Although children are certainly not “just little adults,” the paradigm for treating pediatric scars is mostly extrapolated directly from the adult experience.
The adage of “use it or lose it” suggests that early intervention may be crucial when scars compromise physical, psychological, or social development.
Emerging technologies such as ablative and nonablative fractionated lasers have revolutionized the treatment and mitigation of pediatric scars, with objective evidence supporting the case for coverage by insurance companies.
A multimodal, multidisciplinary approach will likely prove the most successful paradigm for treating pediatric scars.
Well-controlled, randomized, prospective studies comparing the safety and efficacy of scar treatments are lacking in the pediatric population, representing a tremendous opportunity for basic, translational, and clinical research.
Treating even a single child’s scar can improve the outlook of both the patient and the provider in ways neither of them might have ever imagined; do not be afraid to ask your pediatric patients about their scars and what they mean to them!
during the first year of life, changes in barrier function also continue to develop during this time.6 For example, TEWL is often used as a marker of skin barrier function. In infants, the stratum corneum contains higher water content but is also prone to increased TEWL compared to adults.2,6 Premature infants have an even higher rate of TEWL compared to full-term infants and adults.8 This predisposition puts infants at greater risk for dehydration and electrolyte imbalance than adults.9
Table 22-1 Some Percutaneous Toxicity Risks in the Pediatric Population | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
 FIGURE 22-1 Atrophic scar following flap reconstruction. This patient suffered tissue injury and loss secondary to a motor scooter accident. Flap reconstruction successfully filled the tissue defect, but was associated with atrophy and contour irregularity at the distal aspect of the flap. (Courtesy of Andrew C. Krakowski, MD.) |
 FIGURE 22-2 Hot iron burn. This adolescent male severely burned his hand at 1½ years of age. Split-thickness skin grafts were placed on his palm; predictably, a degree of contraction postreconstruction limited his overall function. The patient’s main stated concern was that he wanted “to be able to open a jar of peanut butter” without his mother knowing. (Courtesy of Andrew C. Krakowski, MD.) |
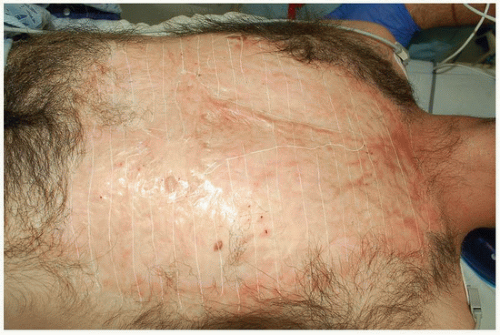 FIGURE 22-3 Large scald burn. This male in his 20s presented with a large burn scar secondary to a scald injury. Note the extensive area of alopecia. Objective evaluation of the scarred areas was performed using high-definition ultrasound, revealing that the majority of the “scar sheet” was approximately 1.5 mm in thickness, with focal areas up to 8 mm. A “grid” pattern was then created over the entire scar sheet using a white surgical marker to help delineate the treatment plan for ablative fractional CO2 laser resurfacing. (Courtesy of Andrew C. Krakowski, MD.) |
involved in the management plan from the start so that realistic expectations may be established. Payers must also be involved from the beginning, understanding that the right people performing the right treatments will yield the best, most cost-effective results.
Table 22-2 Differential Diagnosis for Atrophic Scarring | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
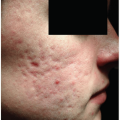
 FIGURE 22-4 Severe inflammatory acne frequently leads to atrophic scarring. The notion that an inflammatory skin condition such as acne vulgaris, with the potential to inflict permanent physical disfigurement and psychosocial distress, is “just cosmetic” is antiquated and ignorant. A primary clinical goal of acne vulgaris management should be scar prevention; too many adolescents have been left branded with permanent reminders of missed treatment opportunities. We must evolve our thinking in order to help prevent scars before they form. Ultimately, this is the most efficacious and cost-effective scar intervention we have available today, and insurance reimbursement should reflect this reality. (Courtesy of Andrew C. Krakowski, MD.) |
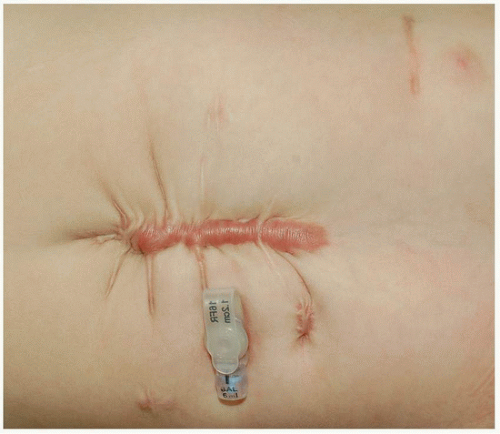 FIGURE 22-5 Iatrogenic hypertrophic scar with scar contractures. This infant with Rubinstein-Taybi syndrome developed a hypertrophic scar after abdominal surgery. The scar itself was pruritic and erythematous. The tension on the wound resulted in multiple “radiating” scar contractures. (Courtesy of Andrew C. Krakowski, MD.) |
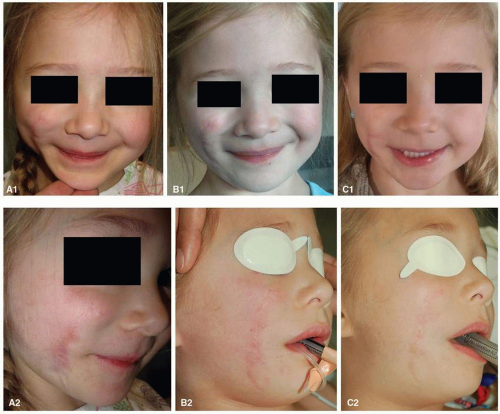 FIGURE 22-6 Multimodal, multidisciplinary treatment of a dog bite scar on the face. A 3-year-old girl presented with a “mixed” (i.e., atrophic and hypertrophic) scar resulting from a dog bite to the right cheek inflicted 21 months earlier. Marked erythema, irregular texture, volume loss, and scar contractures are noted (A1, A2). A total of nine multimodal revision procedures were performed (under general anesthesia because of her age and the extent and location of her injuries). Erythematous portions of the scar were first treated with a 595-nm pulsed dye laser (Vbeam Perfecta, Candela Corporation, Wayland, MA, USA) using a 7-mm spot size, fluence of 8 J per cm2, and 1.5-ms pulse width (clinical endpoint of minimal purpura). The entire scar sheet was then treated using an ablative microfractionated 10,600-nm CO2 laser (UltraPulse, Deep FX; Lumenis, Ltd., Yokneam, Israel) at pulse energy of 15 mJ and density of 15% in a single pass. At the time of her first laser scar revision, the patient’s plastic surgery team performed autologous fat grafting (5 mL) under the depressed scar to help restore volume to her cheek. Serial pulsed dye laser treatments were repeated with fluence settings ranging from 8 to 11 J per cm2 to reach a clinical endpoint of minimal purpura. Additional ablative fractional laser resurfacing treatments were performed with pulse energies ranging from 15 to 25 mJ and corresponding treatment densities of 10% to 5%, respectively. During four early treatment sessions, the patient received triamcinolone acetonide suspension (40 mg per mL) applied topically to the areas of greatest scar hypertrophy immediately after fractional laser treatment. B1 and B2: interim results approximately 10 months after her initial treatment session. C1 and C2: the same patient approximately 19 months after her initial treatment. Marked improvements in scar texture, color, and facial symmetry are noted. Additional enhancements could likely be obtained with repeated interventions such as ablative and nonablative fractional resurfacing and fat grafting. (Admani S, Gertner JW, Gosman A et al. Multidisciplinary, multimodal approach for a child with a traumatic facial scar. Semin Cutan Med Surg. 2015;34:24-27.) |
 FIGURE 22-7 Contracted split-thickness skin graft and amputation. This 3-year-old boy survived meningococcemia but his body was left ravaged by associated necrosis. He lost several fingers and numerous split-thickness skin grafts were necessary during reconstruction. Unfortunately, many of the skin grafts contracted and caused additional functional deficits. Such a complicated presentation highlights the need for a truly specialized, multidisciplinary scar team that might include the patient’s primary pediatrician (the “quarterback”); infectious disease, orthopedics, plastic surgery, dermatology, nutrition, behavior therapy, psychology specialists, and a patient advocate. (Courtesy of Andrew C. Krakowski, MD.) |
Table 22-3 Physical Scar Signs and Symptoms to Consider | ||
|---|---|---|
|
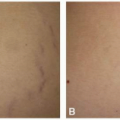
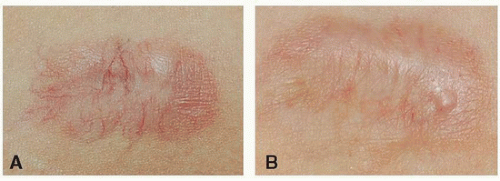 FIGURE 22-8 Tracheostomy scar with prominent telangiectasia. A: This adolescent female’s tracheostomy scar was particularly conspicuous secondary to prominent telangiectases. B: A single treatment with a vascular-specific laser successfully reduced erythema and improved cosmesis, and had the overall effect of reducing the patient’s anxiety levels and enhancing her ability for social interaction. (Courtesy of Andrew C. Krakowski, MD.) |
later, the sensation of being “stuck with an ice pick” within the deep portions of a resulting hypertrophic scar on his arm wakes him from sleep on a near-monthly basis.
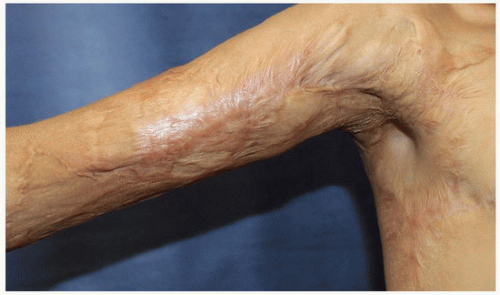 FIGURE 22-9 Scar contracture with functional deficit. This teenage male suffered a gasoline burn injury that resulted in a large hypertrophic scar contracture with the resulting inability to fully abduct his right arm. (Courtesy of Andrew C. Krakowski, MD.) |
treating physicians to assess for psychosocial comorbidities when evaluating a patient with scars and, when present, refer for early intervention.
Table 22-4 Psychosocial Scar Comorbidities to Consider | ||
|---|---|---|
|
 FIGURE 22-10 Chronic wound associated with a burn scar. A: As an infant, this 8-year-old girl had climbed into a bathtub full of hot water and liquid bleach, suffering burns to all four extremities with subsequent associated scar contractures. In one “hot spot” she developed a chronic ulcerated wound that had been present for 8 months despite ongoing traditional wound care. B: One treatment with an ablative, microfractionated 10,600-nm CO2 laser (UltraPulse Deep FX, Lumenis, Ltd., Yokneam, Israel) over the wound and associated contracture bands at pulse energy of 50 mJ and treatment density of 5% helped to stimulate remodeling and relieve the tension on the skin adjacent to the wound, facilitating rapid healing. (Adapted from Krakowski AC, Diaz L, Admani S, et al. Healing of chronic wounds with adjunctive ablative fractional laser resurfacing in two pediatric patients. Lasers Surg Med. 2016;48:166-169.) |
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


