9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
Moustapha Hamdi and Assaf Zeltzer
The microsurgical era evolved from Tansini’s work on the pedicled latissimus dorsi (LD) musculocutaneous flap, which has since been a workhorse in reconstructive surgery.1 It is used extensively as a local flap and as a free flap, providing a large vascularized muscle with or without an overlying skin paddle. The bulk of the flap can be augmented by harvesting it with the surrounding subfascial fat attached to the flap (the extended LD flap), which can especially be useful when dealing with largesize breast reconstructions.2 The LD flap is the widest muscle in the human body accounting for extension, adduction, transverse extension (also known as horizontal abduction), flexion from an extended position, and internal rotation of the shoulder joint. It also has a synergistic role in extension and lateral flexion of the lumbar spine. Although harvesting this muscle is safe and technically reliable, the donor-site morbidity is not negligible. First, muscle function is lost and has to be taken over by the surrounding muscles. Most patients can function well after a LD muscle harvest but have long-term weakness and in some cases pain at the ipsilateral shoulder.3,4 Second, almost all patients have a contour deformity at the donor site, which can be highly visible in lean patients. Third, seroma formation at the donor site is a major issue, and considerable attention has been paid to avoiding or reducing it.5,6
This long era of sacrificing muscle in reconstructive surgery has finally given way to Taylor’s angiosome theory of perforator flaps.7 Perforator flaps have been one of the major breakthroughs in reconstructive surgery, since the first description of an inferior epigastric artery skin flap without the rectus abdominis muscle in 1989 by Koshima and Soeda.8 The advantages of perforator flaps have been widely described and proven, and they all are a direct consequence of the principle of sparing the underlying muscle with its motor innervation when harvesting the flap.9
In 1995, Angrigiani et al first described the thoracodorsal artery perforator (TDAP) flap as a free flap transferred for cervical burn contracture.10 Allen et al11 presented the TDAP flap for breast reconstruction in 1996. Hamdi et al12 elaborated on pedicled TDAP flaps for breast reconstruction in 2004. As with other perforator flaps, the TDAP flap consists of harvesting a skin paddle with underlying fatty tissue, on a constantly vascularized pedicle, while the underlying LD muscle with its motor innervation is spared. Other flaps have been described in the lateral thoracic region to cover a locoregional defect, such as the intercostal artery perforator (ICAP) flap.13
The lateral intercostal artery perforator (LICAP) flap is a good alternative for the TDAP flap for the reconstruction of lateral and inferior defects of the breast. The first description of the lateral intercostal fasciocutaneous flap was by Badran et al14 in 1984, although the use of a flap based on the intercostal neurovascular bundle had already been described in the 1930s.
This chapter describes the anatomy, surgical technique, flap classifications, and clinical indications of the pedicled perforator flap for breast reconstruction.
Regional Anatomyz
The LD and TDAP flap are both based on a reliable and constantly vascularized pedicle that has been widely studied.15–17
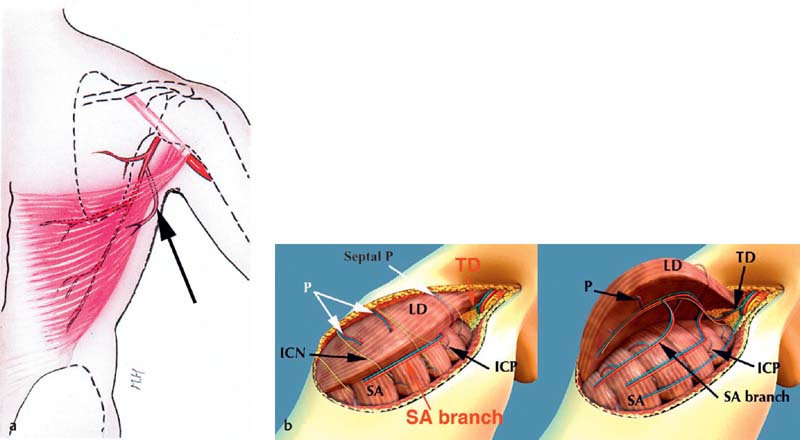
The major vascular axis supplying the TDAP flap is the same that supplies the LD muscle, namely the thoracodorsal (TD) vessels; the medial and inferior portions of the muscle get its vascular supply from intercostal and paraspinal perforators. After originating from the subscapular vessels, the TD vessels course toward the LD muscle. On reaching the deep surface of the muscle, the TD vessels most commonly divide into two primary muscular branches: the transverse branch and the lateral or vertical branch ( Fig. 9.1a ). These branches usually diverge at near 45-degree angles to one another. Both travel from the deep surface of the muscle to become intramuscular. The lateral branch courses vertically and at 2 to 3 cm inside the lateral border of the LD. The TD vessel supplies the muscle by its course in the muscle (parallel to its fibers), and supplies the overlying skin by perforators coursing from the TD vessels perpendicularly to the skin surface ( Fig. 9.1b ). The first perforator is located 6 to 8 cm below the posterior axillary fold and may either be a branch of the distal main TD or arise from its lateral branch. Subsequent perforators, up to a total of three, arise at 1.5- to 4-cm intervals inferiorly off the lateral branch. The first and second perforators are found in most people.18 Each perforator displays a 3- to 5-cm oblique course through the substance of the muscle, giving off numerous muscular branches before penetrating through the dorsal thoracic fascia to supply the overlying skin and subcutaneous fat layers. Each perforating artery is 0.3 to 0.6 mm in diameter and accompanied by two venae comitantes. Heitmann et al19 described two rows of perforators arising from the main pedicle at the lateral border of the LD muscle. The lateral row does not pierce the muscle and provides for the direct TDAP perforators ( Fig. 9.1 ). The medial row of perforators courses through the muscle (perforating it) before reaching the skin and subcutaneous tissues.
Various musculocutaneous flaps described by Kerrigan and Daniel20 can be harvested based on these intercostal vessels. The intercostal vessels form an arcade, between the aorta and the internal mammary vessels, which gives off numerous perforators on which a flap can be designed. Based on the concept of freestyle flap,21 ICAP flaps can be harvested to cover defects that extend on the trunk from the lower neck to lower abdomen and lumbosacral area.
There are four segments of the intercostal vessels: vertebral, intercostal, intermuscular, and rectus ( Fig. 9.2 ). The ICAP flaps are classified as follows ( Fig. 9.2b):
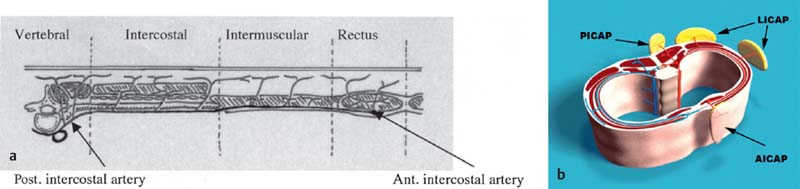
The posterior intercostal artery perforator (PICAP) flap, based on perforators originating from the vertebral segment of the intercostal vessels
The lateral intercostal artery perforator (LICAP) flap, based on perforators arising from the intercostal segment
The anterior intercostal artery perforator (AICAP) flap, the nutrient perforators of which arise from the muscular or rectus segment
The intercostal segment, which is the longest (12 cm), is very important because it gives off five to seven musculocutaneous perforators, on which flaps can be designed and raised.
The LICAP perforators are found 1 to 3.5 cm anterior to the anterior border of the LD muscle.22 The largest perforator is most frequently found at the level of the sixth intercostal space (generally between the fourth and eighth intercostal space). The flap can also be harvested with an intercostal nerve, making it sensate.
The serratus anterior artery perforator (SAAP flap) is based on a connection between the thoracodorsal artery branch to the serratus anterior muscle and the intercostal perforators. It is not a constant perforator and is found in only 20% of cases. When an appropriately sized perforator is identified in front of the anterior border of the LD, it can be followed back to the nutrient artery (which in this case is the serratus anterior branch) by dissecting the pedicle within the fascia and the fibers of the aforementioned muscle.
Indications and Clinical Applications of Pedicled Lateral Thoracic Flaps
The TDAP flap has a wide range of indications as a local flap (pedicled) as does its equivalent muscle flap (LD muscle flap). Most patients who could benefit from a ped- icled LD flap are good candidates for a TDAP flap. The flap is ideally used for lateral and anterolateral defects of the thorax, and it has an important place in the reconstruction of lateral defects of the breast in partial breast reconstruction both in a primary and in a secondary setting. With the TDAP flap, defects of the two lateral quadrants of the breast can easily be reached. The medial quadrants can sometimes be reached when harvesting a flap that is long enough, but defects of the inferomedial quadrant are difficult to reach with a TDAP flap and are better reconstructed in a different manner.23 The flap is also useful in implant breast reconstruction for extra coverage of the device without sacrifice of the muscle or as an autoaug- mentation flap in post-bariatric surgery patients.24,25
The local flap also has applications in the reconstruction of the axilla, shoulder, and upper arm.
The LICAP flap has its main use as a pedicled flap for lateral thoracic defects, superolateral abdominal defects, axillary defects, and supero- or inferolateral breast defects, for which it is most commonly used.
When used as a pedicled flap, dissection of the perforator must be performed far enough to be able to rotate the flap. Dissection in the costal groove is only necessary when harvesting the flap for a free tissue transfer so as to have a longer pedicle with greater diameter of the vessels.
The LICAP flap can also be used for patients after massive weight loss who want to get rid of excessive tissue over the lateral thorax. When performing a mastopexy in these patients, this excess tissue can be used as a pedicled flap to augment the breast (pedicled flap autoaugmentation). Clearly, LICAP flaps have to be harvested bilaterally in these cases.26
The indications for the use of lateral thoracic pedicled perforator flaps are as follows:
Immediate/delayed partial breast reconstruction
Coverage of thoracic defects after radical excision
Postmastectomy breast reconstruction (with or without and implant)
Salvage of major fat necrosis after previous autologous reconstruction
Autologous breast augmentation (aesthetic, postbariatric surgery)
Surface Anatomy and Flap Design
Thoracodorsal Artery Perforator Flap
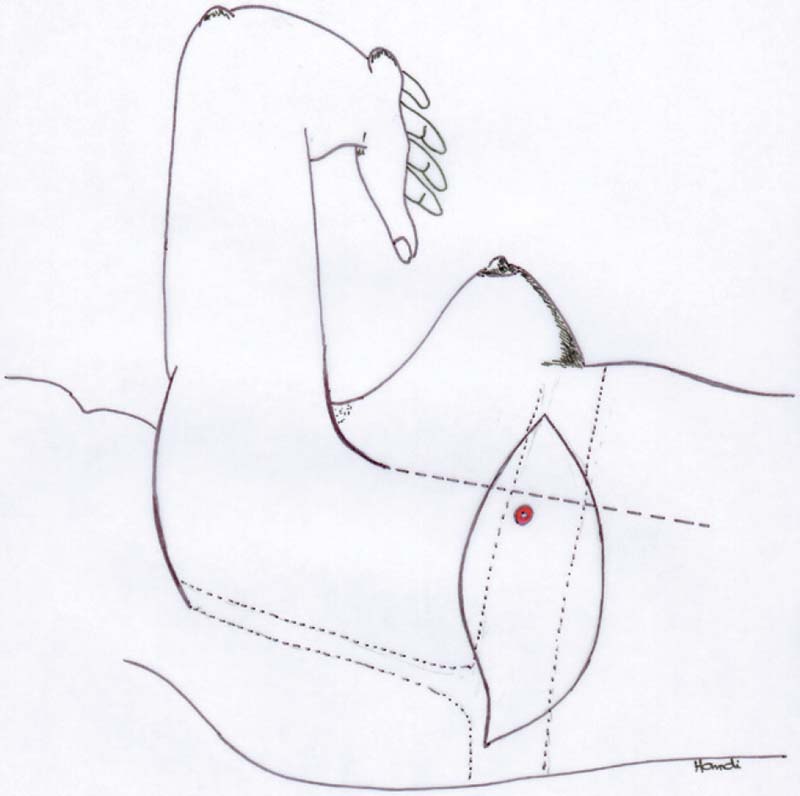
Patients are marked in the standing position before anesthesia for breast surgery. The breast with the defect to reconstruct is marked. The patient is the placed in the lateral decubitus position with the arm abducted 90 degrees from the thorax and the elbow flexed 90 degrees ( Fig. 9.3 ). The anterior border of the LD muscle is palpated and marked on the skin. As discussed above, most perforators are found at 8 to 10 cm from the axilla and within 3 cm of the anterior muscle border. At the presumed site of the perforators, a handheld Doppler device is used to identify the exact position of the perforating vessels. More recently, computed tomography (CT) and magnetic resonance imaging (MRI) have been used to preoperatively determine the position of the perforators on the skin.27,28
Once the perforator mapping is done, depending on the reconstructive needs, the flap can be designed on the skin. The flap should always extend anteriorly to the anterior muscle edge to be sure to include the vascular hilus. The skin paddle can be designed in every possible direction on a perforator. The vertical design facilitates incorporating good perforators in the flap. When used as pedicled flaps (mostly for breast reconstruction), the design should be done in a horizontal fashion (in the line of the bra) to better hide the scar in the bra, with the scar following the skin lines. This orientation (following the direction of the ribs) also makes it possible to harvest the largest reliable flap possible on a single perforator, in accordance with Taylor’s29 angiosome theory. The actual size of the flap is mostly limited by the requirements for primary closure of the donor defect. Flaps as big as 14 x 25 cm have been raised on a single perforator without any significant complications.
Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
 15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


