The normal skin of healthy infants and children is resistant to invasion by most bacteria, because the cutaneous surface provides a dry mechanical barrier from which contaminating organisms are constantly removed by desquamation. Under normal conditions the skin is sterile at delivery and for a short period thereafter. During the process of vaginal birth it acquires organisms from the birth canal, which gradually increase in number during the first 10 days of life. If the newborn is delivered by cesarean section, however, the cutaneous surface remains sterile until after delivery but soon becomes exposed to bacteria from human contactants and fomites.
Almost any organism may live on the cutaneous surface under appropriate conditions. A complete list of transient organisms accordingly would include virtually all microorganisms found in the human environment. The number of species composing the resident flora, however, is relatively small and consists predominantly of Gram-positive organisms and a few Gram-negative species, including Propionibacterium acnes (normally found in high concentrations about the pilosebaceous follicles of the face and less commonly the axillae and forearms), aerobic diphtheroids ( Corynebacterium minutissimum and Corynebacterium tenuis ), Staphylococcus epidermidis micrococci, and anaerobic Gram-positive cocci. Others include Gram-negative bacilli ( Escherichia coli , Proteus , Enterobacter , and Pseudomonas , among others) found uncommonly on normal skin except in the moist intertriginous areas of the groin, axillae, and toe webs and Staphylococcus aureus , a common pathogen that appears to usually be seeded from the carrier state in the anterior nares.
Because the cutaneous surface is continuously exposed to microorganisms, it is most helpful to distinguish among transient, resident, and pathogenic flora. The transient flora consists of multiple organisms that are deposited on the skin from the environment, presumably do not proliferate, and are removed easily by washing or scrubbing of the affected area. The resident flora consists of a smaller number of organisms that are found more or less regularly in appreciable numbers on the skin of normal individuals, multiply on the skin, form stable communities on the cutaneous surface, and are not easily dislodged. Pathogenic bacteria, not ordinarily a regular part of this flora, persist on the skin if there is continuous replacement from some internal or external source or if the integrity of the skin is disrupted by injury or disease. It should be noted that the mere presence of potentially pathogenic bacteria in a cutaneous lesion does not necessarily prove the demonstrable organism to be a cause of bacterial infection.
Children have a more varied cutaneous flora than adults and often harbor soil bacteria on their skin. Prepubertal children lack sebum and accordingly have fewer diphtheroid organisms than adults. It is estimated that 10% to 30% of individuals are nasal carriers of S. aureus and that 70% to 90% are transient carriers. Such coagulase-positive staphylococci are not considered part of the normal cutaneous flora of glabrous skin in adults but are common transients acquired from carrier sites such as the anterior nares and perineum. In a recent 1-year study of 333 healthy preschool children ages 3 to 6 years, 34% of nasal swab samples yielded S. aureus from 185 (55%) carriers, and based on consecutive genotype analysis, 15% of the children were classified as persistent carriers (the remaining were considered to be intermittent carriers).
The introduction of a vast array of antibiotics and chemotherapeutic agents has affected striking changes in the management of bacterial infections. With increased use of these agents the focus of attention has shifted to identifying the specific bacterial cause and its antimicrobial sensitivity pattern when feasible, permitting the appropriate choice of antibacterial agent(s). In purulent skin infections it is relatively easy to obtain adequate specimens for examination and culture. With dry or crusted lesions, the yield will be greatest if the crust is gently lifted off and cultures are obtained from the moist underlying surface. In nonpurulent infections like erysipelas or cellulitis, past recommendations were for aspiration of the most active zone (not the surrounding area of erythema) with a 25-gauge needle attached to a syringe containing sterile saline without added preservatives. This procedure, unfortunately, has a very high false-negative rate, and often the clinician in this setting is forced to rely on clinical features or other diagnostic findings.
Bacterial Infections
Impetigo
Impetigo is a common, contagious superficial skin infection caused by streptococci, staphylococci, or both. Although seen in all age groups, the disease is most common in infants and children. Lesions may involve any body surface but occur most often on the exposed parts of the body, especially the face, hands, neck, and extremities.
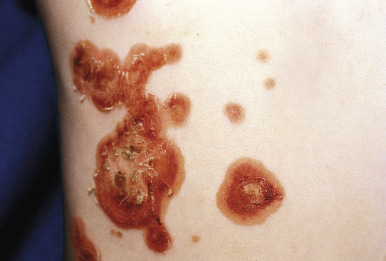
There are two classic forms of impetigo: bullous and nonbullous (or crusted). Nonbullous impetigo accounts for more than 70% of cases. It begins with a 1- to 2-mm erythematous papule or pustule that soon develops into thin-roofed vesicle or bulla surrounded by a narrow rim of erythema. The vesicle ruptures easily with release of a thin, cloudy, yellow fluid that subsequently dries, forming a honey-colored crust, the hallmark of nonbullous impetigo ( Fig. 14-1 ). The infection is easily spread by autoinoculation ( Fig. 14-2 ) through fingers, towels, or clothing, with resultant satellite lesions in either adjacent areas or other parts of the body. Individual lesions may extend peripherally with central clearing, resulting in annular or gyrate morphologies. Nonbullous impetigo historically was caused primarily by group A β-hemolytic streptococci (GABHS) but now appears to be most commonly caused by S. aureus . Anaerobic organisms may also be recovered from lesions of nonbullous impetigo.


Bullous impetigo, which is nearly always caused by S. aureus , presents as flaccid, thin-walled bullae or more commonly, tender, shallow erosions surrounded by a remnant of the blister roof ( Figs. 14-3 and 14-4 ). Common locations include the diaper region ( Fig. 14-5 ), face, and extremities. Lesions of bullous impetigo can be thought of as a localized form of staphylococcal scalded skin syndrome (SSSS) (see Staphylococcal Scalded Skin Syndrome section), the characteristic lesions being the result of the same exfoliative toxin as implicated in that condition. Neonatal pustulosis (see Chapter 2 ), another condition favoring the diaper region and other fold areas in infants, is usually caused by S. aureus and presents with small pustules on an erythematous base that rupture easily upon swabbing.


Fever and regional lymphadenopathy may occur later in the course of impetigo but appear to be more common with the nonbullous type caused by GABHS. Potential complications of both bullous and nonbullous impetigo include sepsis, osteomyelitis, septic arthritis, lymphadenitis, and pneumonia. Cutaneous streptococcal disease may be associated with guttate psoriasis, scarlet fever, and poststreptococcal glomerulonephritis when a nephritogenic strain of GABHS is implicated.
An important reservoir for staphylococci is the upper respiratory tract of asymptomatic persons. Asymptomatic nasal carriage occurs in 20% to 40% of normal adults and up to 80% of patients with atopic dermatitis. The perineum is another common site of carriage, albeit not as common as the nares. These carriers spread the agent to the skin of infants and young children, probably with their hands. The reservoir for streptococci involved in skin infections appears to be skin lesions of other individuals, not the respiratory tract of affected or asymptomatic persons. Factors such as trauma and insect bites probably contribute to the pathogenesis of this infection.
Treatment for impetigo depends on the clinical presentation. Untreated, the disorder may last for 2 to 3 weeks with continuous spread and development of new lesions. In severe cases there may be large, crusted vegetations with deep extension and ulceration. Gentle cleansing, removal of crusts, and drainage of blisters and pustules may help prevent local spread of disease. If crusts are firmly adherent, warm soaks or compresses are useful.
Topical antibiotics may be useful in the treatment of mild, localized disease caused by S. aureus . With streptococcal or more severe staphylococcal infections, however, systemic antibiotics produce a swifter response and fewer failures. Bacitracin, polymyxin, gentamicin, and erythromycin are all effective topical agents and are relatively nonallergenic. Bacitracin, however, is a potential contact allergen, and this should be remembered in patients treated with this agent who develop worsening erythema and evidence of contact dermatitis. In addition, treatment failures are common when bacitracin is used for impetigo. Neomycin is another effective topical agent, although reports of contact allergy have traditionally appeared to be more common with this agent than with other topical antimicrobials (see Chapter 3 ). Mupirocin exerts a high level of bactericidal activity against a broad spectrum of Gram-positive organisms including S. aureus and GABHS and has little or no potential for irritation, side effects, or cross-reaction with other antibiotics. It is effective against methicillin-resistant S. aureus (MRSA), although some resistance to mupirocin has emerged in recent years, especially after prolonged use. Some studies have demonstrated equal or greater effectiveness of topical mupirocin over oral erythromycin in the treatment of impetigo in children. Mupirocin is typically applied three times daily for 7 to 10 days. Nasal carriage of S. aureus may be reduced with the use of intranasal mupirocin, which should be considered in known carriers with recurrent impetigo or in the setting of epidemic outbreaks. Retapamulin, a newer pleuromutilin-class topical antibiotic for the treatment of skin and skin-structure infections, has been demonstrated effective against both S. aureus and GABHS and is another treatment option for localized impetigo. Retapamulin is also active against MRSA and many anaerobes, including Propionibacterium species, Bacteroides species, and Clostridium species. The benefits of retapamulin include its lower propensity toward the development of resistance and twice daily dosing.
Oral therapy for impetigo should be with an agent that covers both S. aureus and GABHS, because distinguishing between these etiologies clinically is often not possible. In areas with a low prevalence of erythromycin-resistant S. aureus , erythromycin ethylsuccinate or erythromycin estolate are reasonable options. If known erythromycin resistance is present in the community, alternative oral agents with a good track record include a penicillinase-resistant penicillin (i.e., cloxacillin or dicloxacillin), amoxicillin plus clavulanic acid, a first- (i.e., cephalexin) or second- (i.e., cefprozil) generation cephalosporin, clindamycin, or in some cases, other macrolide antibiotics (i.e., clarithromycin or azithromycin). Oral therapy is used by most clinicians when the involvement is more widespread and/or severe.
In severe or recalcitrant cases, skin swab for bacterial culture and sensitivity testing should be performed. The evolving epidemiology of community-associated MRSA (CA-MRSA) (see below) infection must be considered in this setting, as highlighted by multiple observations of the increasing prevalence of this pathogen. These patients often lack traditional risk factors for MRSA, and the isolates may be more susceptible to clindamycin and trimethoprim-sulfamethoxazole.
A review of the National Ambulatory Medical Care Survey data on office visits for impetigo from 1997 to 2007 revealed that a majority of the 4 million patients were treated by nondermatologists (pediatricians, internists, emergency room and family physicians), and systemic antibiotics were the most commonly prescribed therapy, followed by topical antibiotics. A recent Cochrane review found that topical mupirocin and topical fusidic acid (not available in the United States) were equally or more effective than oral treatment in the studies that met their inclusion criteria. This highlights a potential opportunity for physician education, because increased utilization of topical therapy for patients with more limited impetigo could decrease the morbidity associated with oral antibiotic treatment, in line with the principles of antibiotic stewardship.
Lesions of impetigo caused by GABHS are shallow and usually heal well, and rheumatic fever does not occur after streptococcal skin infection. In contrast, acute glomerulonephritis and scarlet fever can occur after cutaneous streptococcal infection. As in the case of nephritis after streptococcal pharyngitis, only certain serologic types, different from those producing nephritis as a sequel of streptococcal pharyngitis, appear to result in this complication of cutaneous infection. This complication is uncommon except for certain epidemics resulting from nephritogenic strains of streptococci. Although systemic antibiotics help eliminate cutaneous streptococci, they do not appear to prevent glomerulonephritis caused by streptococcal impetigo. In general, however, with the changing bacteriology and the fact that staphylococci are a more common cause of both types of impetigo, concerns about postimpetigo glomerulonephritis have been greatly reduced.
Methicillin-Resistant Staphylococcus Aureus Infections
The epidemiology of S. aureus skin and soft-tissue infections has changed over the last decade, with an increasing prevalence of CA-MRSA infections observed in both the United States and elsewhere. Since the initial descriptions of children lacking predisposing risk factors with CA-MRSA infection in the late 1990s, marked increases in S. aureus isolates with this characteristic were observed, both in endemic and epidemic forms. By the mid-first decade of the twenty-first century, up to 50% of community-associated S. aureus infections in many US centers were being identified as MRSA. Increases in the number of children hospitalized with MRSA infections have also been observed, but fortunately the mortality rate for these children remains low.
MRSA originated after the introduction of a mobile genetic element, staphylococcal chromosomal cassette (SCC) carrying the mecA gene, into strains of methicillin-sensitive S. aureus (MSSA). This gene encodes an altered penicillin-binding protein. In distinction to hospital-associated MRSA, CA-MRSA is generally classified as such when there is no history of prior MRSA infection or colonization, when the positive culture was obtained in the outpatient setting or isolated within 48 hours of hospitalization, and when the patient lacks an exposure history (i.e., to a healthcare facility, chronic care facility, or indwelling catheter). Molecular characteristics of the isolate are also useful in distinguishing the strains. Many CA-MRSA strains produce Panton–Valentine leukocidin (PVL), a toxin that kills neutrophils, although this toxin is also produced by some of the other more-sensitive strains of S. aureus . The exact role of PVL in CA-MRSA infections remains controversial, although it appears to be increasingly associated with follicular infections (see Furunculosis section).
CA-MRSA infections seem to disproportionately affect children, young adults, and individuals from ethnic minority and low socioeconomic groups. Spread is facilitated by crowding, skin-to-skin contact, skin compromise, and shared personal hygiene items. Cutaneous CA-MRSA infections are common in athletes, most notably collegiate football players. The potential clinical manifestations associated with CA-MRSA infection are listed in Box 14-1 . The constellation of disorders caused by infection with CA-MRSA have been grouped under the designation of skin and soft-tissue infections (SSTIs). Empiric outpatient therapy decisions for CA-MRSA infections should incorporate the type and site of infection, prevalence of the organism in the community, and local antibiotic susceptibility patterns. Abscesses (including furuncles and carbuncles), which are collections of pus within the dermis and deeper skin layers, are a common manifestation of CA-MRSA infection ( Figs. 14-6 and 14-7 ) and are most commonly located on the buttocks. Incision and drainage of abscesses is often useful and sometimes sufficient as monotherapy for purulent uncomplicated infections. However, better studies are required to determine the role of antibiotics in treating abscesses that have been adequately drained.
Skin/soft-tissue infections
Folliculitis
Furuncles
Carbuncles
Impetigo
Pustulosis (neonates)
Cellulitis
Abscesses
Paronychia
Staphylococcal scalded skin syndrome
Necrotizing fasciitis/myositis
Pneumonia/empyema
Lymphadenitis
Otitis media/externa
Osteomyelitis
Thrombophlebitis
Septic arthritis
Bacteremia
Pyelonephritis
Toxic shock syndrome
Endocarditis
Epidural abscess
MRSA, Methicillin-resistant S. aureus .


The most commonly utilized oral antibiotics in the United States are: trimethoprim-sulfamethoxazole, clindamycin, doxycycline, linezolid, rifampin, and the fluoroquinolones. Fusidic acid is also utilized in the United Kingdom, Australia, and other countries. Inducible clindamycin resistance has increased in recent years and should be considered when testing reveals clindamycin susceptibility and erythromycin resistance. In these instances, a “D test” should be performed and used to guide the choice of therapy. Management of colonization has been attempted with intranasal mupirocin and skin disinfection (i.e., with chlorhexidine washes), with variable success. Recently it was shown that persistent colonization with MRSA in outpatients is associated with increased household colonization pressure (colonization of household contacts). In addition, MRSA colonization and infection has been increasingly observed in companion animals, especially cats and dogs, and may serve as reservoirs for human infection.
Ecthyma
Ecthyma is a deep or ulcerative type of pyoderma commonly seen on the lower extremities and buttocks of children, and caused most often by GABHS. It may occur as small punched-out ulcers or a deep spreading ulcerative process. The disorder begins in the same manner as impetigo, often occurring after infected insect bites or minor trauma, but penetrates through the epidermis to produce a shallow ulcer. The initial lesion is a vesiculopustule with an erythematous base and firmly adherent crust. Removal of the crust reveals a lesion deeper than that seen in impetigo with an underlying saucer-shaped ulcer and raised margin ( Fig. 14-8 ). The lesions are painful and heal slowly over a few weeks, often with scar formation. When multiple, lesions of ecthyma may be confused with child abuse related to cigarette burns. S. aureus (including MRSA) may occasionally be cultured from the lesions, and epidemic outbreaks have been reported, occasionally in association with poststreptococcal glomerulonephritis or other systemic sequelae. Treatment consists of warm compresses and the appropriate systemic antibiotic.

Ecthyma gangrenosum is a cutaneous finding that may be seen in patients with Pseudomonas aeruginosa bacteremia. Most of the affected individuals have an underlying immunodeficiency (either congenital or acquired) or a history of cancer chemotherapy. There are reports of ecthyma gangrenosum in apparently healthy, immunocompetent children (often with diaper-area involvement), but the diagnosis should prompt a thorough investigation for occult immunodeficiency. Neutropenia may be a risk factor for ecthyma gangrenosum. The characteristic lesions are hemorrhagic papules with a pink or violaceous rim ( Fig. 14-9 ) that progress to bullae, ulcers, and necrotic plaques. Eschar formation eventually occurs ( Fig. 14-10 ), and old lesions heal with scarring. The diagnosis can be confirmed by Gram stain and bacterial culture of lesions or blood cultures, which are positive for P. aeruginosa . Treatment with appropriate antipseudomonal therapy (i.e., aminoglycoside and an antipseudomonal penicillin) should be instituted early.


Folliculitis
The term folliculitis refers to an infection of hair follicles. The clinical appearance varies according to the location and depth of follicular involvement. Deeper follicular infections (furuncles and carbuncles) are discussed later. Superficial folliculitis (Bockhart impetigo), an infection of the follicular ostium, begins with superficial small, yellow-white pustules, often with a narrow red areola ( Fig. 14-11 ) and a hair shaft protruding from the center of the lesion. It occurs most commonly in children and usually is seen on the buttocks ( Fig. 14-12 ) and extremities, especially the thighs. Most lesions are painless, occur in crops, and heal over 7 to 10 days with postinflammatory hyperpigmentation. S. aureus is by far the most common pathogen; other possible etiologies include streptococci, Gram-negative organisms, and even dermatophytes. In immunocompromised children, commensal organisms may cause folliculitis, including Pityrosporum and Demodex (see Chapter 18 ). Superficial folliculitis is not always infectious in origin. “Sterile folliculitis” may be seen after skin contact with oil or other occlusive products and results in follicular plugging and inflammation. A classic example of sterile folliculitis is the scalp pustulosis occasionally associated with application of hair oils.


Superficial folliculitis usually responds to gentle cleansing with antibacterial soaps and the application of topical antibiotics such as clindamycin, erythromycin, or mupirocin. More extensive or resistant cases should be treated with a systemic antibiotic (a penicillinase-resistant penicillin or cephalosporin, depending on local resistance patterns). In such instances, bacterial culture should be obtained before the initiation of systemic therapy. Sodium hypochlorite (bleach) baths or washes on a twice to three-times weekly basis may be useful for individuals or families with recurrent folliculitis or furunculosis (see below). The recommended concentration for bleach baths is ![]() cup of bleach (around 5% to 6% sodium hypochlorite) dissolved in a full bathtub (around 40 gallons) of water, or approximately 1 mL/L (final concentration approximately 0.005%).
cup of bleach (around 5% to 6% sodium hypochlorite) dissolved in a full bathtub (around 40 gallons) of water, or approximately 1 mL/L (final concentration approximately 0.005%).
Folliculitis Barbae
Folliculitis barbae ( sycosis barbae ) is a term used to describe a deep-seated folliculitis of the beard area involving the entire depth of the follicle and perifollicular region ( Fig. 14-13 ). A pruritic papule is usually the initial lesion, with the process spreading from one follicle to another by trauma from scratching and/or shaving. The disorder is characterized by follicular papules and pustules and with progression, erythema, crusting, and boggy infiltration of the skin. Although occasionally other bacteria may be isolated, the etiology is usually S. aureus . The use of an electric rather than traditional razor or complete avoidance of shaving can sometimes be helpful in prevention and treatment of this condition. Warm compresses and topical antibiotics are often sufficient to control minor forms of sycosis barbae. If the condition is severe or recurrent, several weeks of systemic antibiotics may be necessary.

Pseudofolliculitis Barbae
Pseudofolliculitis barbae (PFB) (see Chapter 7 ) is a common, noninfectious inflammatory disorder of the pilosebaceous follicles of the beard that may be confused with sycosis barbae. PFB (commonly referred to as razor bumps ) is caused by shaved hairs that curve inward with resultant penetration of the skin followed by an inflammatory foreign body reaction. This form of folliculitis is seen particularly in African-Americans and individuals with curly hair. Mild cases may be managed by careful shaving and occasionally by changing from a traditional to an electric razor. Discontinuation of shaving is quite effective but not always acceptable to the patient. Close shaving, which promotes oblique penetration of hairs into the skin, should be avoided whenever possible. Other treatment options include chemical depilatory creams, topical retinoids or glycolic acid, topical steroids, benzoyl peroxide, and topical antibiotics. Epilation laser therapy (see Chapter 7 ) has also been demonstrated to be effective for the condition.
Pseudomonal Folliculitis (Hot-Tub Folliculitis)
Pseudomonal folliculitis is a form of folliculitis caused by P. aeruginosa that occurs after exposure to poorly chlorinated hot tubs, whirlpools, or swimming pools. It has also been reported in association with a contaminated water slide, a contaminated loofah sponge, swimming in a children’s pool filled with well water, and after shower/bath exposure. It is characterized by erythematous, follicular pustules and vesiculopustules that occur most often on the trunk, buttocks, and legs ( Fig. 14-14 ), especially in sites occluded by swimming garments. Lesions usually develop within 1 to 2 days after exposure. Mild constitutional symptoms may be present, including fever, malaise, headache, and arthralgias. More serious associations, including urinary tract infection and pneumonia, have also been reported. Lesions of hot-tub folliculitis generally subside spontaneously over 7 to 10 days. Antipseudomonal antibiotic therapy (i.e., with ciprofloxacin) may be necessary in severe cases. Preventive measures include maintenance of appropriate chlorination, frequent water changes, and thorough scrubbing of whirlpool baths and hot tubs with each water change. Importantly, 21% of 108 water and swab samples of hot tubs and indoor swimming pools were positive for P. aeruginosa in one study, and 96% of these isolates were multidrug resistant. The Centers for Disease Control and Prevention recommend maintaining the concentration of free chlorine in swimming pools to between 1 and 3 ppm and the pH at 7.2 to 7.8.

Hot hand–foot syndrome (also known as Pseudomonas hot foot syndrome ) presents with painful, erythematous palmoplantar nodules ( Fig. 14-15 ) after exposure to water containing a high concentration of P. aeruginosa and may be seen in conjunction with hot-tub folliculitis. When pustules are present, the organism can be easily cultured from skin swab material. An epidemic occurred in children exposed to the same community wading pool with a floor that was coated with abrasive grit and which, along with the inlets and a drain, yielded P. aeruginosa on culture. This disorder may be related to (or the same condition as) idiopathic palmoplantar hidradenitis of childhood (see Chapter 20 ). Similar palmoplantar inflammatory lesions have been reported in otherwise healthy children infected with Mycobacterium abscessus , also in association with exposure to public swimming pools (see Nontuberculous [“Atypical”] Mycobacterial Infection section).

Eosinophilic Pustular Folliculitis/Eosinophilic Folliculitis of Infancy
Eosinophilic pustular folliculitis (EPF; Ofuji disease) is a dermatosis of unknown cause characterized by erythematous patches with follicular papules and pustules, often in an annular or serpiginous arrangement, with occasional peripheral eosinophilia and leukocytosis. It was classically reported in Japanese individuals, although it may be seen in people of diverse ethnic backgrounds, and men appear to be affected more than women. Although this disorder is not bacterial in origin, it is included here because it is in the differential diagnosis of folliculitis. EPF may involve any surface area, including the face, trunk, and extremities. A form of EPF is recognized as an extremely pruritic dermatosis in adult patients with human immunodeficiency virus (HIV) infection, usually presenting late in the course of infection.
A distinct form of EPF occurs in otherwise healthy infants and toddlers and has been called eosinophilic folliculitis of infancy. It presents with recurrent crops of itchy follicular pustules of the scalp (most commonly; Fig. 14-16 ), trunk, and extremities with eventual spontaneous involution (see Chapter 2 ). The outbreaks occur in a cyclical fashion and may last from 3 months to 5 years, occasionally longer. Peripheral eosinophilia may be present. Whereas adults tend to have annular, serpiginous, or polycyclic lesions, the prominent scalp involvement and failure to form annular rings appear to distinguish the infantile form. Occasionally, eosinophilic folliculitis of infancy may be a presenting feature of the hyperimmunoglobulin-E (hyper-IgE) syndrome (see Chapter 3 ).

Treatment options for EPF include topical corticosteroids, oral erythromycin, dapsone, indomethacin, colchicine, topical tacrolimus, antihistamines, and ultraviolet B (UVB) phototherapy, which have each been used with variable success. The majority of patients respond to treatment with the former two agents; in one study of 51 patients treated with low- to medium-potency topical steroids, 46 (90%) responded well. The other treatments have been demonstrated successful but carry a greater risk of adverse effects.
Furuncles and Carbuncles
Furuncles (or “boils”) are painful, deep infections of the hair follicle in which purulent material extends into the dermis and subcutaneous tissues, forming perifollicular abscesses (see above). These lesions have a tendency toward central necrosis and suppuration. They are caused by S. aureus and are seen most often in older children and adults. They usually develop from a preceding folliculitis with deeper extension into the dermis and subcutaneous tissue. Chronic carriers of S. aureus are particularly predisposed, and familial spread of PVL-producing MSSA isolates has been observed and may be associated with greater numbers and more intensely erythematous lesions. Furuncles caused by CA-MRSA infection are increasing in incidence in the United States and are strongly related to production of the PVL virulence factor. Furuncles are most common in areas of skin that are hairy and subject to friction and maceration, particularly the back, axillae, thighs, buttocks, and perineum. They present as tender red nodules ( Fig. 14-17 ) that gradually become fluctuant and if untreated, may have a purulent blood-tinged discharge. There is a high rate of contagion in patients with furunculosis.

Carbuncles are larger, deep-seated staphylococcal abscesses composed of aggregates of interconnected furuncles that drain at multiple points on the cutaneous surface ( Fig. 14-18 ). They are usually seen in males on the posterior neck, back, thighs, and buttocks and extend into the deeper dermis and subcutaneous tissues, reaching a larger size than furuncles (up to 10 cm in diameter). They undergo necrosis and suppuration more slowly than furuncles and may present with severe pain and constitutional symptoms. Several factors predispose to the development of furuncles and carbuncles ( Box 14-2 ).

Diabetes mellitus
Obesity
Alcoholism
Scabies
Hematologic disorders
Immunodeficiencies, including hyper-IgE syndrome
Malnutrition
Chemotherapy
Corticosteroid therapy
Local skin trauma (abrasions, cuts, excoriations)
Debilitated state
The treatment of furuncles and carbuncles depends on the extent and location of lesions. The mainstay of therapy is systemic antistaphylococcal antibiotics with incision and drainage of fluctuant lesions. Cultures with sensitivity testing should be considered, especially in geographic areas with an increasing prevalence of staphylococcal resistance. Lesions caused by MRSA may respond (as discussed) to incision and drainage alone. Topical antibiotics (as discussed for impetigo and folliculitis) are not sufficient for the treatment of furuncles and carbuncles, given the depth of the process. The triple regimen of chlorhexidine skin disinfection (21 days), mupirocin applied to the nares (5 days), and oral clindamycin (21 days) was found to be very effective with a prolonged remission in nearly 90% of patients in an open-label study that included patients with both MSSA and MRSA furunculosis. Many practitioners recommend sodium hypochlorite baths or washes for patients with recurrent disease (see Folliculitis section). Lastly, attention to predisposing factors with appropriate treatment or modification (as feasible) is indicated.
Cellulitis
Cellulitis is an acute infection of the skin, particularly the subcutaneous tissues, characterized by erythema, swelling, and tenderness. The borders of cellulitis are not elevated or sharply defined, which helps to contrast it from the more superficial form called erysipelas (see Erysipelas section).
Cellulitis usually occurs after some form of skin trauma including puncture wounds, lacerations, dermatitis, burns, varicella, or dermatophyte infections. It presents with markedly red, tender, warm swelling of the skin with an infiltrated appearance ( Fig. 14-19 ), and the most common location is the lower extremities. Constitutional symptoms including malaise and fever are often present. The most common causes of cellulitis are S. aureus and GABHS, although occasionally other bacterial agents may be implicated. MRSA appears to be a rare cause of nonsuppurative cellulitis when extrapolated from staphylococcal patient-colonization data, although colonization may not be a primary risk factor in the pathogenesis of this infection. In young children, particularly those under 2 years of age, Haemophilus influenzae type b (Hib) was traditionally implicated in a facial cellulitis termed buccal cellulitis , although this form is now less common since licensure of the conjugated Hib vaccine. Buccal cellulitis characteristically reveals a dusky red to blue discoloration of the involved skin. Children with H. influenzae cellulitis may be quite toxic, with accompanying upper respiratory tract symptoms and bacteremia or septicemia. Streptococcus pneumoniae is another potential etiology of facial cellulitis in children, occurring especially in those under 36 months of age who are at risk for pneumococcal bacteremia. Because 96% of the serotypes (in one large series of S. pneumoniae facial cellulitis) are included in the heptavalent-conjugated pneumococcal vaccine now licensed in the United States, this cause of cellulitis will likely become significantly less relevant in years to come. Lastly, in children younger than 3 months of age, cellulitis is most commonly caused by group B streptococci (GBS) and is more likely to be associated with invasive disease, including bacteremia and meningitis. These children require blood, urine and cerebrospinal fluid (CSF) sampling and cultures as part of their initial evaluation.

Periorbital cellulitis is a unique form of cellulitis that deserves special mention here, given the potential confusion with orbital cellulitis and the associated complications. Periorbital (preseptal) cellulitis is a form of the disease that presents with erythema and swelling of the periorbital tissues. It may appear after skin trauma, in which case it is usually caused by S. aureus or GABHS infection or may result from cutaneous spread of pathogens from the paranasal sinuses or bloodstream, where it may result from Hib or S. pneumoniae infection. If the infection traverses the orbital septum (a continuation of the periosteum of the bony orbit to the margins of the upper and lower eyelids), it may result in orbital cellulitis, a more serious condition that may be complicated by abscess formation or cavernous sinus thrombosis. Patients with orbital cellulitis may experience proptosis, ophthalmoplegia, and decreased visual acuity in addition to the cutaneous findings. Computed tomography (CT) and ophthalmologic examinations are indicated if orbital cellulitis is suspected. The microbiology of periorbital and orbital cellulitis has also changed with the advent of Hib immunization, and Hib is now a very uncommon cause of these disorders, being supplanted by streptococcal species (including S. pneumoniae and GABHS) and S. aureus .
Treatment of cellulitis depends on the clinical presentation and knowledge (and identification, when possible) of the affecting organisms. The diagnosis of cellulitis is generally a clinical one, although fine-needle aspiration with Gram stain and bacterial culture may be helpful when unusual organisms are suspected (i.e., the immunocompromised host). Antibiotic therapy that covers for GABHS and S. aureus will be appropriate in most cases of routine, nonfacial cellulitis. In geographic areas with high rates of CA-MRSA, antibiotic selection should include coverage against this organism. There is no consensus on the choice between oral and intravenous antibiotics, although blood cultures, intravenous antibiotics, and hospitalization have traditionally been recommended for children at high risk for cellulitis. In recent years, short-course intravenous antibiotic therapy has been increasingly used in emergency department (ED) settings but may be associated with a higher failure rate and longer ED stay.
In children with facial or periorbital cellulitis, the possibility of S. pneumoniae and Hib infection should be considered in conjunction with the patient’s age and immunization status, and antibiotics should be chosen accordingly. Imaging (most often contrast-enhanced CT or diffusion-weighted magnetic resonance imaging [MRI]) is recommended in these patients to define the extent of involvement and help guide appropriate therapy. In infants younger than 3 months of age with cellulitis, GBS should be presumed as a potential etiologic agent, and in these infants, as well as the patient with periorbital or orbital cellulitis who is young, toxic, or shows signs of meningeal irritation, laboratory evaluation for sepsis and meningitis should be performed. Hospitalization with parenteral antibiotic therapy (and ophthalmologic consultation in those with orbital cellulitis) is indicated in these latter settings.
Erysipelas
Erysipelas is a superficial cellulitis of the skin with marked lymphatic involvement, resulting in most cases from GABHS. The organism usually gains access by direct inoculation through a break in the skin, but occasionally hematogenous infection may occur. The initial lesion begins as a small area of erythema that gradually enlarges to reveal a characteristic warm, painful, shiny, bright red infiltrated plaque with a distinct and well-marginated border. The face, scalp, and hands are the most common sites of involvement, although erysipelas may involve any skin surface. Penicillin, or a macrolide antibiotic in patients with penicillin allergy, is the drug of choice for therapy. In occasional patients, S. aureus may be a copathogen, in which case antimicrobial therapy directed against this organism is necessary.
Perianal Streptococcal Dermatitis
Perianal streptococcal dermatitis (PSD, also known as perianal dermatitis, perianal cellulitis, perianal streptococcal cellulitis, and streptococcal perianal disease ) is a well-defined entity that may be often overlooked. It presents as sharply circumscribed perianal erythema with occasional fissures, purulent discharge, and/or functional disturbances. GABHS is the etiology in most cases of PSD, although S. aureus and coliform bacteria have also been recovered. An epidemic outbreak in a daycare center has been reported. In a recent series of 26 patients with perianal dermatitis, S. aureus was the most common isolate and clinically was notable for concurrent papules and pustules of the buttocks and extension of the erythema to the adjacent buttock skin.
The skin findings in PSD are variable, from a dry pink appearance to bright red erythema ( Fig. 14-20 ) with a wet surface and occasionally the presence of a white pseudomembrane. The surface is often tender to touch, and associated symptoms include rectal itching or discomfort, painful defecation, blood-streaked stools, and constipation. In males, balanoposthitis or in females, vulvovaginitis may be present. Fever is notoriously rare in patients with PSD. Streptococcal pharyngitis may concomitantly be present in patients with PSD, but the exact associations between pharyngitis, PSD, and streptococcal colonization is unclear. There is some suggestion that specific GABHS isolates may have a tropism for perineal tissues, but the mechanism of infection is not yet clear. Guttate psoriasis (see Chapter 4 ), which is classically associated with streptococcal pharyngitis, may also be associated with PSD, and in any patient with new-onset guttate psoriasis, a thorough anogenital examination should be performed.


The differential diagnosis of PSD is broad and includes psoriasis, candidiasis, seborrheic dermatitis, cutaneous Crohn disease, pinworm infestation, and sexual abuse. The diagnosis can be confirmed by bacterial culture of a perianal swab, but when performing cultures to confirm the diagnosis of PSD, it is important to notify the laboratory of the microbe (GABHS) in question, because several labs utilize media selective for enteric pathogens with rectal swabs. Treatment with oral penicillin V, amoxicillin, a first-generation cephalosporin, or a macrolide or azalide (i.e., erythromycin, clarithromycin, or azithromycin) for patients allergic to penicillin is usually effective, with or without concomitant topical mupirocin. Some have suggested, however, that the risk of clinical recurrence is greater in patients treated initially with penicillin or amoxicillin. Oral cefuroxime was demonstrated more effective than penicillin in one study and is another reasonable option. If staphylococcal infection seems more probable clinically or is isolated in culture, the antibiotic regimen should be adjusted accordingly.
Blistering Dactylitis
Blistering dactylitis (also known as blistering distal dactylitis ) is a unique bullous manifestation of GABHS infection or only occasionally, other bacteria including S. aureus and GBS. It is rarely reported in association with MRSA infection. In its classic form, blistering dactylitis presents as a painful, tense, superficial blister on an erythematous base ( Fig. 14-21 ) most often located over the volar fat pad of the distal phalanx of a finger or several fingers. It is most common in children between the ages of 2 and 16 years, although it is also reported in adults, most notably immunocompromised ones. The blisters may occasionally extend to involve the dorsal surfaces of the fingers. Systemic manifestations including fever are rare. The differential diagnosis of blistering dactylitis includes bullous impetigo, herpetic whitlow, traumatic blistering, burns, and epidermolysis bullosa. Coexistent whitlow and blistering dactylitis have been reported. The diagnosis is confirmed by Gram stain and culture of blister fluid. If herpes infection is suspected, Tzanck smear, direct fluorescent antibody testing, or viral culture should be performed. Streptococcal blistering dactylitis is successfully treated with penicillin or erythromycin, but given recognition of the increasing role that staphylococci may play in the etiology, empiric antimicrobial therapy to cover for both organisms is recommended.

Necrotizing Fasciitis
Necrotizing fasciitis is a rapidly progressive, potentially fatal, necrotizing infection of the skin and subcutaneous tissues commonly associated with severe systemic toxicity. Over the years it has been known by several different names, including hospital gangrene , acute infective gangrene , streptococcal gangrene , gangrenous erysipelas , synergistic necrotizing cellulitis, and Meleney ulcer . A popular term in the lay media is flesh-eating bacteria disease . Although usually caused by GABHS, necrotizing fasciitis may be polymicrobial in nature and has been reported in association with other streptococci, P. aeruginosa , S. aureus , Klebsiella species, E. coli, Enterobacter cloacae , Serratia species, Proteus species, Enterococcus , a variety of anaerobic agents including Clostridium species and Bacteroides species, and even Vibrio species. CA-MRSA has been described as a potential monomicrobial cause of necrotizing fasciitis. The disorder is most common in individuals with decreased local resistance (skin trauma, surgery, varicella), malnutrition, or chronic disease. Necrotizing fasciitis is rare in children. In neonates, it has been observed in association with omphalitis, balanitis, mammitis, fetal scalp monitoring, and postoperative complications, with omphalitis being the most common.
Necrotizing fasciitis most commonly presents on an extremity and is characterized by pain, edema, and erythema with exquisite tenderness to palpation. These changes quickly progress through several sequential stages including ecchymosis, bullae, necrosis ( Fig. 14-22 ), gangrene, and with deep and extensive infection, overlying skin anesthesia. The inflammation extends deeply along fascial planes, highlighting the importance of rapid diagnosis and surgical exploration. Laboratory findings include leukocytosis, elevated serum creatine kinase level, hyponatremia, coagulopathy, and bacteremia. Fever, shock, and altered mental status typically develop within 48 hours. The most serious complication of necrotizing fasciitis is streptococcal toxic shock syndrome (TSS) (see below), which is characterized by hypotension, renal impairment, coagulopathy, liver abnormalities, respiratory distress, and a diffuse erythematous cutaneous eruption. Clinical clues that suggest necrotizing fasciitis over cellulitis include intense pain (often out of proportion to the clinical examination), rapid progression, bullae, necrosis, and lack of a rapid response to antibiotic therapy. Imaging studies may be useful in confirming the diagnosis, especially if soft-tissue gas is present, although this is not a consistent finding. MRI may be useful in distinguishing necrotizing fasciitis from uncomplicated infective fasciitis. Confirmation of infection can be accomplished with Gram stain and culture of blister fluid, lesion discharge or tissue, blood culture, and polymerase chain reaction (PCR) analysis for pyrogenic exotoxin B on tissue biopsy specimens.

Prompt thorough surgical debridement of necrotic tissue is of prime importance in the management of patients with this disorder, because without exploration and debridement, the mortality rate approaches 100%. Additionally, greater delays in time to initial surgical debridement are associated with increased mortality in children, as in adults with similar infections. Antimicrobial therapy should be initiated immediately, and the chosen agents should have activity against Gram-positive, Gram-negative, Clostridium , and anaerobic organisms. Clindamycin in particular seems to be quite effective as part of the antimicrobial regimen, given its ability to suppress both toxin and M protein synthesis. Antimicrobial therapy should be adjusted based on the results of Gram stain and bacterial cultures of the surgical specimen. In addition to these specific therapies, fluid resuscitation and blood pressure/blood product support are often indicated. The roles of hyperbaric oxygen therapy and intravenous immunoglobulin (IVIG) remain controversial, the latter being used primarily in the setting of GABHS infection with TSS.
Noma
Noma (cancrum oris, necrotizing ulcerative stomatitis) is a rare, progressive destructive infection usually involving the soft and hard tissues of the oral and paraoral structures. Most reported cases of noma are in children who are severely malnourished or chronically debilitated, and the disease tends to be most common in sub-Saharan Africa, South America, and Asia. The peak ages of incidence are between 1 and 4 years. The triad of malnutrition, poor oral hygiene, and periodontal disease contributes to the increased incidence in these locations. It is usually caused by anaerobic organisms, including Fusobacterium species, Prevotella intermedia , Actinomyces species, Peptostreptococcus micros , and Borrelia species and is characterized by a gangrenous, ulcerative infection of the gingivae, buccal mucosa, and eventually the cheeks and jaw.
The initial stage of noma is characterized by a painful, small purple-red lesion that becomes indurated and progresses to edema, necrosis, and ulceration. With expansion, underlying bone involvement occurs with resultant loss of dentition. Bony sequestrations of the mandible or maxilla may occur. Patients may also have fever, tachycardia, tachypnea, and anorexia, and their medical history may reveal recurrent fevers, diarrhea, and history or parasitic and/or viral infections. Treatment of noma includes antibiotics, wound care, and debridement with eventual surgical reconstruction. Without treatment, the mortality rate is 70% to 90%, and survivors suffer the long-term sequelae of orofacial mutilation and functional impairment. Rehydration, attention to electrolyte balance, and nutritional rehabilitation to correct protein and micronutrient deficiencies are other important aspects of therapy.
Noma neonatorum is a gangrenous process of the nose, eyelids, oral cavity, and anogenital region in low-birthweight infants and usually caused by P. aeruginosa . Most patients also have Pseudomonas sepsis, and the mortality rate without antimicrobial therapy is extremely high. Noma neonatorum, which is also more common in developing countries, was so named because of the clinical and histologic similarity to noma. However, there is significant overlap with the clinical presentation of ecthyma gangrenosum. Although some of the reported infants had immunodeficiency, it was either absent or not tested for in the majority of published cases. Noma neonatorum may represent a neonatal form of ecthyma gangrenosum.
Meningococcemia
Meningococcal infection, caused by the Gram-negative diplococcus Neisseria meningitidis , is a major world health problem in children under 5 years of age and is the leading cause of bacterial meningitis in children. Three serogroups of N. meningitidis , A, B, and C, account for more than 90% of cases of meningococcal disease, and along with groups Y and W-135 are implicated most commonly worldwide as causes of invasive disease. Person-to-person spread of N. meningitidis usually occurs through inhalation of droplets of infected nasopharyngeal secretions by direct or indirect oral contact. Meningococcal disease typically presents between 1 and 14 days after nasopharyngeal acquisition of N. meningitidis.
Acute meningococcemia may present in a variety of ways, from transient fever to fulminant disease. After an upper respiratory prodrome, patients develop high fever and severe headache. If meningitis develops, stiff neck, nausea, vomiting, and coma may be present. Up to two-thirds of patients develop a skin eruption, most classically a petechial rash of the skin and mucous membranes. Other cutaneous morphologies include macular, morbilliform, and urticarial eruptions, as well as a gray-colored acrocyanosis. The petechiae are usually small, stellate, and gray-purple with a raised border and slightly depressed, vesicular, or pustular center. The trunk and lower extremities (especially ankles and wrists) are common sites of predilection, whereas the palms, soles, and head tend to be spared. Mucosal surfaces including the palpebral and bulbar conjunctivae may be involved. More extensive hemorrhagic lesions are seen in fulminant meningococcal infections, and a progressive increase on all areas of the body may be followed by coalescence of lesions to form large purpuric patches with sharply marginated borders ( Fig. 14-23 ). These may progress to bullae, necrosis with sloughing, and eventual eschar formation. Autoamputation related to digital ischemic necrosis is a potential complication. Consumptive coagulopathy may be present and when occurring in the setting of progressive cutaneous hemorrhage and necrosis, is termed purpura fulminans. This finding is felt to portend a poor prognosis for the patient with meningococcemia. Three important clinical features that are suggestive of early acute meningococcal disease are leg pain, cold hands and feet, and abnormal skin color.

Chronic meningococcemia is a rare form of meningococcal infection that is unusual in children. It is characterized by intermittent episodes of skin lesions in conjunction with fever, joint pain, myalgia, and episcleritis. The cutaneous lesions seen in the majority of patients appear in crops coincident with or after the fever. Individual lesions are usually macular and occasionally purpuric or pustular. Because of potential confusion with other infectious or collagen vascular illnesses, a high index of suspicion is necessary. Patients with complement deficiencies, especially of the terminal complement system (C5-9), have an increased risk of both acute and chronic meningococcal infections.
The differential diagnosis of meningococcemia includes gonococcemia, Henoch–Schönlein purpura, rickettsial diseases, enteroviral infections, erythema multiforme, atypical measles, hypersensitivity vasculitis, and other bacterial septicemias or meningitides. The diagnosis is confirmed by culture of the blood and CSF. Isolation of meningococci from the nasopharynx is presumptive but not diagnostic, because asymptomatic carriage is not uncommon. Petechial lesions can be smeared and examined for the presence of Gram-negative diplococci and may be cultured for organisms. Serologic assays that can detect N. meningitidis capsular polysaccharide antigen in CSF, urine, serum, and other bodily fluids are also available. A serogroup-specific PCR test to detect N. meningitidis is used routinely in the United Kingdom and may be useful in patients who receive antimicrobial therapy before cultures have been obtained. The diagnosis of chronic meningococcemia is best confirmed by blood culture taken during a febrile episode, although several cultures may be necessary.
Meningococcal disease is treated with penicillin G, but at the time of presentation the initial choice of antimicrobials should be based on the clinical differential diagnosis and local antibiotic susceptibility patterns. Antibiotics with more expanded coverage such as cefotaxime or ceftriaxone are often used initially in patients with sepsis or meningitis until the diagnosis is confirmed. In patients with a history of anaphylaxis to penicillin, chloramphenicol is recommended. Supportive therapy with fluid, pressor, and blood product support as indicated is vital. Chemoprophylaxis of close contacts of patients with invasive meningococcal disease is recommended within 24 hours of diagnosis of the index case. Selective immunization is recommended for children 2 years of age and older in high-risk groups (asplenia, terminal complement deficiencies, or travel to endemic or epidemic areas). Routine immunization with the licensed quadrivalent vaccine is recommended for adolescents at the 11- to 12-year visit and at high school entry or 15 years of age (whichever comes first), as well as students entering college who plan to live in dormitories and military recruits. However, routine childhood immunization is not recommended because of the low incidence of disease, the poor response in young children, the short-lived immunity, and the potential impaired response to subsequent vaccine doses in some serogroups.
Gonococcemia
Gonococcemia is associated with cutaneous lesions similar to those of meningococcemia and presents with fever, chills, arthralgia, and myalgia in patients with gonococcal septicemia. Symptoms of sexually transmitted gonococcal infection may or may not be present, including vaginitis, pelvic inflammatory disease, urethritis, proctitis, or pharyngitis. Hematogenous spread of Neisseria gonorrhoeae occurs in up to 3% of untreated persons with mucosal gonorrhea. Skin lesions develop within 3 to 21 days of contact, are located primarily over joints of the distal extremities, and usually appear as petechiae, small erythematous or hemorrhagic papules, or vesiculopustules ( Fig. 14-24 ). They usually heal spontaneously in 4 to 6 days.

The causative agent, N. gonorrhoeae , is a Gram-negative diplococcus and may be demonstrated by smear, culture, or immunofluorescence studies of skin lesions or by culture of the blood, anogenital tract, pharynx, or joint fluid on Thayer–Martin medium (chocolate agar with the addition of antibiotics to inhibit normal flora and nonpathogenic neisserial organisms). Nucleic acid amplification studies (i.e., PCR) are also available and have a high sensitivity and specificity when performed on urethral or cervicovaginal swabs.
The treatment of choice for gonococcemia is parenteral ceftriaxone or cefotaxime. Alternatives for individuals with β-lactam allergy include ciprofloxacin, ofloxacin, or spectinomycin. If concomitant infection with Chlamydia trachomatis is suspected, initial therapy should also include erythromycin, doxycycline, or azithromycin.
Staphylococcal Scalded Skin Syndrome
SSSS is a term used to describe a blistering skin disease caused by the epidermolytic (or exfoliative) toxin (ET)-producing S. aureus . It was previously known as Ritter disease or pemphigus neonatorum and tends to occur most often in neonates and young children. Its severity may range from mild, localized blistering to widespread exfoliation. Mild cases are probably more common yet less often reported.
The pathogenesis of SSSS relates to the production of ETs, of which there are two serotypes affecting humans, ETA and ETB. These toxins have high sequence homology and are both capable of cleaving the epidermis at the superficial level of the stratum granulosum. The pathogenic mechanisms of ETA and ETB have been clearly elucidated, and they have been shown to target desmoglein 1, a cell–cell adhesion molecule found in desmosomes of the superficial epidermis. Desmoglein 1 is the same molecule targeted in the autoimmune blistering disease, pemphigus foliaceus (PF) (see Chapter 13 ). Once it was determined that antibodies against desmoglein 1 cause PF, astute researchers hypothesized and eventually proved that the target of the staphylococcal exfoliative toxin was also desmoglein 1. There are two main theories for the observation that SSSS preferentially affects neonates and children: lack of protection from antitoxin antibodies and decreased renal excretion of the toxin. In adults, SSSS is quite rare and usually occurs in the setting of immunosuppression, malignancy, heart disease, or diabetes.
Outbreaks of SSSS have been reported in neonatal intensive care units and well-baby nurseries. In these settings, asymptomatic or clinically infected healthcare workers often act as carriers of the epidemic strain of S. aureus , and given the potential severity of infection in the premature infant, prompt recognition with institution of strict infection-control strategies is vital to prevent further nosocomial spread. In a series of 39 neonates with SSSS, pneumonia was the most common complication, followed by myocarditis.
SSSS generally begins with localized infection of the conjunctivae, nares, perioral region, perineum, or umbilicus. Separation of perioral crusts often leaves behind radial fissures around the mouth, resulting in the characteristic facial appearance of SSSS ( Figs. 14-25 and 14-26 ). Other infections that may serve as the initial nidus for SSSS include pneumonia, septic arthritis, endocarditis, or pyomyositis. Fever, malaise, lethargy, irritability, and poor feeding subsequently develop, and the generalized eruption begins. The rash is characterized by erythema that progresses to large, superficial fragile blisters that rupture easily, leaving behind denuded, desquamating, erythematous, and tender skin (see Fig. 14-26 ; Fig. 14-27 ). The eruption is most marked in flexural creases but may involve the entire surface area of skin. The Nikolsky sign (progression of the blister cleavage plane induced by gentle pressure on the edge of the bulla) is positive. With extensive denudation of skin, patients may have decreased thermoregulatory ability, extensive fluid losses, and electrolyte imbalance and are at serious risk for secondary infection and sepsis. With appropriate management the skin heals without scarring, given the superficial cleavage plane of the blisters.




SSSS is usually diagnosed based on the clinical presentation. The main differential diagnosis is toxic epidermal necrolysis (TEN), a severe exfoliative condition that is usually drug-induced and has a high mortality rate. The most helpful distinguishing feature of TEN is mucosal involvement, including of the mouth, conjunctivae, trachea, and genital mucosa, which is lacking in SSSS. Other less common differential diagnoses include scalding burns, epidermolysis bullosa, graft-versus-host disease, nutritional deficiency dermatosis, and bullous ichthyosis (in the neonate). The diagnosis of SSSS is confirmed by isolation of S. aureus . It must be remembered that the majority of blisters in SSSS are sterile, because they are caused by the hematogenous dissemination of the bacterial toxin and not the bacteria itself. The organism is most easily recovered from pyogenic (not exfoliative) foci on the skin, conjunctivae, nares, or nasopharynx. When the diagnosis remains in question, differentiation from TEN can be made by microscopic examination of a skin snip of the blister roof or a skin biopsy. In SSSS, cleavage occurs in the superficial epidermis at the level of the granular layer, whereas in TEN the split occurs below the dermal–epidermal junction.
Treatment of SSSS is directed at the eradication of toxin-producing staphylococci, thus terminating toxin production. A penicillinase-resistant penicillin, first- or second-generation cephalosporin, or clindamycin are all appropriate initial choices, with modification based on sensitivity testing. In patients with MRSA infection, parenteral vancomycin or other agents (as dictated by local resistance patterns) would be indicated. Because SSSS is usually a more mild disease in older children, ambulatory therapy may be an option in this population. In neonates or in infants or children with severe infection, hospitalization is mandatory, with attention to fluid and electrolyte management, infection control measures, pain management, and meticulous wound care with contact isolation. In particularly severe disease, care in an intensive care or burn unit is required. Neutralizing antibodies that inhibit the binding of ETs to desmoglein 1 are under investigation, given concerns about the development of antibiotic-resistant, exfoliative-toxin-producing staphylococci.
Toxic Shock Syndrome
TSS is an acute febrile illness characterized by fever, rash, hypotension, and multisystem organ involvement. Although classically described in menstruating women in relation to the use of superabsorbent tampons, TSS is now recognized in both menstrual and nonmenstrual forms, the latter now being more common. Nonmenstrual TSS may occur in association with surgical procedures, nasal packing, the postpartum state, and a variety of S. aureus infections.
TSS is caused by toxin-producing strains of S. aureus . Manifestations of the disease are mediated primarily by the TSS toxin (TSST-1) and staphylococcal enterotoxins (SEA, SEB, SEC). These toxins are capable of widespread polyclonal activation of T cells, which results in massive cytokine release and in the clinical picture of TSS. Both TSST-1 and the SEs are considered “superantigens,” given their ability to activate T cells without intracellular processing and via specific binding to major histocompatibility complex (MHC) class II molecules. MRSA appears to account for a small percentage of TSS cases.
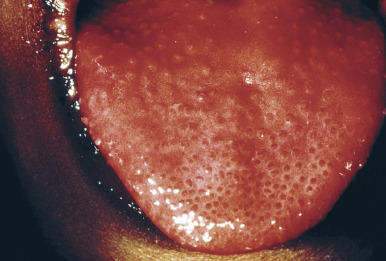
A prodrome of mild constitutional symptoms including malaise, myalgias, and chills often precedes the symptoms of TSS. Eventually fever develops along with lethargy, diarrhea, chills, nausea, and altered mental status. Symptoms of hypovolemia including hyperventilation, palpitations, and orthostatic dizziness may be present. Physical findings include high fever, hypotension, a diffuse rash, and pharyngitis with hyperemia of mucous membranes. The cutaneous eruption is a diffuse, macular erythroderma that is occasionally reminiscent of the rash of scarlet fever. Accentuation of the eruption in skin folds is a common finding, and in rare cases the inguinal or perineal regions may be the only skin surfaces involved. Edema of the hands, feet, and face may be present, and desquamation of the affected skin surfaces ( Fig. 14-28 ) eventually ensues. The nails may be shed, and telogen effluvium may occur up to several months later. Oral examination often reveals a strawberry tongue ( Fig. 14-29 ), and palatal petechiae may be present. Diffuse myalgia is almost always present, and many patients complain of exquisite skin or muscle tenderness when they are touched or moved.


In addition to the fever, desquamating rash, and hypotension, evidence of multiorgan involvement is present. To meet the case definition of TSS, three or more of seven other organ systems must be involved ( Box 14-3 ). The diagnosis of TSS generally rests on clinical criteria, although isolation of S. aureus from a normally sterile site, especially if toxin production can be demonstrated, is supportive. Histopathologic findings on skin biopsy are not pathognomonic. The differential diagnosis of TSS includes streptococcal TSS (see below), Kawasaki disease, scarlet fever, drug reaction, atypical measles, Rocky Mountain spotted fever, and other exanthematous illnesses. The presence of shock and multiorgan involvement is unusual in the other entities, except for streptococcal TSS, which usually has some distinguishing features.
- ▪
Temperature >38.9° C (102° F)
- ▪
Diffuse macular erythroderma
- ▪
Desquamation, 1 to 2 weeks after onset, particularly of the palms and soles
- ▪
Hypotension
- ▪
Multisystem involvement (3 or more of the following):
- ▪
Gastrointestinal (vomiting, diarrhea)
- ▪
Muscular (severe myalgia, increased creatine phosphokinase level)
- ▪
Mucous membrane (vaginal, oropharyngeal, or conjunctival) hyperemia
- ▪
Renal (elevated serum urea nitrogen or serum creatinine level more than twice the upper limit of normal, or urinary sediment with >5 WBC per field in absence of UTI)
- ▪
Hepatic (total bilirubin, AST or ALT greater than twice the upper limit of normal)
- ▪
Hematologic (platelet count ≤100,000/mm 3 )
- ▪
Central nervous system (disorientation, altered consciousness without focal neurologic signs when fever and hypotension are absent)
Laboratory criteria: negative results on the following tests (if obtained):
- ▪
Blood, throat, or CSF cultures (except blood culture may be + for S. aureus )
- ▪
Serologic tests for Rocky Mountain spotted fever, leptospirosis, or measles
- ▪
Probable disease: meets laboratory criteria and 4 of the 5 bulleted (dark green) findings are present
Confirmed disease: meets laboratory criteria and all 5 of the bulleted (dark green) findings, including desquamation (unless patient expires before desquamation occurs)
ALT, Alanine aminotransferase; AST, aspartate aminotransferase; CSF, cerebrospinal fluid; UTI, urinary tract infection; WBC, white blood cell.
A neonatal TSS-like disease has been reported, and in some of these patients MRSA was recovered. When studied, several of these MRSA isolates were positive for TSST-1 production. Most of the reported neonates had a mild course with a fairly rapid recovery.
Since the late 1980s a disease similar to TSS yet with some distinguishing features has been recognized. This disorder is associated with toxin-producing GABHS and is referred to as streptococcal TSS . Although the pathogenic mechanisms are not entirely clear, streptococcal pyrogenic exotoxins (SPEA, SPEB, SPEC), mitogenic factor, and streptococcal superantigen appear to be associated with the clinical findings.
Streptococcal TSS is similarly characterized by the acute onset of shock and multisystem organ failure, but unlike staphylococcal TSS, patients usually have a focal, invasive tissue or blood infection with GABHS ( Box 14-4 ). Most patients with streptococcal TSS have pain localized to an extremity in association with necrotizing fasciitis or myonecrosis. This pain is usually out of proportion to the clinical findings on physical examination. Varicella is a particularly important risk factor for invasive GABHS infections in children, and in the child with varicella who becomes febrile after having been afebrile or who has any fever beyond the fourth day of illness, GABHS infection should be considered.
Isolation of GABHS:
- ▪
From a normally sterile site (i.e., blood, CSF, peritoneal fluid, tissue biopsy) *
* Definite case: from a normally sterile site and both bulleted (dark green) findings.
OR
- ▪
From a nonsterile site (i.e., throat, sputum, vagina) †
† Probable case: from a nonsterile site and both bulleted (dark green) findings.
AND
- ▪
- ▪
Hypotension or shock
AND
- ▪
At least 2 of the following:
- ▪
Renal impairment (creatinine >2 mg/dL or >twice the upper limit for age)
- ▪
Coagulopathy (DIC or thrombocytopenia)
- ▪
Hepatic involvement (AST, ALT, or total bilirubin >twice the upper limit for age)
- ▪
Adult respiratory distress syndrome
- ▪
Generalized erythematous rash with or without desquamation
- ▪
Soft-tissue necrosis (i.e., necrotizing fasciitis or myositis or gangrene)
- ▪
ALT, Alanine aminotransferase; AST, aspartate aminotransferase; CSF, cerebrospinal fluid; DIC, disseminated intravascular coagulopathy; GABHS, group A β-hemolytic streptococcus.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


