Synopsis
- ■
Reconstruction of the soft tissues of the back at first may seem to be a daunting task compounded by large wounds, unfamiliar and segmental anatomy, radiation, hardware, and difficulties with postoperative positioning.
- ■
Many of the conditions treated require significant coordination with surgical colleagues.
- ■
Many of the conditions are unfamiliar to the plastic surgeon and without parallel conditions elsewhere in the body, an example being pseudomeningoceles filled with cerebrospinal fluid (CSF).
- ■
The goal of this chapter is to provide the reader with real-life solutions to difficult problems involving back wounds.
Keywords
Back, Trunk, Lumbar, Thoracic
Synopsis
- ■
Reconstruction of the soft tissues of the back at first may seem to be a daunting task compounded by large wounds, unfamiliar and segmental anatomy, radiation, hardware, and difficulties with postoperative positioning.
- ■
Many of the conditions treated require significant coordination with surgical colleagues.
- ■
Many of the conditions are unfamiliar to the plastic surgeon and without parallel conditions elsewhere in the body, an example being pseudomeningoceles filled with cerebrospinal fluid (CSF).
- ■
The goal of this chapter is to provide the reader with real-life solutions to difficult problems involving back wounds.
Brief introduction
- ■
The back is 18% of the total body surface area, yet it is an area commonly neglected in older texts of plastic surgery. However, with advancements in spine instrumentation and surgery and subsequent wound-related complications, surgical procedures to close the back reliably have been developed.
- ■
Spine teams have noted the efficacy of muscle flap closure of open spine wounds, and this has led to the introduction of prophylactic use of muscle flaps at the time of spine surgery. The same algorithms described in the chapter below are used, but now at the time of the back procedure, rather than only when there is a complication.
- ■
It is difficult, if not impossible, to define exactly who should need a prophylactic soft tissue reconstruction of the back.
- •
Patients with previous hardware infections, a woody feel to the soft tissues at the time of surgery, prior back surgery, long reconstructions greater than six vertebral bodies, cerebrospinal fluid (CSF) leaks, and a radiation history to the area all seem to be appropriate candidates to receive a soft tissue reconstruction.
- •
In our center, we limit prophylactic closures to patients with prior infections, when the muscles will not close in the midline due to tissue loss or prior surgery, a history of radiation with a woody feel to the tissues, and CSF leaks.
- •
- ■
Chronic hardware exposures, those which occur 6 months after placement, act differently from acute exposures. From experience, long-term coverage of chronically exposed hardware is not successful.
- ■
When patients present with small areas of drainage, and by palpation, a piece of hardware can be reached, this defines a hardware infection. Similarly, patients with fluid collections or “fluid cysts” in association with hardware have chronic infections.
- ■
These infections can be present for months or years and yet not suppurate, nor make the patient overly ill, and are undoubtedly due to the low virulence of the organism, such as Staphylococcus epidermidis .
- ■
Debridement, irrigation, and soft tissue coverage of these chronic exposures may be initially successful, but eventually fail. Thus, for most patients, the involved hardware should be removed.
- ■
The question is whether all of the hardware needs to be removed or if just a local portion (such as a large bolt) should be removed and the soft tissues closed. These are decisions made in the operating room.
- •
All hardware in association with exudative fluid should be removed.
- •
Well-incorporated hardware encased in bone can be allowed to remain.
- •
No flaps are typically required for closure when all of the hardware is removed.
- •
Patient outcomes depend more on the structural stability of the spine than on any soft tissue work.
- •
The soft tissues are simply approximated over drains, and complete healing is the rule rather than the exception. Antibiotics are not needed for prolonged periods in these situations.
- •
Preoperative considerations
Midline back wounds
- ■
When a spine surgeon calls to discuss new drainage from a midline spine wound, the thought process for treatment should be methodical and thorough. A review of operative details and thorough history and physical examination are critical.
- ■
A complete history should include operative details, the presence, visibility, and/or palpability of hardware, any history of postoperative complications and/or dural injury with associated CSF leak, and a review of imaging demonstrating hardware position relative to areas of wounds or drainage.
- ■
An evaluation of patient co-morbidities and potential wound healing issues is also necessary, including a history of malnourishment, diabetes, obesity, dead space management problems, and/or prior radiation.
- ■
A thorough examination should note wound characteristics, including the presence of persistent drainage and dieback of wound edges commonly seen with deep fluid collections and new pressure points as a result of new postoperative spinal alignment.
- ■
The time course of the presentation is critical.
- ■
Early postoperative episodes of drainage less than 4–6 weeks after the spine surgery are typically successfully treated with repeat surgery and soft tissue reconstruction with hardware preservation.
- ■
However, drainage that has been only partially treated with a small debridement or treated solely with intravenous antibiotics, only to resurface months later, is more difficult to treat.
- ■
A chronic hardware infection, defined as bacteria in association with hardware greater than 6 months after placement, is typically not a situation that plastic surgery can definitively treat without hardware removal.
- ■
Much can be learned with the simple examination of a patient’s chest X-ray in terms of the existence and location of hardware. Otherwise, plain films of the spine are obtained to reveal the length of the construct when present, degenerative spine disease, and the presence or absence of fusion.
- ■
CT scans and MRI are helpful to look for fluid collections, pseudomeningoceles, and inflammation of the soft tissues.
- ■
A key issue is if fluid collections are above or below the standard back muscle closure. If fluid or hematoma is seen deep to the musculature, a deep hardware infection is more likely.
Non-midline back wounds
- ■
While midline wounds are either due to pressure sores or spine procedures, non-midline wounds represent a much more heterogeneous collection of etiologies and therefore require a wide range of solutions.
- ■
Much like acquired wounds elsewhere in the body, wounds of the non-midline back are due to poor wound healing after access incisions of the chest cavity or retroperitoneum, necrotizing infections, or after tumor excision.
- ■
For these patients, a more standard thought process often suffices in the absence of hardware, deep wounds, and CSF leaks.
- ■
The wounds are typically flat and often allow skin grafting.
- ■
When flaps are needed to cover bone or prosthetic material, the muscles that are used to cover the midline spine are often available and even easier to mobilize to the lateral back due to the lateral placement of their pedicles.
- ■
The lateral tissues, being more mobile than the midline tissues, are easier to transpose for adjacent tissue transfers.
- ■
Free flaps are facilitated by having larger inflow vessels available, such as the axillary artery, than exist for midline reconstructions.
Technical pearls
Flap selection by region
Cervical region
- ■
The cervical spine area is more often instrumented from the anterior than the posterior approach.
- ■
Wounds of the anterior cervical spine are uncommon, and, when they occur, can be in association with esophageal injuries. Wounds of the posterior cervical spine are more common.
- ■
Soft tissue defects without spine involvement are treated depending on the size and location of the defect either with skin grafts or adjacent tissue transfers. Pressure sores tend to be treated conservatively with pressure relief. Laminectomies are performed for spinal cord pressure from metastases, and the wound beds are typically radiated.
- ■
Trapezius pedicled flaps are the preferred treatment for patients who have received radiation following laminectomy and oncologic tumor resection.
Thoracic region
- ■
Soft tissue defects without spine involvement are treated depending on the size and location of the defect either with skin grafts or adjacent tissue transfers.
- ■
The scapular and parascapular flaps can be helpful in closing some of these soft tissue defects without spine involvement, and the donor site should be oriented perpendicular to the long axis of the wound to facilitate closure.
- ■
Latissimus flaps based on the paraspinous perforators are ideal in radiated wounds to allow the muscle to be “dropped in” these defects, and thereby not manipulate the radiated and stiff erector spinae muscles. Myocutaneous latissimus flaps have easier insets, with the overlying skin paddle sewn to the adjacent midline back skin.
- ■
Wounds of the thoracic back after spine surgery and placement of hardware are best treated with erector spinae flaps. There is no need for a “double muscle” closure with further mobilization of a latissimus flap if the erector spinae muscles come together normally.
- ■
Rarely, in extremely deep wounds, the pedicled omental flap is ideal to fill the defect and to help achieve closure. These unusual circumstances often also require either erector spinae flaps or latissimus flaps to aid in the closure.
Lumbar region
- ■
The high lumbar area is the optimal area for reclosure with erector spinae flaps. The muscles are largest in this area and exist in a lordotic area of the back that is protected from pressure.
- ■
Other flaps are also possible for the lumbar area and include turnover latissimus flaps, which can reach this area, but only with some difficulty. Sliding of myocutaneous latissimus flaps elevated from the lower lumbar area and transposed medially provides thick coverage of the spine, but only at the expense of a skin-grafted donor site. The omentum will also reach this area with some ease.
- ■
The inferior region of the lumbar spine is best covered with superior gluteal artery–based flaps.
- ■
Often, a gluteal flap will be combined with erector spinae flaps for coverage of a longer lumbar and lumbosacral defect.
Lumbosacral region
- ■
The recess between the sacrum and the inferior aspect of the spine is best filled with a superior gluteal artery–based flap, as the erector spinae muscles are thin and laterally displaced in this area, precluding their use.
- ■
Omental flaps are possible but require position changes in the operating room and bowel dissection. Random-pattern skin flaps of the lumbar tissue or perforator-based flaps are also possible, but are difficult to inset and control in an area that is subjected to high shear forces with position changes. Finally, while latissimus flaps can be mobilized to reach this area, there are many wounds that are simply too big to have the latissimus muscle both reach and fill the entire cavity.
- ■
Patients undergoing a full sacrectomy for tumor can undergo bilateral gluteus myocutaneous flaps if the superior and/or inferior gluteal arteries are preserved during the sacrectomy. Closure of the gluteus muscles in the midline, like a pressure sore, can be done with V-Y advancement of the skin paddles if necessary.
- ■
For low rectal tumors with invasion into the sacrum, a transabdominal flap using a flap based on the inferior epigastric artery is also feasible.
- •
The oblique rectus abdominis musculocutaneous flap, using a skin paddle based in an oblique direction off the periumbilical perforators and using only the lower aspect of the rectus muscle, can easily bring non-radiated skin to the lumbosacral area.
- •
The vertical rectus abdominis musculocutaneous flap is another common design to achieve wound closure, but requires the harvest of more muscle.
- •
These abdominal flaps need to be parked adjacent to the sacrum and the abdomen closed. After sacrectomy, the flap can be retrieved from the posterior approach into the abdomen.
- •
- ■
For the majority of patients with lumbosacral defects, the tissue near the trochanter can be elevated with the blood vessels in continuity with the superior gluteal artery for soft tissue coverage ( Fig. 15.1 ) .
- •
This can be done as a pure perforator flap, or else with a strip of gluteus muscle under the skin paddle (which is de-epithelialized).
- •
As the flap is typically flipped 180°, the skin paddle will rest over the dura. To re-emphasize, this is a different design than for superior gluteal artery perforator flaps done for sacral pressure sores.


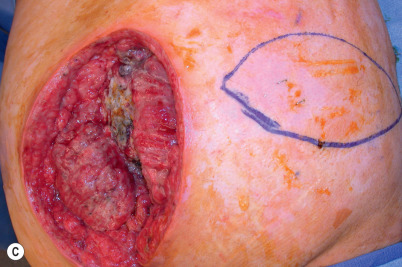

Figure 15.1
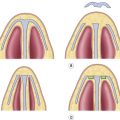
(A) Large Marjolin ulcer found in a chronic pilonidal cyst in an ambulatory patient. (B) Tumor excision. (C) A superior gluteal artery perforator flap is drawn out. The long axis of the skin paddle is perpendicular to the long axis of the defect to facilitate closure. The tumor excision and the final closure were staged to allow for definitive pathologic clearance of the margins. (D) Flap inset into defect.
- •
Wounds of the lateral back
- ■
Soft tissue reconstruction of the lateral back has certain special characteristics.
- ■
In the thoracic area, if the rib cage is intact, then most wounds would be closeable with local wound care, latissimus flaps, parascapular/scapular flaps, serratus flaps, or posterior movement of a perforator flap from tissues in the anterior axillary line area.
- ■
If the ribs are involved, then a decision about possible reconstitution of the pleural line needs to be made. Most authorities recommend that three or more ribs be reconstructed with a prosthetic patch, and this patch would then need to be covered with soft tissues. However, when the rib defect is located under the scapula, then the scapula serves to protect and camouflage any defect, and so, larger rib resections are tolerated.
- ■
The lateral lumbar area in adults typically is protected by its lordotic shape, and the only structure that needs to be reconstructed is the posterior aspect of the abdominal wall. All other wounds can be closed with local wound care, skin grafts, or transfer of the latissimus muscle.
Operative techniques
Local wound care
- ■
For superficial, relatively painless wounds without exposed hardware, local wound care with dressings is a relatively risk-free way to achieve wound closure.
- ■
Draining midline incisions tend to have wide areas of undermining along the length of the closure. These tunnels can typically be opened in the office with local injection of anesthesia and finger fracturing of the incision.
- ■
A long wound without tunnels with a saucer shape typically heals faster than small wounds with a fishbowl-shaped internal wound; therefore, tunnels should be opened along old incision lines.
- ■
All necrotic tissue should be debrided. All non-absorbable sutures, such as braided polyester, should be removed.
- ■
Patients are often unaware of the real size of the wound and must be prepared for the resulting appearance of the surgical site after opening of tunnels.
- ■
Dressings can be simple wet-to-wet saline dressings, with twice-a-day showers to cleanse the surface of the wound. Subatmospheric-pressure dressings can be employed, but the tubing is sometimes difficult to place under back-bracing devices.
- ■
After a wound has granulated, or if it is painful, then delayed primary closure or skin grafts can be performed if the wound is sizeable.
Operative debridement
- ■
Patients with persistently draining wounds after spine surgery associated with hardware should be evaluated critically for an operating room debridement.
- ■
Secondary indications for a debridement include unexplained fevers and fluid collections seen on imaging scans.
- ■
The maneuvers in the operating room are a critical step in the treatment of patients with postsurgical back wounds.
- ■
A thorough incision and drainage should be performed for patients with unexplained or purulent drainage through their incision.
- ■
The entire length of the incision should be opened as widely as necessary to explore for purulence and drain fluid collections.
- ■
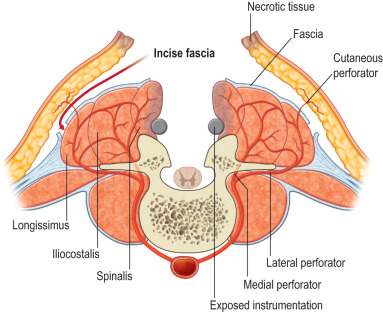
The erector spinae muscle closure should be reopened for cultures and to evaluate for liquefying hematomas.
- ■
The surgeon should be knowledgeable at the beginning of the debridement if a laminectomy had been performed at the original spine surgery in order to prevent injury to the spinal cord and dura during the incision and drainage.
- ■
After adequate exposure, the surgeon will need to make a decision as to the quality of the tissues.
- ■
Non-purulent benign fluid collections in the subcutaneous tissues with no purulence deep to the musculature can be reclosed over drains or else closed secondarily with a subatmospheric-pressure dressing.
- ■
Purulent and deep collections require additional decisions.
- ■
If the local wound is so purulent as to preclude an immediate reclosure, then all non-viable tissue should be debrided, the wound irrigated and left open for local wound care.
- ■
Alternatively, a subatmospheric-pressure dressing may be applied, but this often involves a return trip to the operating room for its next exchange.
- ■
For those deep wounds judged amenable to reclosure, a radical incision and drainage are performed. This should involve the surgical excision of scarred tissues where possible to reveal supple soft tissues with pulsatile bleeding.
- ■
Pulsatile bleeding at wound margins has been shown to correlate with wound healing in problematic incisions, such as distal foot amputations.
- ■
Tissues with a pseudobursa should be excised, as this, too, represents scar. Tissue that is stiff is unyielding and does not conform well, and so the tissues should be removed until they are soft to palpation.
- ■
An interesting issue is the removal of non-viable elements such as hardware and bone graft.
- ■
Hardware that is well fixed should remain in place in early hardware infections. This is done both to stabilize the wound for improved healing as well as to avoid the surgery involved with removal and later replacement of hardware.
- ■
Long-term maintenance of the hardware as well as clinical and radiographic evidence of fusion are well documented in patients who were returned to the operating room for washouts within 6–8 weeks of placement.
- ■
In the absence of definitive studies, it seems reasonable to remove non-incorporated and easy-to-remove graft, but to leave in place graft that has, in any way, begun to stick to the local tissues due to inosculation.
- ■
In the treatment of wounds of the spine, the three-dimensional shape should be evaluated and converted as much as possible to a two-dimensional wound.
- ■
Prominent hardware should be exchanged for something with a lower profile.
- ■
Patients with incomplete corrections of the spine deformities should be revised to recreate better the natural contours.
- ■
The deeper the hole, the more a flap should be “dropped into” the defect, rather than tissue simply slid towards the midline. This requires a more redundant soft tissue flap, such as an omentum, to fill the defect appropriately.
Flap closure
Principles
- ■
The first step in reconstruction is a timely debridement.
- ■
The second step is local wound control with a radical debridement of all stiff and scarred tissue.
- ■
Finally, the reconstruction should be performed to do the “maximum for the minimum.”
- ■
The procedure with the highest chance for success and with the lowest morbidity should be selected for the patient.
- ■
Central questions to be answered include the presence or absence of a fusion and the vertebral levels involved.
- ■
When an instrumented fusion has been performed, then the erector spinae musculature function is no longer necessary, and the muscles are completely expendable in terms of a reconstruction. The fusion rods prevent postoperative motion, and so, when the erector spinae muscles are reapproximated in the midline, they tend to stay there.
- ■
Spine patients without fusions still require the function of the erector spinae musculature when healing is completed for flexion and extension of the spine. These patients do better with flaps that are “dropped into the hole”, rather than with erector spinae muscles that are closed side to side and that would dehisce with back flexion.
- ■
Local wound care often suffices for superficial wound problems above the erector spinae.
Possible flap choices for spine closure
Erector spinae muscle flaps
- ■
The erector spinae muscles, also called the paraspinous muscles, are expendable after a previous spine fusion and no longer are functional for spine extension and flexion.
- ■
This flap is appropriate from the high cervical area to the low lumbar area, but it will not adequately cover an occipitospinal fusion, nor will it be sufficient for lumbosacral soft tissue coverage.
- ■
One must be careful in its use when a lateral approach to the spine has been made, because the muscle can be transected for access.
- ■
First, skin flaps are elevated superficial to the thoracolumbar fascia ( Fig. 15.2 ) .