15 Deep Circumflex Iliac Artery Perforator Flap for Breast Reconstruction
Edward Buchel
Autologous breast reconstruction using abdomen-based perforator flaps continues to be a highly successful means of reconstructing partial and complete breast defects. Much has been learned about the perfusion characteristics associated with the deep inferior epigastric perforator (DIEP) flap and the superficial inferior epigastric artery (SIEA) flaps. The SIEA flap routinely perfuses an ipsilateral hemiabdomen, whereas the DIEP flap reliably perfuses the ipsilateral and occasionally portions of the contralateral anterior abdominal tissue. Neither reliably perfuses tissue posterior to the anterior axillary line. This tissue, the flanks or “love handle” area, is frequently abundant and in fact is one of the most common areas of the trunk that undergoes secondary revision surgical contouring after abdomen-based breast reconstruction (“dog-ear” excision). This flank tissue is of significant value, either on its own or in conjunction with the anterior abdominal wall, for patients in whom the anterior abdominal wall has been already harvested, or the volume of tissue is inadequate for breast volume replacement, respectively. The deep circumflex iliac artery perforator perfuses lateral abdominal and hip tissue reliably and has proven to be an excellent adjunct to abdomen-based perforator breast reconstruction. Secondarily, it further improves the abdominal aesthetics by contouring the flanks as an extended “dog-ear” excision.
Anatomy
Taylor et al1 first described the deep circumflex iliac artery (DCIA) as the supply for the groin flap in 1979. The preliminary reports documented an arterial diameter greater the 2 mm at the origin of the external iliac just lateral to the deep inferior epigastric artery. It reliably has two venae traveling with it varying in size from 1.5 to 2.5 mm. Starting from the external iliac artery origin, the artery travels laterally along the medial surface of the ilium and then superficially where it pierces the transversalis fascia. At this position it gives off musculocutaneous perforators and nutrient perforators to the iliac crest. At a point just superior and lateral to the anterior superior iliac spine (ASIS), the DCIA frequently gives off an ascending branch supplying the inferior lateral peritoneum and muscle of the abdominal wall.2 The pedicle then continues as the lateral branch, supplying the iliac crest and the overlying skin after piercing the internal and external oblique muscles. In most cases the vascular bundle travels for 1 to 2 cm obliquely between the muscle layers before piercing the next most superficial muscle layer. The main perforator artery has an average diameter of 0.7 mm with an average of 1.6 DCIA perforators found on cadaveric injection studies.3 Perforators were located 5 to 11 cm posterior to the ASIS, and 1 to 35 mm superior to the iliac crest, resulting in a perforator zone of 31 cm.3 In clinical cases the dominant perforator has been found 1 to 2 cm superior and 1 to 4 cm lateral to the ASIS. The skin territory reliably supplied is superior to the iliac crest for 10 to 15 cm, and 10 to 15 cm horizontally in each direction from the entry point of the perforator into the flap.
Indications
Anterior abdominal wall tissue is always the first choice when considering autologous breast reconstruction. When the anterior abdomen tissue does not provide sufficient volume or has been previously resected, the flank tissue should be considered. Tissue lateral to the ASIS and superior to the iliac crest typically has thicker associated fat than is appreciated at first. Skin laxity on the flanks is variable, and will determine the maximum width of the flap that can be harvested and still allow for easy closure of the donor site. In general, the DCIA perforator flap is harvested alone when the anterior abdominal tissue has been previously resected, and as a combined flap with the ipsilateral DIEP or SIEA when a traditional hemiabdomen flap provides insufficient volume. In both situations, the donor site needs to be assessed to ensure that it has adequate fat and skin laxity. Closure of the donor site can provide a markedly improved abdominal contour, especially around the waist, but aggressive flap harvest can present difficulties in wound closure and prolonged wound healing. In general, the maximum vertical harvest dimensions of the DCIA flap are determined in the same way as they would be for a body-lift cosmetic procedure. Thus, the donor-site closure will result in a similarly improved aesthetic result.
Technique
Markings
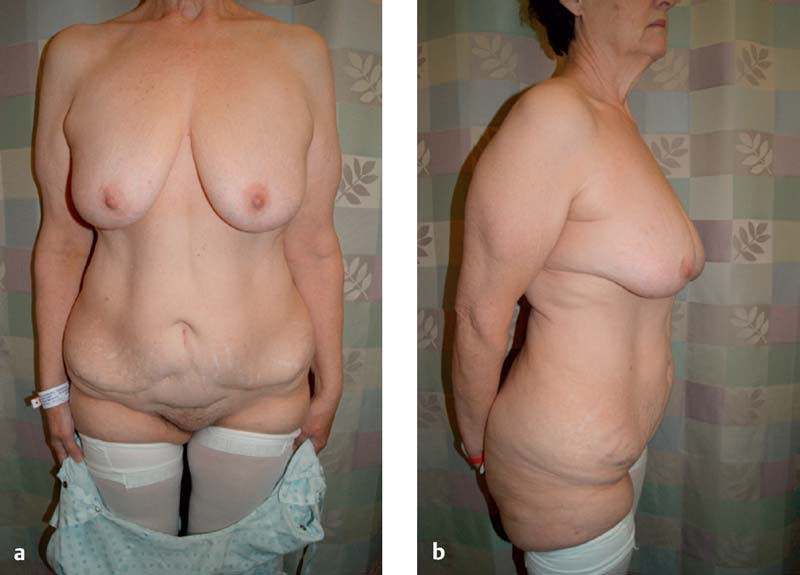
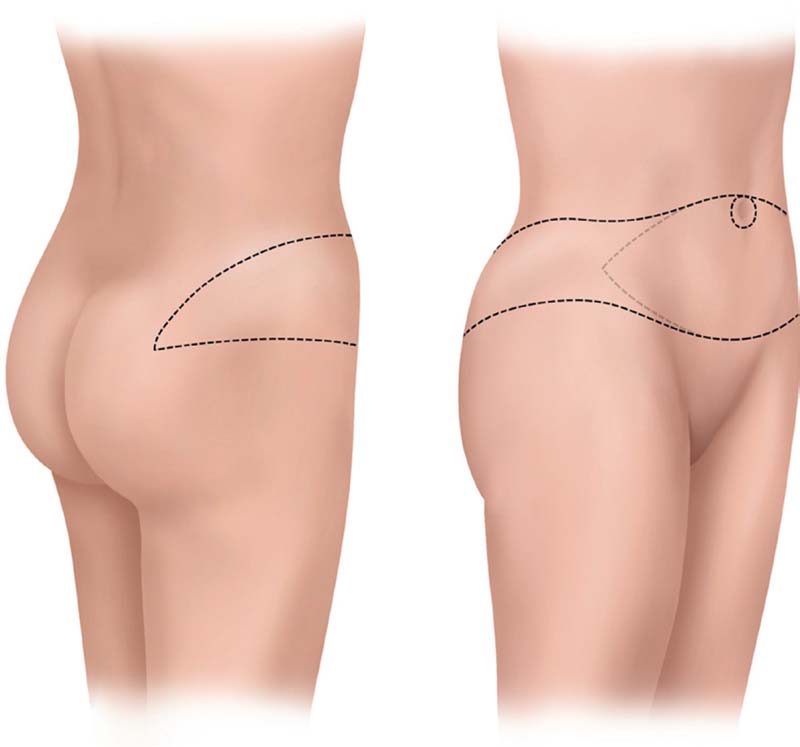
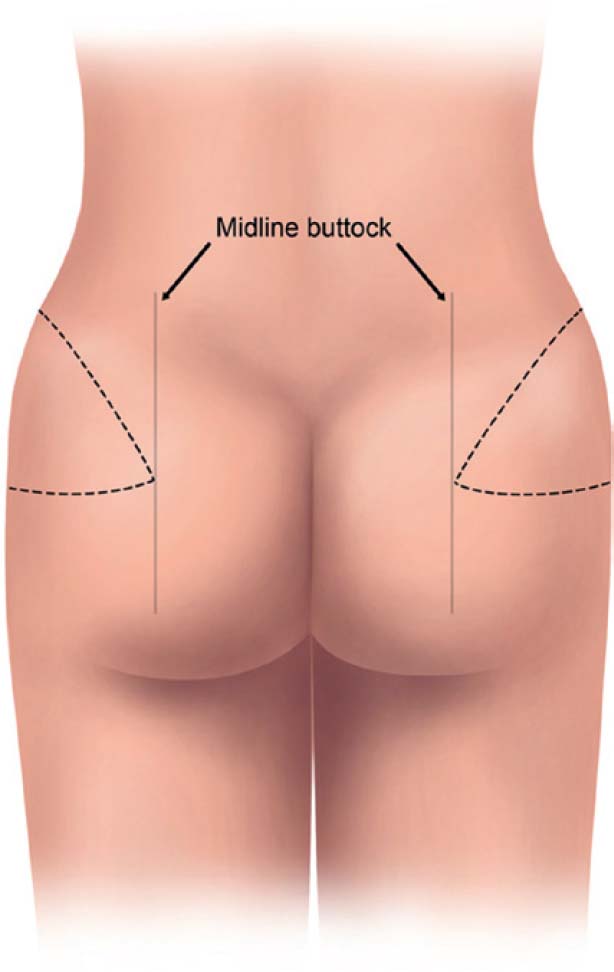
The DCIA flap is designed to be centered on the DCIA perforator. The use of the DCIA flap by itself or in conjunction with the DIEP or SIEA flap will determine the harvesting dimensions on the anterior abdominal wall. If the DCIA is used by itself, as is the case when the anterior abdominal wall has been resected previously ( Fig. 15.1 ), an inferior horizontal skin mark is made just lateral to the ASIS, extending posteriorly to include the excess tissue, or “dog ear.” The corresponding superior horizontal skin mark is made by pinching the skin at this level to determine the maximum amount of excess skin that can be harvested. This will define the dimensions of the DCIA flap. The DCIA perforator will be located just superior and lateral to the ASIS ( Fig. 15.2 ). The upper and lower incision lines are brought together posteriorly at a point just lateral to the mid-buttock line ( Fig. 15.3 ).
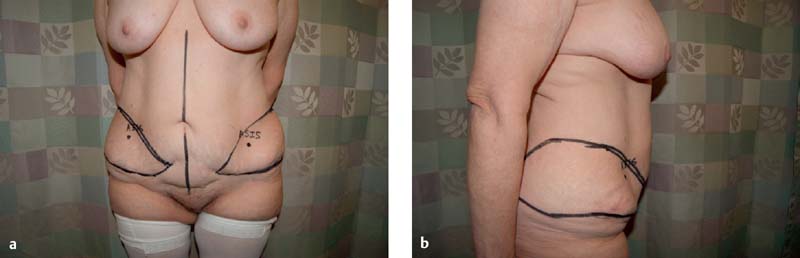

When harvesting a combined DCIA-DIEP or DCIA-SIEA flap, the markings for a standard DIEP or SIEA flap are done first. Then using these markings the DCIA flap markings are superimposed on them. As such the inferior markings of the DIEP-SIEA flap are treated as the prior abdominal wall scar as described above ( Fig. 15.4 ). Posterior markings are the same as for a single DCIA flap without the anterior abdominal included ( Fig. 15.5 ).
Related posts:
 2 Starting a Perforator Flap Breast Program
2 Starting a Perforator Flap Breast Program
 4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
4 Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
 10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
10 Bipedicled (Double or Stacked) Abdominal Perforator Flap in Unilateral Breast Reconstruction
 9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
9 Pedicled Lateral Thoracic Flap for Breast Reconstruction
 13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
13 Lateral Thigh Perforator Flap (Septocutaneous Tensor Fasciae Latae Perforator Flap)
 11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
11 Venous Salvage Procedures in the Deep Inferior Epigastric Perforator Flap for Breast Reconstruction
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


