Chapter 8 Midface Volume Rejuvenation With Fillers
… thou know′st the mask of night is on my face.
W S
This chapter examines the layered anatomic array of the midface and translates these anatomic principles into consistent midface injection analysis and technique. The cadaver dissections, video demonstrations, and three-dimensional patient photography provide injectors with a comprehensive armamentarium to deliver accurate and reproducible results in midface volume rejuvenation with fillers.
INDICATIONS AND CONTRAINDICATIONS
Primary indications for midface volumizing procedures include generalized facial aging, volume deflation and displacement, diminished cheek projection, altered shape, deep rhytids, and camouflage of malar mounds (lymphatic collections in the superficial malar fat). Preprocedure preparation should incorporate a complete history and physical examination, documentation of drug allergies, and a listing of the patient′s current medications. Prophylactic medications such as antiherpetics, medications to decrease bruising, and a short course of postprocedure antibiotics need to be discussed during the consultation.
Relative contraindications to volumizing procedures include but are not limited to vascular malformations, trigeminal neuralgia, prior silicone injections, and a documented history of allergic reaction. Patients with autoimmune skin disease or history of excessive scarring should be examined carefully.
The Aging Midface
The addition of volume to restore deflated tissues and recessed bony structures requires a stereotaxic anatomic knowledge of the vasculature, ligamentous support, soft tissue spaces, and fat compartments of the face.
The aged appearance of the midface is the result of multifactorial processes. Val Lambros1 painted a great analogy of the aging midface when he wrote, “the midface behaves like a tectonic plate sliding down the face to form the nasolabial fold, leaving in its wake the nasojugal groove and the exposed and diminished malar eminence.” Beginning at the skeletal level, Kahn and Shaw2 demonstrated rotational changes of the orbit along with posterior retrusion and enlargement of the piriform aperture. Over areas of bony support and the masseter, the retaining ligaments of the face as described by Furnas3 prevent large-scale ptosis of the midface, chin, and lateral face. With age, these retaining ligaments become more vertically oriented. Lambros1 postulated that midface changes were largely volume related and not ptosis dependent. This has become accepted as the new paradigm guiding midface rejuvenation. Furthermore, the fat of the face has been recognized to occur in compartments, superficial and deep. The deep compartments are intimate with the mimetic muscles and neurovascular structures and reside deep to the superficial myoaponeurotic system (SMAS).4 The superficial fat compartments are separated by vascularized septae that are ligamentous in nature over the bony and masseteric supporting structures. Based upon adipocyte size, fat within the deep compartments is postulated to atrophy with age, whereas fat in the superficial compartment increases with age and obesity.5 The deep compartments of the midface contain three relevant anatomic spaces. Anatomic spaces are areolar in nature and are devoid of crossing neurovascular structures and ligaments.6–7
Volumization procedures should focus on reestablishing support in the “pillars of the face” that have resorbed, deflated, or become ptotic with age. A keen appreciation of the difference between deep and superficial layers of facial fat is paramount. Recognition of the gliding effect of superficial fat over deep fat with animation will assist the injector in aesthetic visualization of a patient′s face in youth.
Midface Anatomy for the Injector
Prezygomatic Space
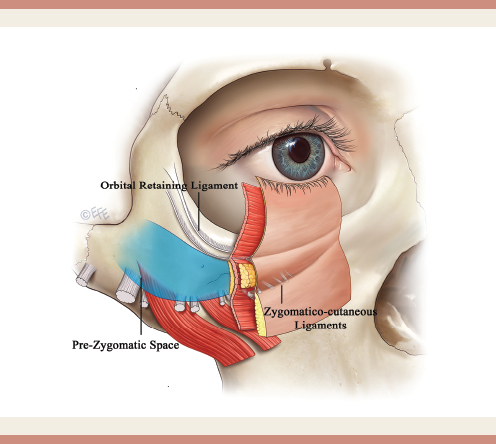
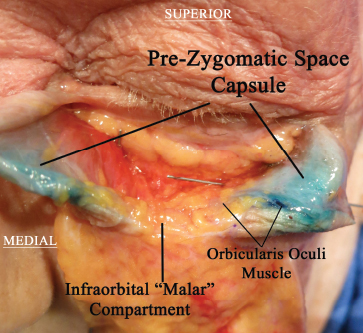
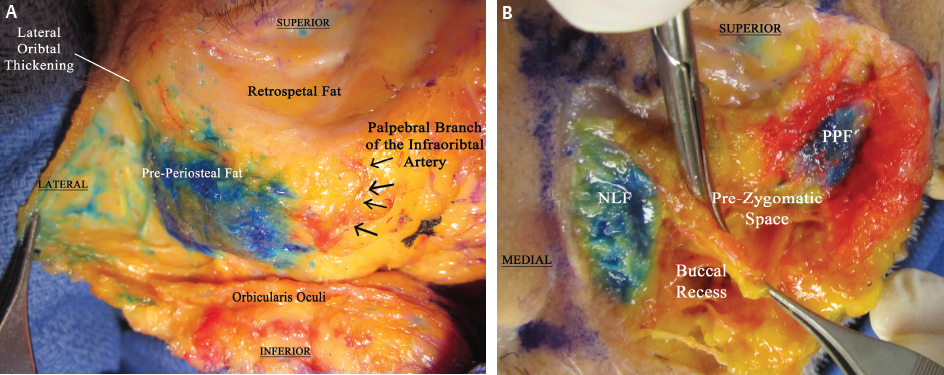
First described by Bryan Mendelson,6 the prezygomatic space lies between the orbital retaining ligament and the zygomatic retaining ligaments (Fig. 8-1 and Video 8-1). The space extends laterally in a cephalic direction to the lateral orbital thickening. The space is enveloped by a capsule analogous to the SMAS on the undersurface of the orbicularis oculi (Fig. 8-2). On the deep floor of the space resides the preperiosteal fat resting on the maxilla (Fig. 8-3) . This is a distinctly different plane than the more superficial suborbicularis oculi fat (SOOF). The SOOF is a loosely oriented fat pad residing between the prezygomatic space capsule and the posterior surface of the orbicularis muscle (Fig. 8-4).
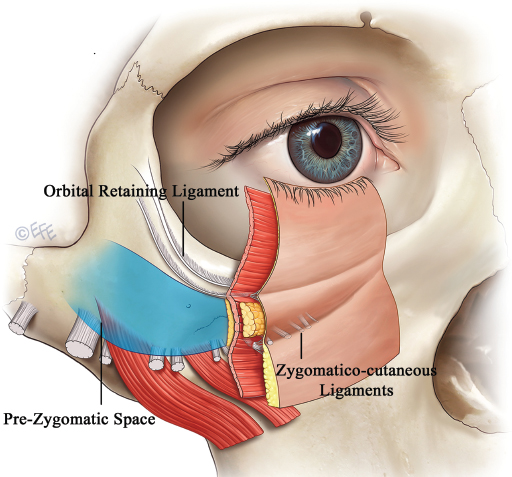
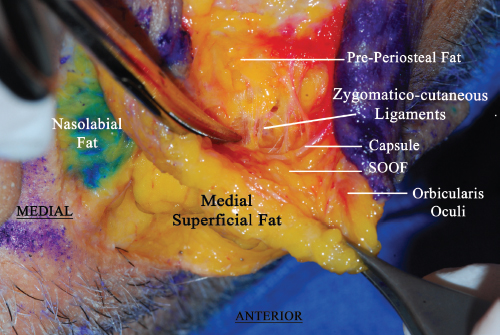
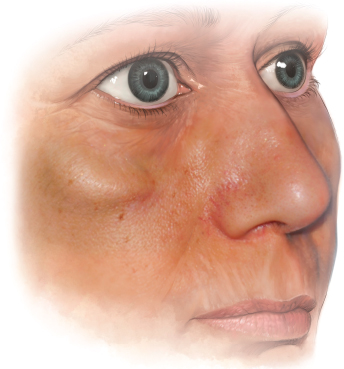
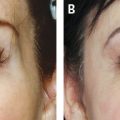
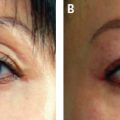
Several studies now document that there is an additional layer of fat superficial to the orbicularis oculi muscle. We believe this is the corollary to the “malar” fat pad whose traditional description refers to the fat pad above the orbicularis muscle. Therefore distinction must be made regarding this published malar or “infraorbital” fat pad. The fat pad is a superficial compartment and is separated from its caudal counterparts by the cutaneous insertion of the zygomatico-cutaneous ligaments (see Fig. 8-1). This compartment is believed to have poor lymphatic drainage, and injection into this region can be problematic, potentially resulting in an iatrogenic malar mound. Clinically we have seen retained lymphedema in this compartment after injection (Figs. 8-5 and 8-6; see also Fig. 8-1).

Regarding the prezygomatic space and its role in midface injections, an important point to consider is the dynamic gliding nature of the midface during facial expression. The prezygomatic space affords gliding motion of the superficial structures of the midface with smiling. In effect, contents placed in this space remain in a deep plane and in a consistent shape as the more superficial structures glide over it. In regards to the intimate vasculature, authors describe the junction of the lid-cheek crease and nasojugal groove as an identifiable topographic landmark for the infraorbital neurovascular bundle. An ascending branch of the artery traverses to the palpebral fissure in this region along with a small percentage of angular arteries that have detoured from their normal course; therefore great care should be exercised when performing superficial tear trough injections (see Fig. 8-3).
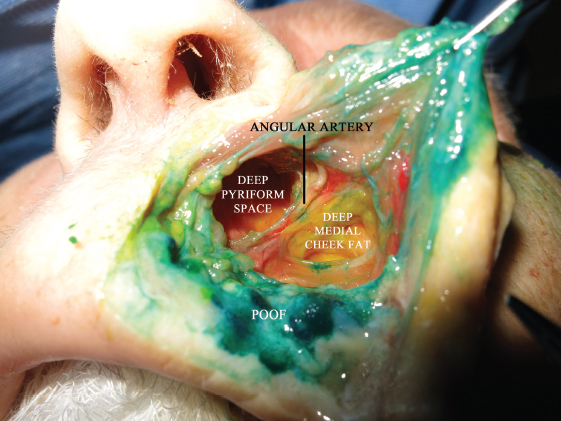
Premaxillary and Deep Piriform Spaces, Deep Medial Cheek Compartment
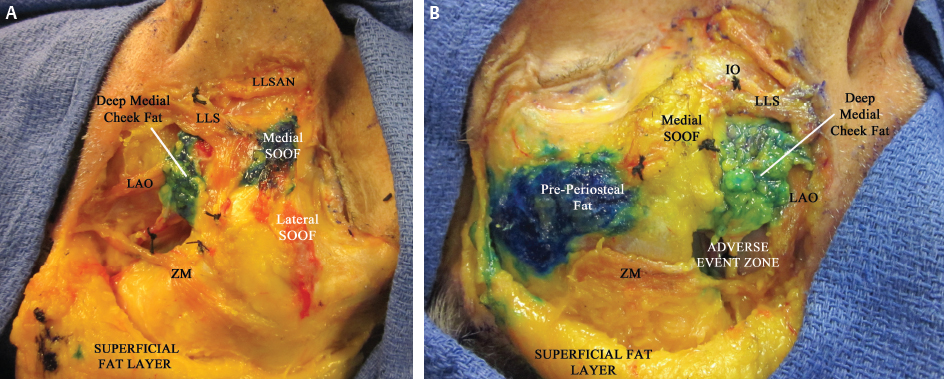
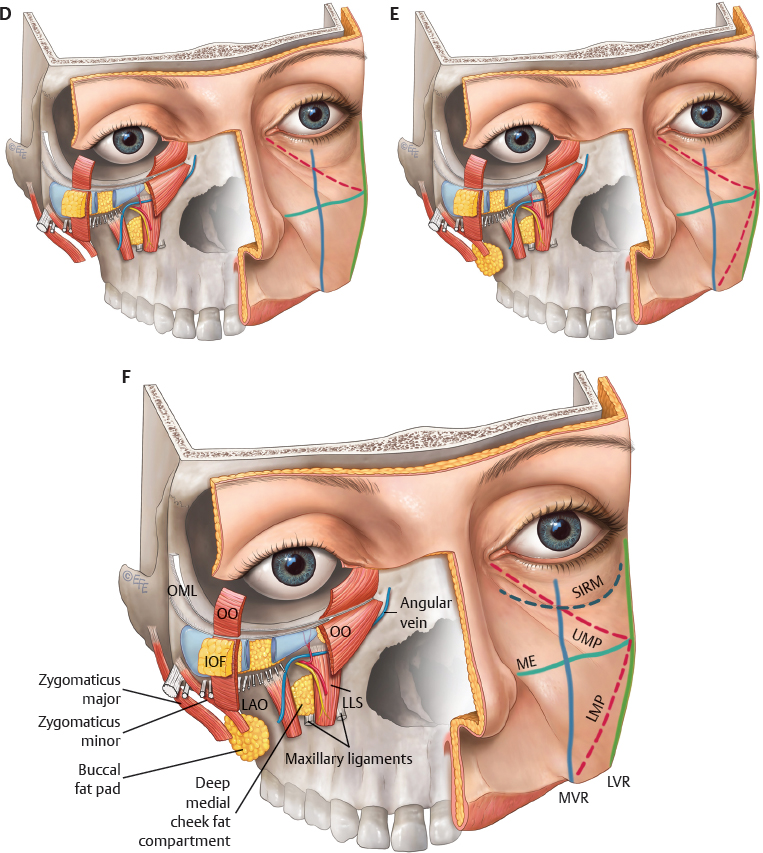
The deep medial cheek compartment overlies the maxilla and lies lateral to the deep piriform space (Figs. 8-7 and 8-8). The more lateral component of deep cheek fat traverses along the maxillary deflection and abuts the buccal space. Deep lateral injections in this region can be troublesome, because material can descend caudally into the buccal space (Fig. 8-9). We recommend more medially oriented injections in the deep piriform space or the medial component of the deep medial cheek fat. Immediately superficial to the levator labii superioris is the premaxillary space, which affords glide and muscle excursion immediately deep to the SMAS (see Fig. 8-8). The lateral boundary of the premaxillary space contains the angular vein.

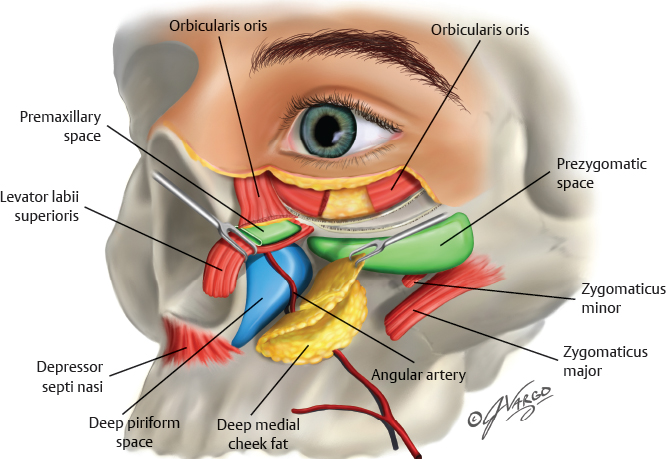
Both the deep piriform and the premaxillary spaces are devoid of crossing neurovascular and ligament structures. The cephalic extension of both spaces lies deep to the orbicularis oculi muscle and is superiorly bounded by the tear trough ligament.8 The angular artery is tethered to undersurface of the levator musculature and does not reside in the space (Fig. 8-10). Medial maxillary recession with age likely enlarges the deep piriform space, making it a plausible location to inject volume in a safe manner, because the vasculature is superficial to the space. In addition, volumizing of this space provides support for the draping lip elevators that traverse superficial to the space (see Fig. 8-8).
Superficial Medial and Middle Fat Compartments
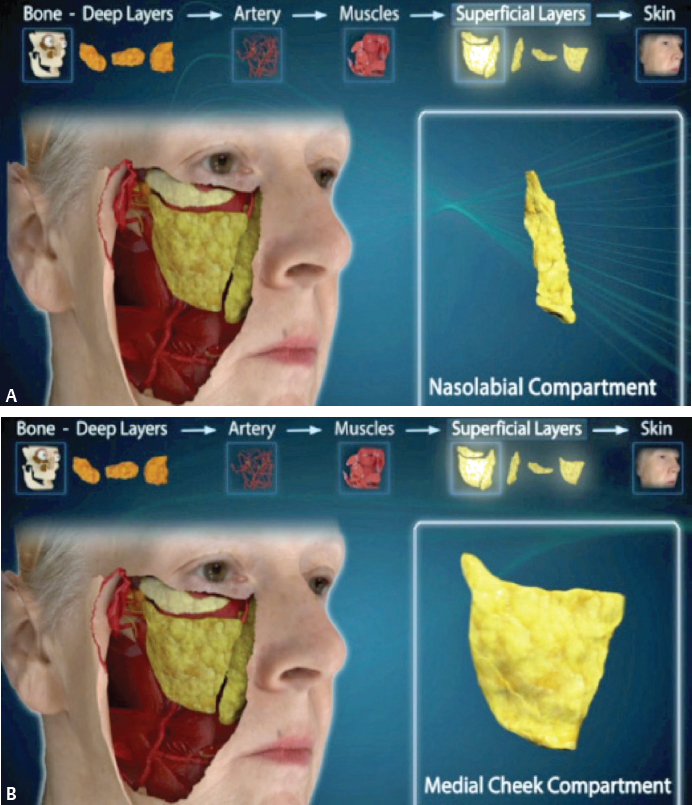
Three superficial fat compartments exist in the midface: the nasolabial, medial superficial, and middle superficial fat compartments (Fig. 8-11). Dense vascular septae divide these compartments. These septae can be readily felt with the end of a blunt cannula when injecting in the superficial fat of the face. These superficial fat compartments glide upward with facial expression. Volume placed within these compartments can restore turgor to the skin. Consideration is also given to the expansion of the Langer lines with superficial volumization, a technique that can alter cheek convexity.
PREOPERATIVE PLANNING AND PREPARATION
Many surgeons rely on their “aesthetic eyeball” to analyze and plan volumizing procedures. Although this method can be effective, we present an alternative approach using an anatomically inspired topographic analysis (Video 8-2). This method divides the cheek into “target areas” and “injection caution zones” using five basic markings (Fig. 8-12). We recommend reviewing the anatomy and analysis videos accompanying this chapter for a more detailed description of this planning approach.
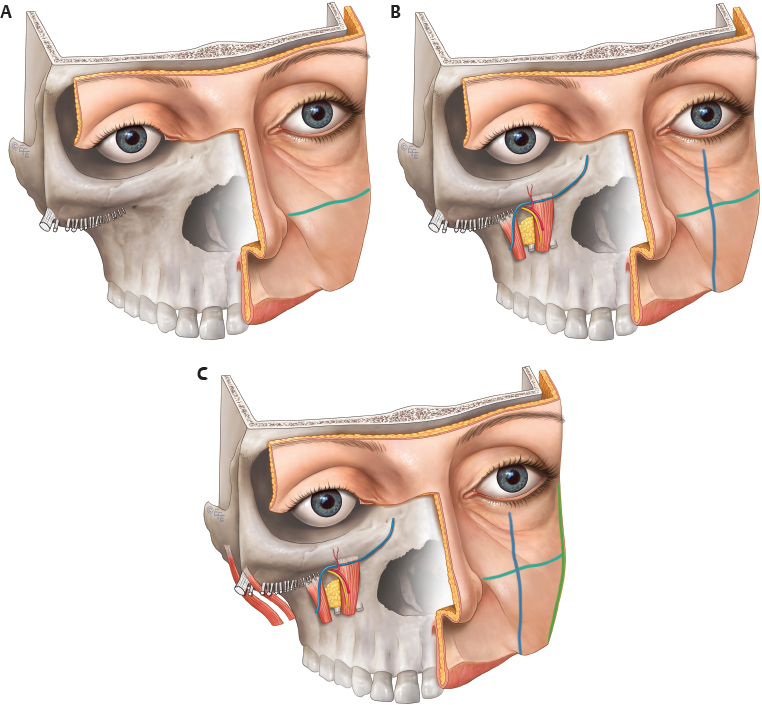
Topographic Analysis of Target Areas
Malar Equator
The midface is first bisected as a horizontal line drawn from the alar crease to the tragus. This line is the malar equator and anatomically corresponds with the zygomatico-cutaneous retaining ligaments and upper labial buccal sulcus. These anatomic landmarks distinctly separate the upper midface from the lower midface (see Fig. 8-12, A).
Related posts:
 Chapter 9 Filling Temples With Highly Diluted Hyaluronic Acid Fillers
Chapter 9 Filling Temples With Highly Diluted Hyaluronic Acid Fillers
 Chapter 11 The Microbotox Technique
Chapter 11 The Microbotox Technique
 Chapter 10 Aesthetic Contouring of the Upper and Central Third of the Face With Soft Tissue Fillers
Chapter 10 Aesthetic Contouring of the Upper and Central Third of the Face With Soft Tissue Fillers
 Chapter 2 Microfat Grafting
Chapter 2 Microfat Grafting
 Chapter 5 SNIF: Sharp Needle Intradermal Fat Grafting
Chapter 5 SNIF: Sharp Needle Intradermal Fat Grafting
 Chapter 4 Perioral Rejuvenation
Chapter 4 Perioral Rejuvenation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


