Accurate diagnosis of cutaneous disease in infants and children is a systematic process that requires careful inspection, evaluation, and some knowledge of dermatologic terminology and morphology to develop a prioritized differential diagnosis. The manifestations of skin disorders in infants and young children often vary from those of the same diseases in older children and adults. The diagnosis may be obscured, for example, by different reaction patterns or a tendency toward easier blister formation. In addition, therapeutic dosages and regimens often differ from those of adults, with medications prescribed on a “per kilogram” (/kg) basis and with liquid formulations.
Nevertheless, the same basic principles that are used to detect disorders affecting viscera apply to the detection of skin disorders. An adequate history should be obtained, a thorough physical examination performed, and, whenever possible the clinical impression verified by appropriate laboratory studies. The easy visibility of skin lesions all too often results in a cursory examination and hasty diagnosis. Instead, the entire skin should be examined routinely and carefully, including the hair, scalp, nails, oral mucosa, anogenital regions, palms, and soles, because visible findings often hold clues to the final diagnosis.
The examination should be conducted in a well-lit room. Initial viewing of the patient at a distance establishes the overall status of the patient and allows recognition of distribution patterns and clues to the appropriate final diagnosis. This initial evaluation is followed by careful scrutiny of primary and subsequent secondary lesions in an effort to discern the characteristic features of the disorder.
Although not always diagnostic, the morphology and configuration of cutaneous lesions are of considerable importance to the classification and diagnosis of cutaneous disease. A lack of understanding of dermatologic terminology commonly poses a barrier to the description of cutaneous disorders by clinicians who are not dermatologists. Accordingly, a review of dermatologic terms is included here ( Table 1-1 ). The many examples to show primary and secondary skin lesions refer to specific figures in the text that follows.
| Lesion | Description | Illustration | Examples |
|---|---|---|---|
| PRIMARY LESIONS | |||
| The term primary refers to the most representative, but not necessarily the earliest, lesions; it is distinguished from the cutaneous features of secondary changes such as excoriation, eczematization, infection, or results of previous therapy. | |||
| Macule | Flat, circumscribed change of the skin. It may be of any size, although this term is often used for lesions <1 cm. A macule may appear as an area of hypopigmentation or as an area of increased coloration, most commonly brown (hyperpigmented) or red (usually a vascular abnormality). It is usually round but may be oval or irregular; it may be distinct or may fade into the surrounding area. |  | Ephelides; lentigo (see Fig. 11-41 ); flat nevus (see Fig. 9-1 ); and tinea versicolor (see Fig. 17-35 ). |
| Patch | Flat, circumscribed lesion with color change that is >1 cm in size. |  | Mongolian spot (see Fig. 11-57 ); port wine stain (see Fig. 12-57 ); nevus depigmentosus (see Fig. 11-22 ); larger café-au-lait spot (see Fig. 11-43 ); and areas of vitiligo (see Fig. 11-1 , Fig. 11-2 , Fig. 11-3 , Fig. 11-4 , Fig. 11-5 , Fig. 11-6 , Fig. 11-7 , Fig. 11-8 , Fig. 11-9 , Fig. 11-10 ). |
| Papule | Circumscribed, nonvesicular, nonpustular, elevated lesion that measures <1 cm in diameter. The greatest mass is above the surface of the skin. When viewed in profile it may be flat-topped, dome-shaped, acuminate (tapering to a point), digitate (finger-like), smooth, eroded, or ulcerated. It may be covered by scales, crusts, or a combination of secondary features. |  | Elevated nevus (see Fig. 9-4 ); verruca (see Fig. 15-17 ); molluscum contagiosum (see Fig. 15-40 ); perioral dermatitis (see Fig. 8-20 ); and individual lesions of lichen planus (see Fig. 4-43 ). |
| Plaque | Broad, elevated, disk-shaped lesion that occupies an area of >1 cm. It is commonly formed by a confluence of papules. | 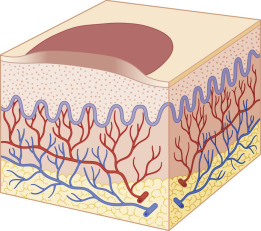 | Psoriasis (see Fig. 4-4 ); lichen simplex chronicus (neurodermatitis) (see Fig. 3-37 ); granuloma annulare (see Fig. 9-58 ); nevus sebaceus (see Fig. 9-41 , Fig. 9-42 , Fig. 9-43 , Fig. 9-44 ); and lesions of lichen planus (see Fig. 4-45 ). |
| Nodule | Circumscribed, elevated, usually solid lesion that measures 0.5 to 2 cm in diameter. It involves the dermis and may extend into the subcutaneous tissue with its greatest mass below the surface of the skin. | 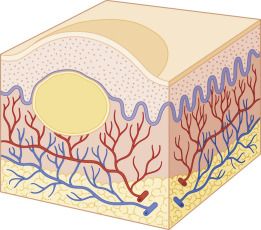 | Erythema nodosum (see Figs. 20-44 and 20-45 ); pilomatricoma (see Fig. 9-48 ); subcutaneous granuloma annulare (see Fig. 9-60 ); and nodular scabies (see Fig. 18-9 ). |
| Tumor | Deeper circumscribed solid lesion of the skin or subcutaneous tissue that measures >2 cm in diameter. It may be benign or malignant. | 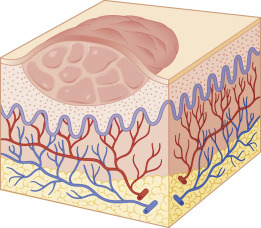 | Deep hemangioma (see Fig. 12-7 ) and plexiform neurofibroma ( Fig. 11-50 ). |
| Wheal | Distinctive type of elevated lesion characterized by local, superficial, transient edema. White to pink or pale red, compressible, and evanescent, they often disappear within a period of hours. They vary in size and shape. | 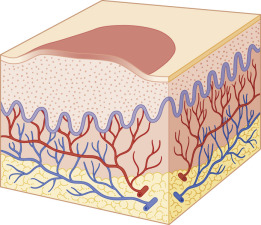 | Darier sign of mastocytosis (see Fig. 9-52 ); urticarial vasculitis (see Fig. 21-14 ); and various forms of urticaria (see Fig. 20-2 ). |
| Vesicle | Sharply circumscribed, elevated, fluid-containing lesion that measures ≤1 cm in diameter. |  | Herpes simplex (see Figs. 2-47 , 15-10 and 15-11 ); hand-foot-and-mouth disease (see Fig. 16-30 ); pompholyx (see Fig. 3-41 ); varicella (see Fig. 16-1 ); and contact dermatitis (see Fig. 3-57 ). |
| Bulla | Larger, circumscribed, elevated, fluid-containing lesion that measures >1 cm in diameter. |  | Blistering distal dactylitis (see Fig. 14-21 ); bullous pemphigoid (see Fig. 13-26 ); chronic bullous disease of childhood (see Fig. 13-29 ); bullous systemic lupus erythematosus (see Fig. 13-32 ); and epidermolysis bullosa (see Fig. 13-4 ). |
| Pustule | Circumscribed elevation <1 cm in diameter that contains a purulent exudate. It may be infectious or sterile. |  | Folliculitis (see Fig. 14-11 ); transient neonatal pustular melanosis (see Fig. 2-17 ); pustular psoriasis (see Fig. 4-22 ); and infantile acropustulosis (see Fig. 2-19 ). |
| Abscess | Circumscribed, elevated lesion >1 cm in diameter, often with a deeper component and filled with purulent material. |  | Staphylococcal abscess (in a neonate, see Fig. 2-5 ; in a patient with hyperimmunoglobulinemia E, see Fig. 3-35 ). |
| OTHER PRIMARY LESIONS | |||
| Comedone | Plugged secretion of horny material retained within a pilosebaceous follicle. It may be flesh colored (as in closed comedone or whitehead) or slightly raised brown or black (as in open comedone or blackhead). Closed comedones, in contrast to open comedones, may be difficult to visualize. They appear as pale, slightly elevated, small papules without a clinically visible orifice. | Acne comedones (see Figs. 8-3 and 8-4 ) and nevus comedonicus (see Fig. 9-45 ). | |
| Burrow | Linear lesion produced by tunneling of an animal parasite in the stratum corneum. | Scabies (see Fig. 18-3 ) and cutaneous larva migrans (creeping eruption, see Fig. 18-39 ). | |
| Telangiectasia | Persistent dilation of superficial venules, capillaries, or arterioles of the skin. | Spider angioma (see Fig. 12-86 ); periungual lesion of dermatomyositis (see Fig. 22-25 ); and Goltz syndrome (see Fig. 6-15 ). | |
| SECONDARY LESIONS | |||
| Secondary lesions represent evolutionary changes that occur later in the course of the cutaneous disorder. Although helpful in dermatologic diagnosis, they do not offer the same degree of diagnostic aid as that afforded by primary lesions of a cutaneous disorder. | |||
| Crust | Dried remains of serum, blood, pus, or exudate overlying areas of lost or damaged epidermis. Crust is yellow when formed by dried serum, green or yellowish-green when formed by purulent exudate, and dark red or brown when formed by bloody exudative serum. | 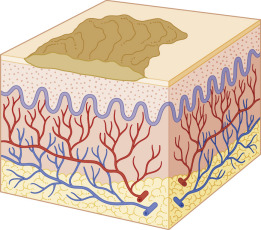 | Herpes simplex (see Fig. 15-4 ); weeping eczematous dermatitis (see Fig. 3-1 ); and dried honey-colored lesions of impetigo (see Fig. 14-2 ). |
| Scale | Formed by an accumulation of compact desquamating layers of stratum corneum as a result of abnormal keratinization and exfoliation of cornified keratinocytes. | 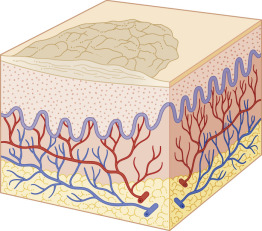 | Seborrheic dermatitis (greasy and yellowish, see Figs. 3-2 and 3-39 ); psoriasis (silvery and mica-like, see Fig. 4-1 ); pityriasis alba (fine and barely visible, see Fig. 3-33 ); and lamellar ichthyosis (large and adherent, see Fig. 5-10 ). |
| Fissure | Dry or moist, linear, often painful cleavage in the cutaneous surface that results from marked drying and long-standing inflammation, thickening, and loss of elasticity of the integument. | 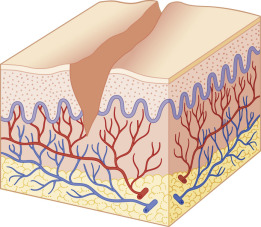 | Angular cheilitis (see Fig. 17-40 ) and dermatitis on the plantar aspect of the foot (see Fig. 3-61 ). |
| Erosion | Moist, slightly depressed vesicular or bullous lesions in which part or all of the epidermis has been lost. Because erosions do not extend into the underlying dermis or subcutaneous tissue, healing occurs without subsequent scar formation. | 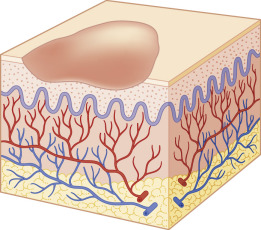 | Herpes simplex (see Figs. 3-28 and 15-1 ); epidermolytic ichthyosis in a neonate (see Fig. 5-4 ); and superficial forms of epidermolysis bullosa (see Fig. 13-7 ). |
| Excoriation | Traumatized or abraded (usually self-induced) superficial loss of skin caused by scratching, rubbing, or scrubbing of the cutaneous surface. | 
| |