The bony orbit is commonly involved in athletic injuries. Evaluation should include a comprehensive history and ocular examination. Computed tomography imaging is the gold standard for diagnostic testing. Urgent surgical intervention for orbital floor fractures should occur after “white eye” trapdoor fractures or if oculocardiac response occurs. Most orbital fractures do not require urgent intervention and repair can be completed within 2 weeks of injury. There are many approaches to repair orbital fractures, and consideration of techniques depends on the unique fracture pattern. Intraoperative computed tomography has become frequently used and can lead to increased identification of plate malpositioning intraoperatively.
Key points
- •
Athletic injuries can frequently involve the bony orbit. Evaluation should include a comprehensive history and ocular examination. Computed tomography imaging is the gold standard for diagnostic testing.
- •
Orbital fractures can occur in isolation or as combined fractures with multiple orbital walls and/or zygomaticomaxillary complex fractures. Depending on the fracture pattern, considerations for vision and intracranial complications must be considered.
- •
Management of orbital floor fractures can be broken down into 3 main treatment pathways: urgent surgical intervention, delayed surgical intervention, and nonoperative management. Most orbital fractures do not require urgent surgical intervention and repair can be completed within 2 weeks of the injury.
- •
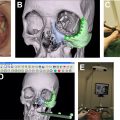
The goal of operative management of orbital fractures includes restoration of globe position, mobility, and orbital volume. Intraoperative computed tomography has become more frequently used and can lead to improved intraoperative plate positioning.
Introduction
Orbital trauma is a commonly seen athletic injury. It is estimated that between 40,000 and 600,000 physician visits per year are sports-related ocular injuries in the United States. Sports-related ocular injuries also have potential for major morbidity. Orbital trauma is the second leading cause of blindness and sports are responsible for one-third of eye injuries that lead to blindness. Because of the risk of blindness, care for the globe is of utmost importance. Certain sports have a greater propensity for orbital injury and those include baseball/softball, paintball, basketball, racquetball, football, and soccer. Maxillofacial trauma makes up approximately 21% of sports-related fractures, and orbital floor fractures make up about 17% of that cohort. With a high degree of concurrent cerebral and ocular injuries, care for the patient with ocular trauma must be appropriately triaged. Once patients have undergone safe triage, care for orbital trauma can occur. Orbital fractures can range from small, nondisplaced fractures, to large fractures with significant orbital disruption. Owing to their complex nature, a large range of factors must be considered in the management of orbital trauma.
Evaluation
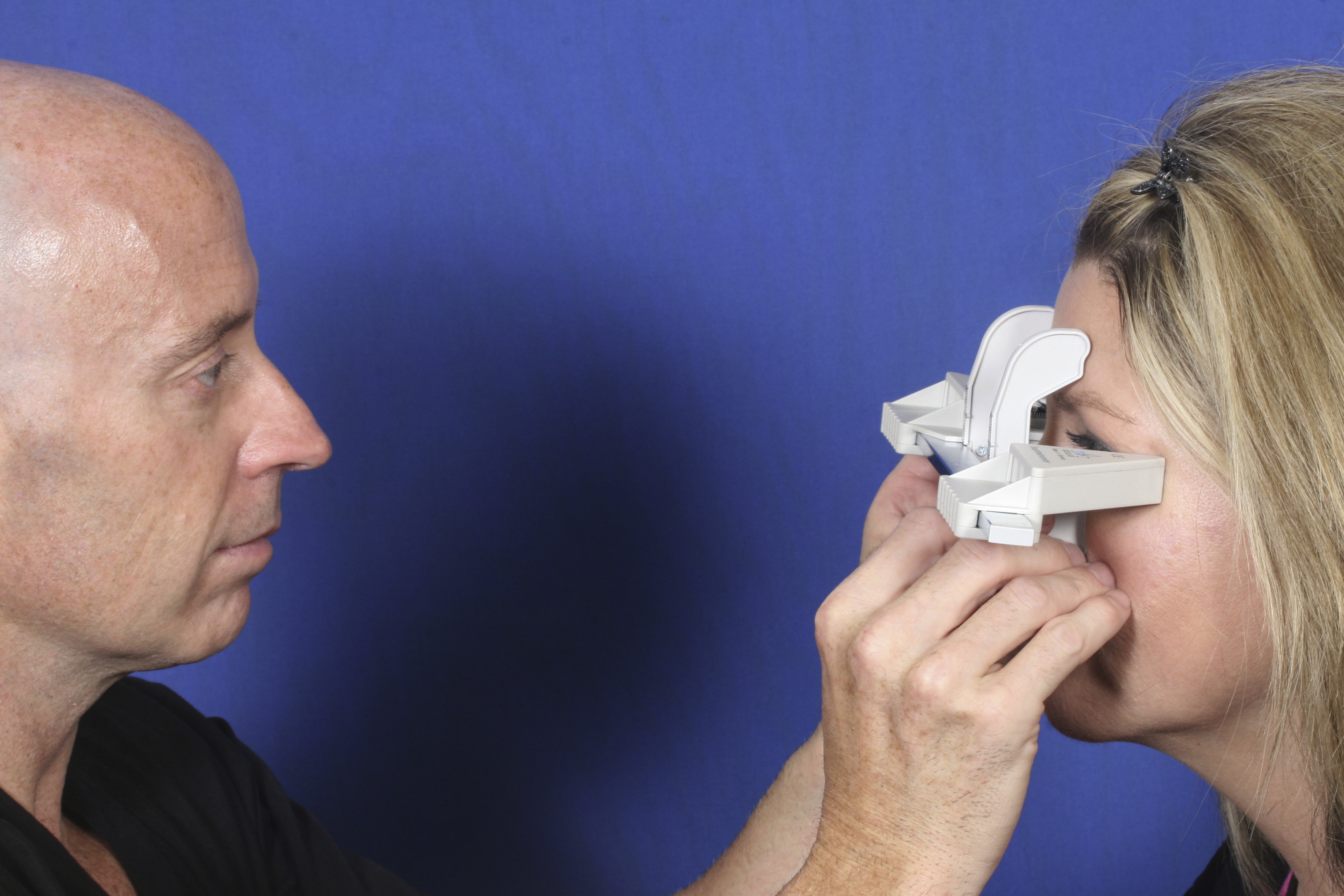
Evaluation should begin with clinical history, comprehensive review of systems, and physical examination. In patients who sustain traumatic injury to the face, orbital trauma should be suspected. Maintaining a high index of suspicion can help enhance the detection of occult fractures. A complete ophthalmic evaluation should be performed. A focused history should include the mechanism of injury and current symptoms. A prior history of ocular conditions and pathologies should also be performed. Visual acuity of individual eyes, pupillary response, and extraocular mobility are paramount to the initial examination. Although enophthalmos and hypoglobus are not always manifested in the acute setting, these findings are associated with increased intraorbital volume after large orbital fractures. Enophthalmos is best detected by taking exophthalmometry measurements ( Fig. 1 ).
Extraocular mobility limitations are common after orbital fracture, but several distinct etiologies can lead to this finding. Both orbital edema and hemorrhage involving the muscles may lead to restriction in movements. Entrapment of muscle or perimuscular tissue can also lead to restrictions, but this is usually associated with pain and guarding. An increase in intraocular pressure greater than 4 mm Hg when looking in the direction of the diplopia may also signify restriction. Contrarily, paralytic diplopia because of nerve injury will not demonstrate increased intraocular pressure or pain. Multidirectional mobility limitations or “frozen globe,” may signify retrobulbar hematoma. This typically manifests with concurrent increased intraocular pressure and proptosis. This is a medical emergency in which canthotomy and cantholysis should be performed to release pressure on the optic nerve.
Evaluation of the ocular adnexa should also be performed. The examination should include the lacrimal system, medial and lateral canthal tendons, and evaluation of telecanthus. A full cranial nerve examination should be performed to evaluate for trigeminal and facial nerve injury.
Ophthalmology consultation and evaluation for all patients with orbital trauma should be considered, as ophthalmologist may recognize ocular pathology at greater rates than nonophthalmologist. , A thorough ophthalmologic examination can help identify ocular foreign bodies, rupture of the globe, altered intraocular pressure, retinal and posterior segment pathology, and lens dislocation. Approximately, 20% of orbital fractures have some associated ocular pathology. The most common findings include commotio retinae, traumatic mydriasis, and traumatic iritis.
Additional testing
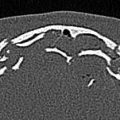
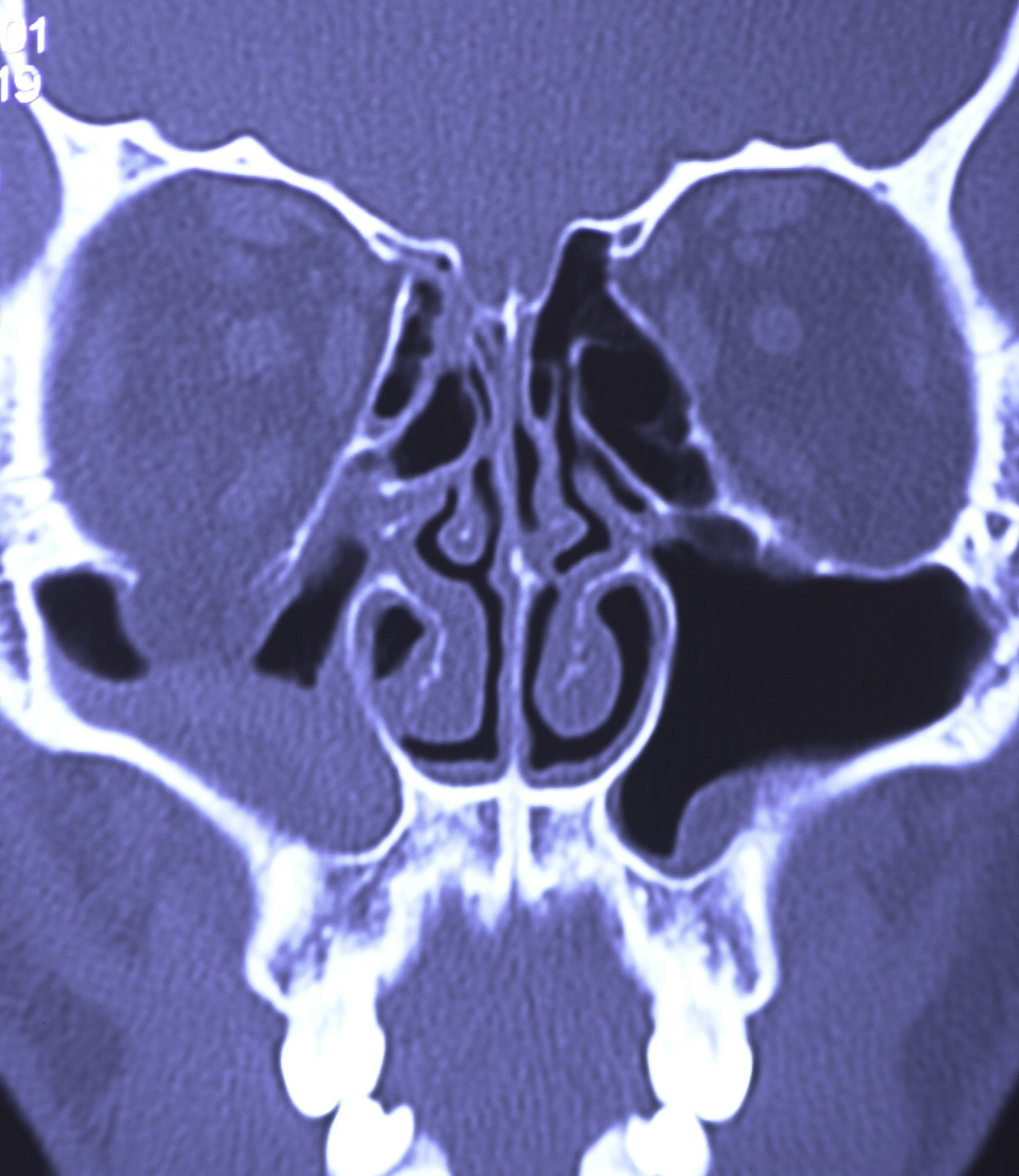
The mainstay of diagnostic testing after orbital trauma is radiological evaluation. Computed tomography (CT) imaging is the gold standard for evaluation of the bony orbit. Fine cuts (<2 mm) should be performed to achieve optimal evaluation of the orbital bone. CT imaging should be thoroughly evaluated in multiple planes. The coronal plane helps identify medial wall fractures as well as orbital floor fractures ( Fig. 2 ). Inferior entrapment may demonstrate a rounded or vertically oriented ovoid shape to the inferior rectus muscle. In addition, inferior rectus rounding may occur during disruption of the fascial sling which supports the orbit. The sagittal plane can aid in understanding the depth and length of an orbital floor fracture.
MRI is generally not necessary in the assessment of orbital trauma. MRI should not be performed as first-line imaging. A CT or plain film should be acquired first to rule out foreign bodies within the orbit. Despite CT imaging being the mainstay of diagnostic testing, some have suggested that soft tissue intraorbital injury may play a larger role in predicting outcomes after orbital fracture. For this reason, MRI has been suggested as a means to help further define treatment strategies in difficult cases. If there is concern for optic nerve, extraocular muscle, or cavernous sinus injury, then MRI may have additional utility.
Numerous studies have analyzed fracture size, location (involvement of anterior or posterior walls, orbital strut), soft tissue displacement, inferior rectus rounding, and other features to predict the development of latent enophthalmos, but these have had varied success. Orbital volume ratios have also been used to predict the need for surgical intervention with inconsistency. ,
Orbital fracture patterns
Orbital Floor
The bony orbit is a conical structure and has a volume of approximately 30 mL. The inferior orbital wall, or orbital floor, forms the roof of the maxillary sinus. It is formed by the maxillary, zygomatic, and palatine bones. The infraorbital nerve courses the length of the orbital floor. As the most dependent portion of the orbit, orbital contents including inferior rectus and orbital fat rest along the floor. Orbital floor fractures may or may not include the inferior orbital rim. Fractures of the orbital floor are the most common orbital fracture pattern. The floor is thinnest medial to the infraorbital nerve, and this serves as the most common location for fracture.
Medial Orbital Wall
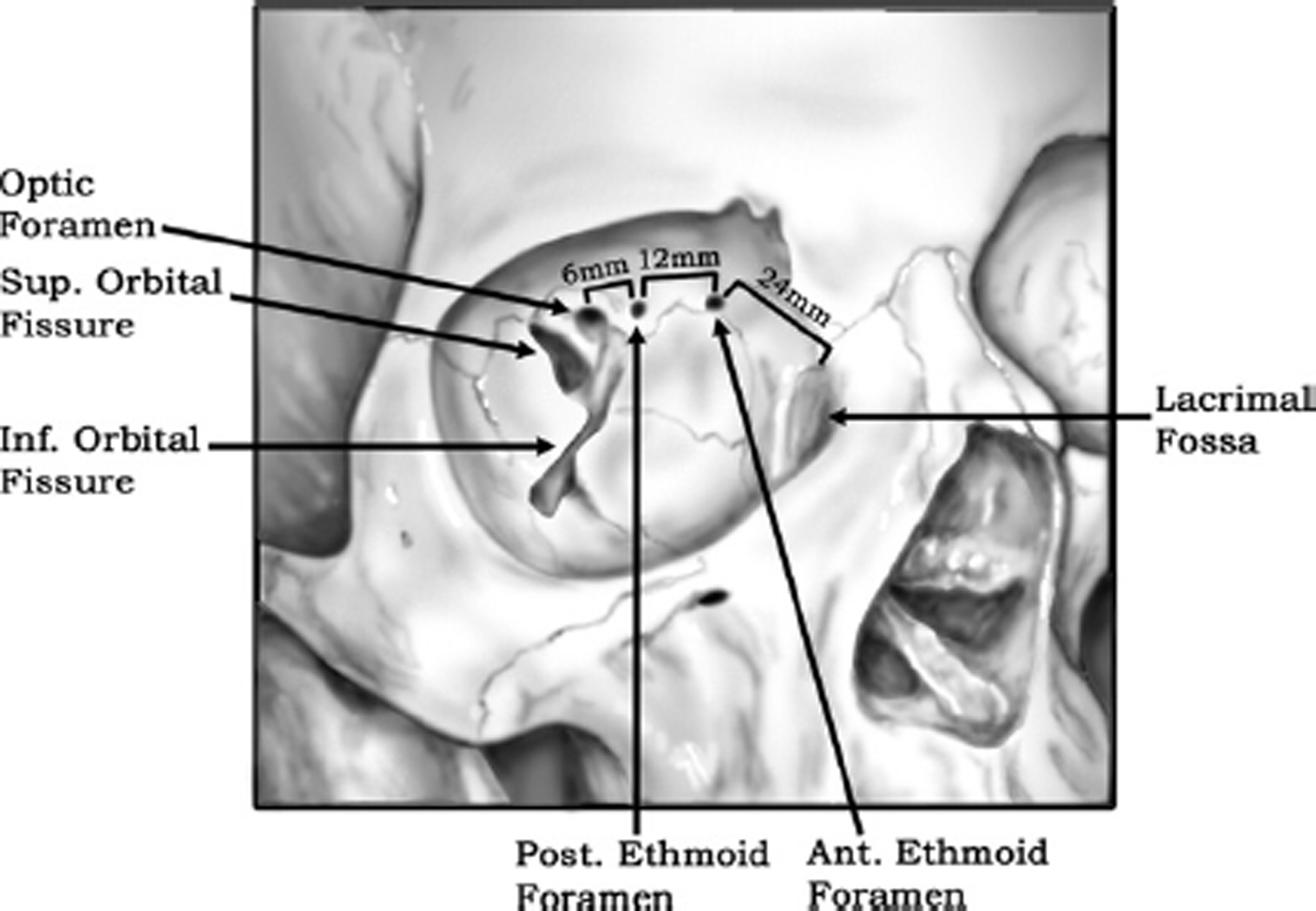
The medial orbital wall is the thinnest of all orbital walls. It is formed by the maxillary, ethmoid, lacrimal, and sphenoid bones. It is thinnest along the lamina papyracea of the ethmoid bone. The ethmoid bone joins with the orbital roof at the frontoethmoidal suture line. It is at this point where anterior and posterior ethmoid foramina are located. Their respective ethmoidal arteries course through these foramina after branching from the ophthalmic artery. The anterior ethmoid neurovascular bundle is typically 20 to 25 mm posterior to the lacrimal crest, whereas the posterior ethmoid neurovascular bundle is another 12 mm posterior to the anterior foramina. The optic canal typically lies 4 to 8 mm posterior to the posterior foramina ( Fig. 3 ). Medial wall fractures can occur in isolation or in combination with orbital floor fractures. Inferiorly, the medial orbital wall transitions to the thick orbital strut bone which is often resistant to fracture.
Orbital Roof
The frontal bone and the lesser wing of the sphenoid make up the orbital roof. The roof separates the orbit from the frontal sinus as well as the anterior cranial fossa. Orbital roof fractures are less common, but their potential for morbidity is high. There are 4 general classifications for orbital roof fractures: “blow in fractures” with inferior displacement of the roof, “blow up fractures” with superior roof displacement into the anterior cranial fossa, supraorbital rim fractures, and frontal sinus fractures. Fractures that involve the anterior cranial fossa may lead to pneumocephalus or a dural tear resulting in cerebrospinal fluid leak. A high-impact injury is required to sustain a roof fracture as there is protection from the surrounding frontal sinus. When orbital roof fractures occur, concurrent traumatic brain injury with intracranial hemorrhage can be seen in approximately two-thirds of cases. Evaluation of orbital roof fractures should involve not only the facial trauma team but also ophthalmology and neurosurgery.
Combined Orbital Fractures
Combined fractures of both the orbital floor and medial orbital wall are not uncommon and can occur in up to 35% of cases. As the orbital wall(s) defect size is increased, the degree of enophthalmos is also increased. Patients with combined fractures have been shown to have a statistically significant change in exophthalmometric measurements compared to those with isolated orbital floor fracture. These fracture patterns can make reconstruction challenging if there is a loss of inferonasal support at the orbital strut. In addition, involvement of the inferior oblique muscle near the lacrimal fossa can complicate reconstruction.
Management
Orbital Floor Fractures
Management of orbital floor fractures can be broken down into 3 main treatment pathways: urgent surgical intervention, delayed surgical intervention, and nonoperative management. Most orbital fractures do not require urgent surgical intervention and repair can be completed within 2 weeks of the injury.
Immediate repair (within the first 48 hours after injury) should be performed if there is a concern for oculocardiac reflex which manifests as bradycardia, nausea, and/or syncope. This reflex occurs secondary to soft tissue entrapment or increased intraorbital pressure. The ophthalmic division of the trigeminal nerve carries afferent fibers to the ciliary ganglion. Vagal nerve efferent signals are then transmitted to both the cardiac and gastric tissues. Life-threatening cardiac arrhythmia may ensue if no intervention is performed. In the absence of oculocardiac reflex, immediate repair has remained controversial and management likely depends on training and experience.
Specific indications for orbital floor repair include clinical (positive force duction testing) and radiological concern for entrapment, enophthalmos greater than 2 mm, and orbital wall defects greater than 2 cm 2 . If enophthalmos develops immediately after injury, then this will not improve without surgical repair. In addition, pediatric trapdoor (white-eye blowout) fractures in which orbital tissue is trapped between bony fragments warrants urgent repair. In cases of entrapment or incarceration, prolonged muscle ischemia can lead to a Volkmann’s type contracture of the extraocular muscles. Evidence of globe rupture, hyphema, or other ocular injuries should delay internal orbit repair approaches until an ophthalmology evaluation and repair has been completed.
In cases that do not necessitate immediate repair, delayed surgical intervention can be considered. Repeat evaluation should be performed within 2 weeks of injury. A better clinical evaluation can be performed after orbital edema and hemorrhage have improved. Transient diplopia is a common finding in the immediate postinjury setting, and this may be due to muscle contusion and/or intraorbital edema. Edema typically improves within 2 weeks of injury, and any persistent diplopia is a compelling sign for intervention. Delayed repair affords improved exposure and mitigates risk of orbital compartment syndrome; however, delay does increase the risk of impinged tissue undergoing fibrosis and resulting in chronic diplopia. ,
Indications for delayed repair of the orbital floor include latent enophthalmos, significant hypoglobus, and progressive hypesthesia along the infraorbital nerve. Significant rounding of the inferior rectus muscle in which the height-to-width ratio is greater than 1.00 has been shown to be predictive of development of latent enophthalmos. Difficult clinical decision-making occurs when ocular motility has improved, but enophthalmos persists. In these scenarios, fracture defect size on CT imaging and individualized patient approach can be helpful. Athletes likely have a lesser degree of tolerance for gaze-induced diplopia compared to an elderly, more sedentary patient.
In some cases, patients may present in a delayed fashion, months to years after injury. In these cases, it has been shown that delayed repair is still useful. Scawn and colleagues repaired 20 late presenting orbital floor fractures (mean presentation time of 19 months after injury) in patients with greater than 2 mm of enophthalmos or diplopia within 30° of primary gaze. Even at a later time of initial presentation, improvement in symptoms is still achievable.
In patients with minimal diplopia (not in the primary or downward gaze fields), good ocular mobility, and no enophthalmos or hypoglobus, they are unlikely to require repair. Additional management for nonoperative patients should include sinus precautions and education regarding avoidance of nose-blowing, as this can force air into the orbit. In severe cases, tension pneumo-orbit can lead to a compartment syndrome resulting in optic nerve compression and blindness. Cold compress and head of bed elevation can reduce orbital edema. If lagophthalmos is present, then corneal protection is required. Best evidence suggests that prophylactic antibiotic use is of minimal utility in upper or midface facial fractures. There is some evidence that patients with pre-existing sinus disease or active sinus infection may be at increased risk of development of orbital cellulitis.
Medial Orbital Wall Fractures
The clinical consequence of fractures along the medial orbital wall can be difficult to predict, but in general, these fractures can be managed conservatively. There is less data regarding clinical guidelines for repair of isolated medial wall fractures, but extrapolation of isolated orbital floor guidelines has led to recommendations. Entrapment based on positive forced duction testing of the medial rectus as well as early enophthalmos are indications for repair. The more common pathophysiologic mechanism by which medial wall fractures limit patient function is by change in orbital volume. Because of this, latent enophthalmos and diplopia also warrant repair.
Orbital Roof Fractures
Recognition of orbital roof fractures is paramount in reducing intracranial or orbital complications. Most orbital roof fractures are minimally displaced and can be managed conservatively. There is a lack of consensus on exactly which symptoms warrant surgery versus conservative management. Because of the rarity of these fractures, guidelines are largely anecdotal, and treatment should be individualized. Blow-in fractures that lead to exophthalmos, levator dysfunction, or entrapment should be considered for undergoing repair. Blow-up fractures that lead to dural tears, bone fragments in the anterior cranial fossa, and refractory oculorrhea should also be considered for repair.
Concurrent Orbital and Zygomaticomaxillary Complex Fractures
It is not uncommon for both orbital and zygomaticomaxillary complex (ZMC) fractures to occur concurrently. This is most commonly seen when an inferior orbital fissure fracture line extends along the orbital floor toward the orbital process of the maxilla and infraorbital rim. Traditionally, orbital floor exploration was part of the treatment paradigm for ZMC fractures. With the increased use of CT imaging, the rate of orbital exploration significantly dropped from 90% in 1985 to 30% in 1989. But even with increased use of preoperative imaging, there is still a concern that during ZMC reduction a change in orbital volume could precipitate enophthalmos or diplopia. Ellis and colleagues looked at this issue and demonstrated that inferior displacement of the orbital floor is rare (6 of 65 cases), and when it occurs, the amount of displacement is small. Because of these findings, it is generally thought that approach and repair of small orbital fractures are not necessary after appropriate reduction of the ZMC. Intraoperative imaging can be used for assessment of orbital fractures following ZMC reduction, but this has been shown to result in a rare need to repair the orbit. Despite the evidence supporting observation of small concurrent orbital fractures when repairing the ZMC, many still concurrently explore and/or repair the orbit in clinical practice.
Management of Pediatric Orbital Trauma
Pediatric orbital fractures vary in their fracture pattern as the child ages due to the ongoing developmental anatomy. The immaturity of the pediatric skeleton demonstrates higher levels of cancellous bone which gives the pediatric facial bones higher levels of elasticity and resistance to fracture. This characteristically results in “greenstick” fractures. As the child ages, increased bone mineralization occurs, and the bone becomes more rigid. In addition, the pediatric population has a greater cranial:facial ratio. Because of the partial or absent pneumatization of the sinuses in younger pediatric populations, there is even greater resistance to fracture. In fact, it has been determined that before age 7 years, orbital roof fractures are more common than orbital floor fractures.
Although periorbital edema and ecchymosis are commonly seen in adult patients with orbital fractures, pediatric patients may present without these findings. This type of fracture is called a “white eye” blowout fracture. These fractures have a higher rate of entrapment when compared with adult patients because of the elasticity of the pediatric bone. Assessment of entrapment may be more difficult in the pediatric patient, and as such, oculocardiac reflex or nausea and vomiting may be the most apparent clinical finding.
Because of the resiliency of the pediatric elastic connective tissues and ligamentous attachments, they are less likely to develop enophthalmos and vertical dystopia. Pediatric fractures are typically able to be observed at higher incidence than adult fractures. Patients with minimal diplopia, unrestricted ocular motility, no evidence of muscle or soft tissue entrapment on CT imaging, and improvement within 2 weeks can be observed. In cases of entrapment or enophthalmos, surgical intervention is warranted. Pediatric orbital fractures are typically approached similar to adults, but unlike adults, rigid titanium mesh may not be the ideal fixation material for the immature facial skeleton. Instead, resorbable plates have been suggested.
Return to Play After Orbital Trauma in Athletes
There are no set guidelines for return to play after orbital trauma. Determination for return to play is largely based on the athlete’s ability to function at his or her pretraumatized level. If binocular vision is restored and patient is without functional deficits, then consideration for play can be made. If an injury has occurred in a patient’s only seeing eye, then great caution should be taken before considering return to play.
When considering return to play, athletes should be counseled on proper protective equipment. Evidence suggests that 90% of ocular injuries are preventable with proper eye protection. Sport-specific eyewear has been recommended by the American Academy of Pediatrics and the American Academy of Ophthalmology. Regrettably, it is estimated that only 15% of children in organized sports adhere to proper eye protection guidelines.
There has been a growing trend of professional athletes donning protective prosthetic face masks after maxillofacial trauma. This use has triggered interest among younger, nonprofessional athletes. There is inherent risk to early return to play after orbital fracture, but prosthetic facemasks can provide some degree of protection against refracture. These facemasks are designed to redistribute forces acquired during sports-related contact to protect the maxillofacial skeleton. Over-the-counter facemasks are available as an affordable option, whereas custom-made masks can also be created from a mold of the player’s face. Currently, there is little scientific evidence to suggest superiority of certain facemask types for prevention of repeat injury.
Surgical techniques
Approaches to the Orbital Floor
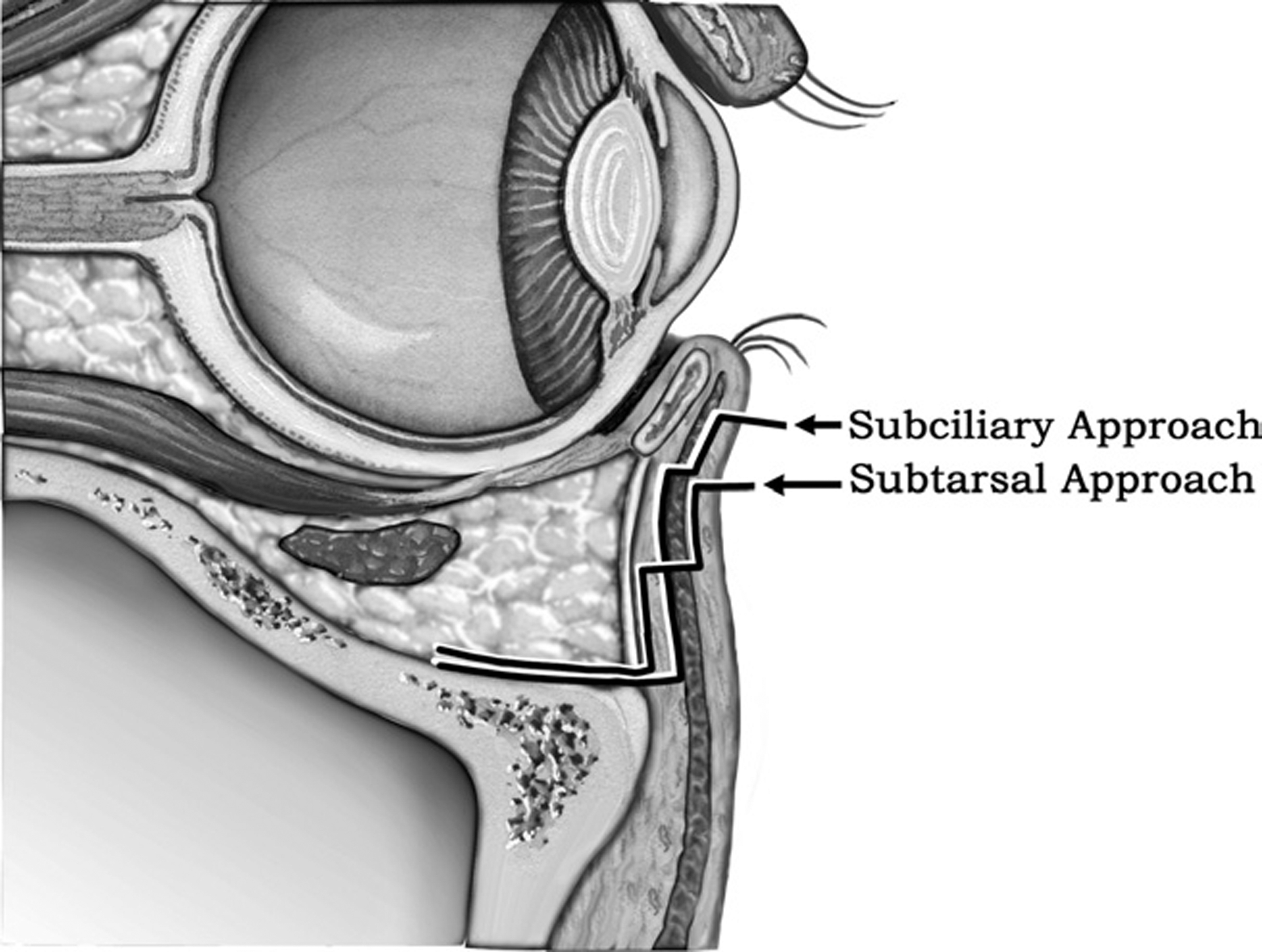
Subcilliary/subtarsal approach
Both the subcilliary and subtarsal approaches are transcutaneous approaches, which were originally described in 1944. Both these approaches begin with the placement of a temporary lateral tarsorrhaphy stitch, which can be used for eye protection and retraction. Incision for the subcilliary approach is carried out 2 mm below the lash line and runs parallel to its course. The incision should not be carried more medially than the lower lid punctum but can extend 15 mm beyond the lateral canthus. Dissection is carried inferior to the tarsal plate in a plane superficial to the orbicularis oculi to maintain the lower lid structural support. The dissection then continues toward the orbital rim in a preseptal plane until the periosteum is encountered. At this point, the periosteum is incised, and periosteal elevator is used to expose the orbital floor ( Fig. 4 ). If a subtarsal approach is used, then the incision is created in the subtarsal fold (approximately 5–7 mm below the lash line). Dissection through the orbicularis oculi should be performed 2 to 3 mm below the level of the skin incision to decrease the likelihood of ectropion or scar inversion. Although these approaches provide excellent exposure to the orbital floor, they will typically have a visible scar and increased probability of lower lid malposition compared with the transconjunctival approach.