Chapter 10 Aesthetic Contouring of the Upper and Central Third of the Face With Soft Tissue Fillers
True beauty is mesmerizing—it knocks you out and leaves you breathless.
W T.L. W
Soft tissue fillers have become one of the most popular techniques for nonsurgical facial rejuvenation and contouring in the last 2 decades. Originally conceived to smooth nasolabial lines and plump up lips, they are now used for a variety of purposes, including volumetric restoration and sculptural aesthetic contouring of the face. The brow, upper eyelids, forehead, and temples are important components of overall facial aesthetics, and volume improvements in this region can bring about significant changes. Technically, although the nose is not part of the upper third of the face, its origins are in this area, and it has important connections to structures in this facial region. This chapter examines the aesthetic considerations of the upper third of the face and presents my injection rationale and techniques. Vascular territories and potential complications are also discussed.
Injecting soft tissue fillers into the face is a growing phenomenon worldwide that has become one of the most important nonsurgical techniques employed by doctors who provide aesthetic facial treatments.1,2 Any physician who performs this procedure must have proper injection technique to correctly assess the effects of volume loss or volume requirement in all parts of the face and to treat any complications in a safe and competent manner.
Emphasis has previously been on volumetric restoration of the lower two thirds of the face, including the infraorbital area, malar eminences, cheek hollows, chin, nasolabial and marionette lines, with scant attention paid to the nose, upper eyelids, brows, forehead, and temples.3 However, better analysis of volume loss in the upper third of the face and its effect on aging has made the importance of this area for total facial rejuvenation obvious. Volumization of the upper lids and forehead have only become fashionable in the last decade, with the growing awareness that sunken hollow eyelids and flat bony foreheads are extremely aging and unaesthetic. Aesthetic contouring of the upper face therefore brings about significant aesthetic improvements, creating balance and harmony with the rest of the face.
AESTHETIC CONSIDERATIONS OF UPPER FACIAL CONTOURING
Although the nose, supraorbital brow ridge, upper lids, forehead, and temples are separate aesthetic units that can each be contoured independently, these five areas are connected to each other and should flow seamlessly from one to the other, creating a balanced, harmonious, and aesthetically pleasing upper face. In the study of faces nothing is more important than the shape of the forehead and nose, because these convey connotations of that person′s character, morals, and virtues—or lack thereof. These areas also display distinct differences between the sexes, with males having strong nasal bridges that meet low-set, prominent brow ridges at a more acute angle and a shorter forehead that can be straight or mildly convex. Invariably men should have a modest suprabrow concavity that highlights the projection of the brow ridge and gives a more masculine and rugged appearance.
For women, the sides of the nose, which should be smaller and more petite, should obliquely and gently curve into the medial aspect of the eyebrow (nasoorbital or dorsal aesthetic lines), which then continues smoothly over the supraorbital ridge to its lateral aspect without any undulations. The supraorbital brow ridge should be flat and indistinct, flowing convexly upward into a forehead that is high, wide, and slightly rounded. The forehead in turn should blend in with the temples laterally, which should be flat or mildly concave. Severe hollowness of the temples leads to lateral brow ptosis and a sickly appearance. Volume replacement of the temples elevates the lateral brow and lends the face a healthy appearance. Conversely, the temples should not bulge convexly. Absence of a suprabrow concavity confers a more feminine appearance.
Of course these are mere generalizations, and many variations are considered aesthetically acceptable, but these ideals emphasize the importance of the upper face as an area for cosmetic contouring and completing the visual perception of a face.4–8 Furthermore, in all races, sunken upper eyelids with A-frame deformities give the face an aged and unappealing appearance. The recent trend in facial rejuvenation is the identification of these disturbing facial hollows and correcting them with volume replacement.9
Historical Context
Before reliable soft tissue fillers for facial contouring were developed, a variety of surgical techniques were used to aesthetically improve these areas of the upper face. Fat grafts from the lower lids (by surgical excision) or periumbilical area (by surgical excision or liposuction) have been used to fill out sunken upper eyelid sulci.10 Silicone and, later, bone substitute implants were used for decades for elevating the nasal bridge and reshaping the forehead. Periosteal and temporoparietal fascial flaps have been used to smooth forehead irregularities, and more complex craniofacial operations have been used to burr down the supraorbital ridge and recontour the anterior wall of the frontal sinus. However, all of these procedures require large incisions and involve significant downtime. Autologous fat injections have in recent years been used to volumize and contour these areas successfully, but this remains a surgical procedure with a degree of unpredictability and potential risk of vascular occlusive complications. Good results with fat injections require excellent surgical judgment and skill. Complications are difficult to reverse.
INDICATIONS AND CONTRAINDICATIONS
Soft tissue fillers are indicated for patients who wish to achieve significant aesthetic contouring of the nose, brow, and forehead with minimal to no downtime. Often used in conjunction with botulinum toxins in the glabellar and forehead regions, significant aesthetic changes can be made within several minutes in the comfort of a nonsurgical setting. The techniques are easy to learn, and with proper precautions and judgment the results can be very satisfying and complications can be minimized. Large volumes (several vials of filler) can be used in a single sitting, with pain relief provided by local nerve blocks or by the lidocaine that is present in many top-grade fillers.
Contraindications for filler injections in this area are patients with unrealistic expectations, patients who have had multiple previous surgeries (especially open rhinoplasties, because the subsequent altered blood supply may result in tissue necrosis), and patients who have not been made aware of the potential complications.
The appropriate type of filler is chosen based on the patient′s concerns. Some patients want only the dorsum and tip of the nose to be reshaped, whereas others may want to enhance the nasoorbital line and the columella as well. Others may wish to contour the forehead and fill in the temples at the same time, and therefore a variety of different fillers of varying hardness may be used. Permanent fillers should not be used in any of these areas; only hyaluronic acid fillers should be used so contour irregularity or vascular complications can be potentially reversed.
PREOPERATIVE PLANNING AND PREPARATION
Whether to use a cannula versus a sharp needle to deliver the fillers is largely a personal preference based on familiarity and practice with the chosen instrument. With experience, equally good results can be obtained using either technique.11 Some physicians use both techniques in different areas of the face. I prefer the sharp needle technique using a 0.5 inch 30-gauge needle for most fillers used in the face regardless of whether it is the upper, middle or lower third of the face. The 30-gauge needle slows down the flow of injection, creating a greater awareness of the effect of volumization, and reduces the risk of overfilling and injecting under high pressure. With a 30-gauge needle, the fillers can be delivered directly and accurately to the desired target and in the correct plane, which in most situations should be directly onto bone. The underlying vascular anatomy must be considered to minimize the risks of vascular compromise. Occasionally, a 30-gauge cannula is used to deliver the softer fillers to the upper lids, brow, and forehead. Consistent injection is difficult on bone with a cannula, because cannulas invariably glide in the plane of least resistance, which in the forehead is subgaleal or intramuscular. This is the plane where the facial vessels, having emerged through their respective foramina, tend to arborize. The periorbital region must be injected carefully whether using a needle or cannula.
Safety Considerations
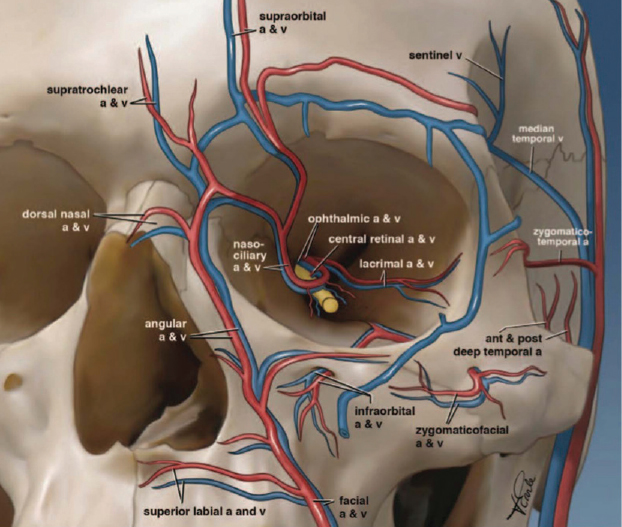
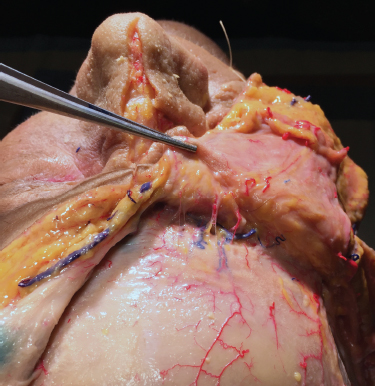
Vascular occlusion is the most serious complication of injecting any substance, whether fat or filler, in and around the orbits, glabella, and nose. Focal areas of skin and soft tissue necrosis, loss of vision from occlusion of the retinal or ophthalmic arteries, and even brain infarction have all been reported and remain risks that must be adequately discussed with every patient receiving these injections.12–22 A thorough knowledge of the vascular supply of the orbits and nose is essential (Fig. 10-1), noting the course of the facial and angular arteries, their branches to the nose, the branches of the ophthalmic artery as they emerge through the supratrochlear and supraorbital foramen, and in particular the anastomoses between these two systems.23,24
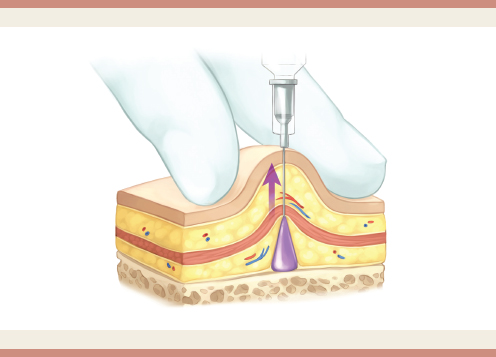
In the face, all arteries emerge from foramina and arborize in and on the overlying muscular layers, never in the interface between the periosteum and perichondrium and the facial and nasal muscles (Fig. 10-2).
Therefore the safest place to inject a filler in the upper third of the face and nose is on the bone or periosteum itself, ensuring that the supratrochlear and supraorbital foramina are first identified by palpation and protected from the needle point. The needle must not enter any of the facial bony foramina.
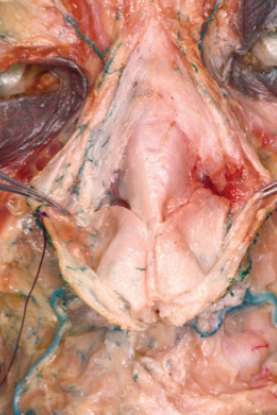
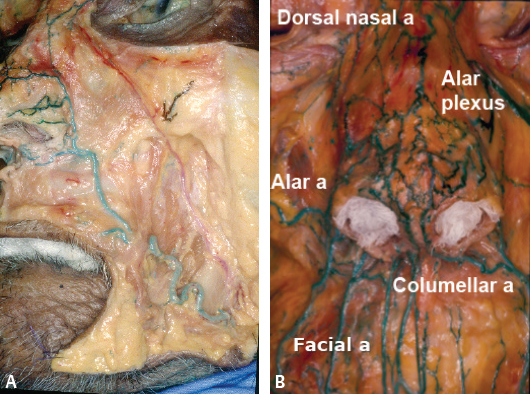
Over the nose, the arterial supply is paired with an alar, columellar (derived from the facial artery), and dorsal nasal (a branch of the ophthalmic artery) artery on each side, with a vascular watershed in the midline of the nose (Fig. 10-3). The midline of the nose is therefore an anatomically safe place for sharp needle injections, which should be placed directly on the underlying bone or cartilage of the nose.23
In the forehead the only anatomic constants are the supraorbital and supratrochlear foramina, which can be easily palpated and identified (Fig. 10-4). The supraorbital and supratrochlear arteries branch out over the central two thirds of the forehead in infinite variations, but they do so above the galea so similarly, the safest place to inject the filler is directly onto the bone itself.
VOLUMETRIC CONTOURING OF THE NOSE
The bridge, root, and tip of the nose are important areas for aesthetic shaping and rejuvenation in both Asian patients and patients of European descent. Younger patients require volume to contour and beautify the nose, correcting any structural deficiencies. Older patients, on the other hand, require volume to restore what has been lost. Ethnic considerations and the physician′s frequency of use of and familiarity with correct injection technique play a significant role in the choice of fillers.25
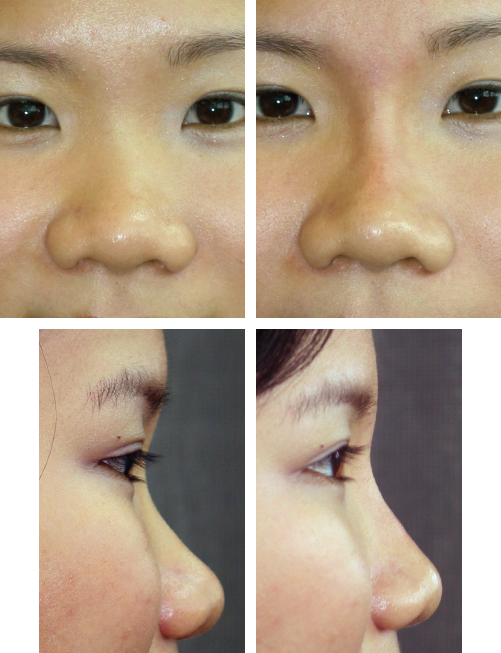
Asian noses are structurally flatter and broader over the dorsum and wide and fleshy over the tip. Fillers are commonly used to elevate the bridge, to replicate the effect of a columellar strut graft, and to project and to lengthen the tip (Fig. 10-5). The aesthetic considerations for injection rhinoplasty should be no different from performing a surgical augmentation rhinoplasty, with the fillers taking the place of either the implant or any cartilage grafts. To augment the dorsum, sharp needle injections should be delivered along the midline of the nose at the deepest possible plane. At the root of the nose, a carefully placed filler can raise the level of the “start point” of the nose and give the illusion of a longer, straighter nose. A small amount of filler placed lateral to the upper portion of the nasolabial fold can also displace the alar lobules medially, giving the impression of a narrower nasal base.
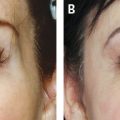
The noses of persons of European descent usually have sufficient dorsal height and tip projection but may have contour irregularities that can easily be smoothed with small amounts of filler.26–29 Narrow noses can be widened. The root of the nose becomes thinner and more attenuated with aging, and restoration of volume here has a significant rejuvenative effect. It also restores the smooth and continuous orbital-nasal lines of youth. Plunging nasal tips can be elevated with filler injected linearly from the anterior nasal spine, along the medial crura and into the tip. Patients with vertical glabellar lines or horizontal creases at the root of the nose indicate excessive muscular activity of the corrugator and procerus muscles and consequent volume loss (Fig. 10-6). Restoring the shape and volume of the nasal root and medial brow together with appropriate injections of botulinum toxin A to the affected muscles significantly reduces these lines and the appearance of an “old, pinched” nose.

Anesthesia
Before injecting in the nose, glabella, or periorbital regions, supraorbital and infraorbital nerve blocks are useful, using lidocaine 1% to 2% mixed with adrenaline 1:80,000 to 1:200,000. This not only provides pain relief but also vasoconstricts the blood vessels that accompany the nerves and may decrease the risk of vascular embolism. The local blocks are administered 10 to 15 minutes before the filler injections to allow adequate time for vasoconstriction to be achieved. Sometimes a blanching of the vascular territories can be seen. Placing an ice pack over the areas to be injected can also encourage vasoconstriction.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


