A Perspective from Military Medicine
Peter R. Shumaker
Thomas Beachkofsky
Andrew Basnett
Carrick Burns
Nathan Uebelhoer
Chad Hivnor
KEY POINTS
More than a decade of conflict and unprecedented battlefield survival rates led to an enormous influx of military personnel in need of functional and cosmetic rehabilitation.
To adapt to the challenges posed by the number and the severity of the injuries and the high expectations for recovery of these young patients, new paradigms of coordinated multidisciplinary care emerged at multiple military centers of excellence in rehabilitation.
Among the benefits of this type of collaborative environment are innovative approaches to care; the routine inclusion of dermatologists and their expertise in a variety of minimally invasive cutaneous procedures has enhanced ongoing rehabilitative efforts and is helping to change paradigms both within and outside the military system.
The benefits of procedures such as ablative fractional laser resurfacing (AFR) for traumatic scars and laser hair reduction for amputees are certainly not limited to battlefield trauma, and millions of patients worldwide may benefit from these and future techniques regardless of the source of injury.
Scar management in the military setting presents many unique challenges and opportunities. Extended conflict and increased battlefield survival has left thousands of otherwise young and healthy individuals in need of long-term rehabilitation and reintegration following devastating injuries including burns, amputations, and traumatic brain injury. The need to address multiple complex medical and psychosocial issues effectively and efficiently has ushered in unprecedented levels of multidisciplinary collaboration at three military advanced rehabilitation centers of excellence including the Military Advanced Training Center (MATC) at Walter Reed National Military Medical Center in Bethesda, Maryland; the Center for the Intrepid (CFI) at Brooke Army Medical Center in San Antonio, Texas; and the Comprehensive and Complex Casualty Care Center (C5) at the Naval Medical Center San Diego. Several aspects of military medicine are conducive to collaboration and the early adoption of new innovations including a focus on mission accomplishment, ongoing experience working in cohesive multidisciplinary teams during both peacetime and conflict, and a relative lack of financial disincentives that more commonly impact civilian practice. The emergence of dermatologists as routine partners in trauma rehabilitation is a product of this environment. This chapter highlights a treatment approach and a variety of minimally invasive cutaneous procedures from the perspective of military dermatologists at two different military centers. Like so many medical advancements in history, the vast majority of the patients that may ultimately benefit from these techniques will never wear a uniform.
Unusual Aspects of Military Practice
Inherent characteristics of the wounded warrior have driven rehabilitation after major trauma to new heights, both literally and figuratively.1 They are often young, motivated, goal oriented, and otherwise healthy and active at baseline before injury. For this cohort of recovering service personnel, simply walking or completing activities of daily living is not good enough. Patients want to return to activities as close as possible to baseline (or even higher) levels of functioning and participate in a range activities such as snowboarding, surfing, hiking, biking, swimming, and running. Others, including amputees, have returned to full duty and even deployed back to combat zones.2 Minimally invasive procedures such as laser scar revision, laser hair reduction, and procedural sweat reduction are extremely effective adjuncts to traditional rehabilitative efforts such as physical and recreational therapy, prosthetics, mental health support, and medical and surgical management.
The psychosocial impact of a scar can vary widely from person to person depending on the size, location, symptoms, and myriad other factors. In the experience of the authors, however, the attitude of a military patient toward the presence of the scar is frequently not as uniformly negative as in nonmilitary patients. For some, the scar may be a badge of honor or a reminder of friends lost; an outward symbol of dedication and sacrifice. Although the mere presence of a scar may not always be problematic, the desire to improve functionality and reduce symptoms such as pain and itch is universal. By the time a polytrauma patient enters the clinic they may have endured numerous surgical procedures requiring general anesthesia. Many patients are grateful to have effective and minimally invasive procedures in the clinic setting. Surprisingly, they can be tolerant of temporary mild to moderate pain associated with an array of cutaneous procedures. Posttraumatic stress and anxiety are relatively common, however, and triggers such as the smell of smoke, noise, and burning pain are wisely anticipated and mitigated during treatment.
Centers of Excellence
After the entry of the United States into the conflicts in Afghanistan and Iraq in the early 2000s, the emergence of the improvised explosive device as a pervasive weapon combined with advances in battlefield resuscitation and transportation resulted in an unprecedented number of survivors with multiple severe injuries and associated sequelae including burns, amputations, disfigurement, traumatic brain injury, posttraumatic stress disorder, and loss of hearing and eyesight.3,4 Simultaneously, an enhanced awareness of the need for higher levels of care for veterans became apparent to the American public. Thus, a highly coordinated multidisciplinary approach to rehabilitation including MATC, CFI, and C5 emerged. Additionally, other entities such as the Extremity Amputation Center of Excellence (EACE) and the Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury began to collaborate through a national network to facilitate ongoing clinical care and research. The requirement for ongoing care, the need to retain skills and capacity to account for future conflicts, and the fact that coordinated care benefits patients regardless of the source of injury help ensure that these centers will have an enduring role.
 FIGURE 23-1 Retired Marine Josue Barron (#35), a member of the Naval Medical Center San Diego (NMCSD) Wolfpack wheelchair basketball team, keeps the ball away from the Fort Sam Warriors. Wolfpack is made up of 13 military and civilian members and is one of 10 teams in the West Coast Conference of the National Wheelchair Basketball Association. (Courtesy of U.S. Navy, photo by Mass Communication Specialist Seaman Pyoung K. Yi/Released.) |
Programs such as C5 operate along a similar model of multidisciplinary care on a residential or drop-in basis, as appropriate. Dedicated program staff provide active case management and patients receive coordinated care as needed through various surgical and medical specialties including but not limited to: orthopedics, neurology, dermatology, physical medicine and rehabilitation, pain management, prosthetics and gait evaluation, mental health, and physical, occupational, and recreational therapy (Fig. 23-1). Additionally, they receive other psychological and social support including pastoral care, family support groups, and career transition resources. These programs are available for all active duty patients, whether or not their injuries are combat related. However, severely injured active duty patients requiring extensive care may be assigned to a rehabilitation program as their primary duty. Often they will reside on the grounds of military medical facility to allow a consolidation of medical resources and a full-time focus on recovery. Patients have access to a broad logistics network facilitating nationwide transfer when necessary, and resources are available to bring and temporarily house patients’ families near the centers. Some patients are ultimately returned to full or modified duty; others are transitioned out of active service with ongoing care coordinated to varying degrees by Veterans Administration (VA) and military treatment facilities depending on
the location, spectrum of injuries, and other factors. The centers have developed resources to assist those with the transition to civilian life.
the location, spectrum of injuries, and other factors. The centers have developed resources to assist those with the transition to civilian life.
International Exchange and Humanitarian Operations
The United States regularly deploys military medical assets around the world to help build durable and effective partnerships with other nations to enhance disaster preparedness and theater security cooperation. The annual Pacific Partnership mission is an excellent example of these efforts; it is the largest multinational humanitarian assistance and disaster preparedness activity in the Indo-Asia-Pacific region. The annual mission began in 2006 following the 2004 tsunami that devastated parts of Southeast Asia. The U.S. Navy deployed assets to the international relief effort, including the hospital ship USNS Mercy. This ship, and its sister ship the USNS Comfort on the east coast of the United States, are fully capable floating hospitals with operating rooms, an intensive care unit, imaging, laboratory, pharmacy, and numerous medical specialists and support staff. The 10th iteration of Pacific Partnership was completed in 2015 and included nine partner nations and multiple nongovernmental organizations participating in activities such as direct medical and surgical care and subject matter expert exchange, public outreach, veterinary services, and engineering projects. Over the course of approximately 4 months in 2015 the Mercy traveled to Fiji, Papua New Guinea, the Philippines, and Vietnam.5
Among the myriad other notable activities during Pacific Partnership 2015, a multidisciplinary team consisting of dermatology, plastic surgery, orthopedics, physical therapy, and other specialties participated in direct care and high-level exchange in the management of severe scars and scar contractures resulting from burns and other trauma. This provided the team an ongoing opportunity to leverage experience gained over more than a decade treating injured service members during wartime to promote cooperation and help ease suffering in multiple corners of Southeast Asia. Combining ablative fractional laser resurfacing (AFR) with surgery and other nonsurgical modalities, numerous patients received cutting-edge treatment to help restore function and appearance during the mission (Fig. 23-2). The hospital ship provides a unique and successful platform to treat patients from a variety of settings. Performed alone or concurrently with surgery, patient follow-up extending up to 4 years from prior missions involving hundreds of patients demonstrates an excellent record of safety and efficacy, even after a single treatment (unpublished experience) (Fig. 23-3). In addition, extensive exchange with host physicians was performed to further enhance sustainable relationships.
 FIGURE 23-2 Service members, assigned to the hospital ship USNS Mercy (T-AH 19), perform a fractional CO2 laser procedure on a child during Pacific Partnership 2015. (Courtesy of U.S. Navy, photo by Petty Officer 2nd Class Mark El-Rayes/Released.) |
Cutaneous Procedures in Trauma Rehabilitation
Military dermatologists have played a significant role in integrating AFR and a variety of other minimally invasive cutaneous procedures into trauma rehabilitation, whether the injuries have been sustained on or off the battlefield. A more comprehensive discussion of laser and other treatments for scars is available in other parts of the text (see Chapters 10, 12, 13 and 14). These devices and techniques are widely available in dermatology and plastic surgery offices around the world, and minor adaptations of these techniques applied regularly for aesthetic applications can help bring life-changing treatment to millions of patients worldwide. This section highlights the experience of the authors at two military centers of excellence: the Naval Medical Center San Diego and the San Antonio Military Medical Center.
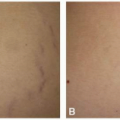
 FIGURE 23-3 A: A 4-year-old girl approximately 16 months after suffering burns over approximately 60% of her total body surface area, and approximately 12 and 4 months from her first and second ablative fractional laser treatments, respectively. Although significant interval enhancements in scar pliability and range of motion were noted, a flexion contracture at the knee and loss of pliability of the tissues surrounding the ankle precluded normal ambulation. B: Approximately 10 months after contracture excision, placement of a bovine collagen and glycosaminoglycan meshed bilayer dressing (INTEGRA Meshed Bilayer Wound Matrix, Integra LifeSciences Corporation, Plainsboro, NJ) and negative pressure wound therapy followed approximately 1 month later by a split-thickness skin graft. A third ablative fractional laser resurfacing procedure (Lumenis UltraPulse, Deep FX, Yokneam, Israel) was performed concurrently with contracture excision over the entire scarred area. Her range of motion had improved significantly and ambulation had largely normalized. This case demonstrates the benefits of multidisciplinary care and long-term collaboration. |
Laser Scar Revision
Treatment Approach
The treatment approach to scars with lasers and light devices in the military setting has been outlined previously.6,7 Although AFR is central to the management of debilitating scarring in the outpatient setting, it is by no means the only useful platform. A range of lasers and light devices that target the three main skin chromophores (water, hemoglobin, and melanin) are routinely used by the authors after trauma. Roughly in descending order of frequency these are: AFR, vascular lasers and light devices (such as the 595-nm pulsed dye laser [PDL]), nonablative fractional resurfacing, long-pulsed pigment-specific lasers for hair reduction, and short-pulsed (Q-switched) pigment-specific lasers for the removal of traumatic tattoos. In many instances, all of these platforms will be used concurrently or in an alternating fashion in the management of a specific patient.
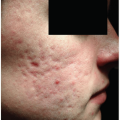
Initial evaluation involves an assessment of scar erythema, degree of healing, pliability, texture, dyspigmentation, thickness, degree of contracture, and proximity to joints and free edges. Additionally, prior treatments, future surgical intervention, prosthetic use, sensitivity and pain syndromes, and the presence of posttraumatic stress should be considered when developing a treatment plan. Far from being a replacement for traditional interventions, laser treatments are most effective when complemented by ongoing multidisciplinary care including physical and occupational therapy and surgical and nonsurgical medical consultation. Because of the minimally invasive nature of laser scar revision and other related procedures, treatment can be initiated relatively early in the postinjury course. Indeed, this appears to be one of its most promising attributes. In the experience of the authors, AFR and vascular laser treatments can often safely begin within 4 to 12 weeks of severe traumatic injury and may actually help mitigate contractures and pathologic scars when performed judiciously. This is an active area of study, and future large prospective controlled trials are required to confirm these observations, as well as help refine appropriate settings, timing, and treatment combinations.
Fractional Lasers
Among the most notable advances in scar treatment in recent decades is the emergence of AFR. Manstein et al.8 first described the concept of fractional photothermolysis in 2004, wherein emitted light in the mid-infrared (e.g., 1,540 and 1,550 nm) and far-infrared (e.g., 2,940 and 10,600 nm) range induces tissue coagulation or ablation, respectively, in a pixelated pattern through the heating of tissue water.9 Key advancements of the technology include fractionation of the tissue injury to minimize side effects and facilitate subsequent healing, and unprecedented levels of control for the operator to determine the depth and density of treatment. In retrospect it seems this technology was tailor-made for scar revision, affording adaptable and minimally invasive treatments to be applied in the compromised and highly variable setting of scar tissue.
Fostered by the multidisciplinary environment, the rapid influx of patients with serious traumatic injuries, and relatively unfettered by billing issues (see Chapter 25), military dermatologists were among the first to elaborate on the potential for AFR to enhance functional rehabilitation in addition to aesthetic restoration.6,7,10,11,12 Although the application is now beginning to expand rapidly as an emerging standard in burn centers and other venues around the world, AFR has been incorporated routinely into treatment paradigms for trauma patients in a handful of centers, including military centers of excellence, since approximately 2008.6,13,14,15
In the experience of the authors, a course of AFR is associated with consistent and significant improvements in wound healing and scar pliability, texture, and pigmentation. Furthermore, complications such as infection and worsening scarring are extremely rare when AFR is applied judiciously.16 In virtually all cases there is at least some degree of improvement over weeks and months, although the overall impact can vary significantly from patient to patient depending on the clinical scenario. Particularly for the novice, safety is maximized by employing low treatment densities and applying treatments in alternating sessions when using multiple platforms. In the experience of the authors, AFR can be a highly effective adjunct to surgical revision for contractures when applied before, concurrent with, and after surgery.6,7,16,17
The interval between AFR treatments is generally at least 6 to 8 weeks to allow for adequate healing and remodeling. The majority of functional gains are usually realized in the first three to five treatments, whereas texture and dyspigmentation may continue to improve with additional ablative and nonablative fractional treatments. Contractures are usually treated with low (perhaps even the lowest) density and higher pulse energy settings (corresponding with scar thickness), whereas treatments for the enhancement of texture and dyspigmentation alone may be associated with slightly higher density and more moderate pulse energy settings. Actual treatment settings will depend on the specific platform and its associated characteristics such as microcolumn diameter, pulse duration, and available treatment depth. For ablative fractional treatments the authors favor a narrow column width (≤400 µm) and shorter pulse duration (<1 ms) to help avoid excessive thermal injury. Density settings are rarely above 10% for ablative treatments, and are frequently lower when using higher pulse energy settings.
Vascular Lasers
Erythema is a frequent finding early in the process of scar formation, and can also be a helpful indicator of persistent inflammation and an incipient pathologic scar with associated symptoms such as pain and itch. Vascular-specific lasers and light devices target hemoglobin to induce moderate vascular injury and subsequent remodeling. The 585 and 595 nm PDL is the most studied, with more than two decades of use for various scar types.18,19 Other devices that target hemoglobin absorption peaks such as the 532 nm potassium titanyl phosphate laser and intense-pulsed light can also offer benefit.20 In the experience of the authors, PDL and other vascular devices can be very helpful in reducing pain and itch in large erythematous traumatic scars, such as after burns. It is extremely common to use both fractional and vascular devices in the same patient in the same or alternating treatment sessions, adjusting the treatment approach during the maturation and remodeling process.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


