyelids “tighter.” It is very tempting to limit the correction to excision of the apparent skin excess, and like many surgeons we have been doing this for many years, with often disappointing results, because it makes the patient look different but often not younger.
Contraindications specific to this procedure are very rare. Classic surgical contraindications such as bleeding disorders, smoking, and severe systemic disease apply.
PREOPERATIVE PLANNING AND PREPARATION
Middle-aged patients may require an ophthalmologic workup for lacrimal insufficiency and to evaluate eye globe pressure. Antiplatelet drugs should be discontinued 10 days before surgery. Smoking is detrimental for fat graft survival and should be stopped 3 weeks before surgery. The patient is given the option of a local anesthetic or a general anesthesia for the surgery. Contact lenses cannot be worn during the first postoperative week.
SURGICAL TECHNIQUE
Upper Eyelid
Markings
The skin excess is marked preoperatively in red with the patient standing or sitting (Video 3-1). The supratarsal crease in the upper eyelid is marked with the eyes closed. The patient is then asked to open the eye and gaze straight ahead. The upper limit of the skin excess is marked at the level of the supratarsal crease. With the eyes again closed the skin excess to be excised can be seen between the two markings.
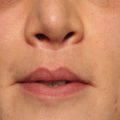
The area to be augmented is marked in green preoperatively with the patient in the upright position (Fig. 3-5). This area typically comprises the medial one half to two thirds of the infrabrow region and often incorporates the lower third of the medial part of the eyebrow. Eyelid fat grafting is a confusing and anatomically incorrect term; the fat is not injected into the eyelid proper, but rather into the infrabrow region extending under the upper orbital rim. The extent of this area depends on the hollowness of the upper eyelid in comparison with how it appeared when the patient was younger.

Anesthesia
The area marked in green (see Fig. 3-5) is infiltrated in a deep layer beneath the muscle with a lidocaine and adrenaline solution (minimal access cranial suspension [MACS] lift solution, containing 0.3% lidocaine and 1:600,000 adrenalin) together with subdermal infiltration of the marked upper eyelid skin excess.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


